Vaginitis and balanitis are nonspecific terms that refer to inflammation of the vagina or the glans penis. Because these epithelial surfaces are variably moist (in men, depending on the presence or absence of the prepuce), the clinical manifestations of common diseases are often altered, and diseases unique to warm, wet areas may occur.
VAGINITIS
Although cutaneous innervation within the vagina has a limited capacity to transmit pain, vaginal inflammation is often very symptomatic. Irritating or infected vaginal secretions drain onto the vulva, which is exquisitely sensitive to sensations of burning, irritation, stinging, and itching. Copious or irritating vaginal secretions produce irritant contact dermatitis of the vestibule and sometimes a larger area of the modified mucous membrane (Fig. 15-1).
Nonneoplastic vaginal abnormalities can be classified into one of the two overlapping categories: vaginitis or vaginosis. Vaginitis is characterized by signs of inflammation, such as redness and vaginal secretions containing an increase in leukocytes. Vaginosis is characterized by abnormalities unaccompanied by erythema or a purulent vaginal discharge. An example is bacterial vaginosis, in which signs and symptoms of inflammation are notably absent. However, not all instances of Candida vaginitis are accompanied by visible erythema or an increase in white blood cells. In addition, patients with cytolytic vaginosis and Lactobacillus vaginosis characteristically report symptoms of inflammation, particularly itching.
Before the vagina and vaginal secretions can be evaluated, the examiner must be aware of the appearance of normal vaginal epithelium and normal vaginal secretions (see Chapter 3). The normal premenopausal but postmenarchal vagina is pink and wet, with prominent folds, or rugae. Prepubertal girls and postmenopausal women exhibit pale, smooth vaginal epithelium with a loss of these rugae.
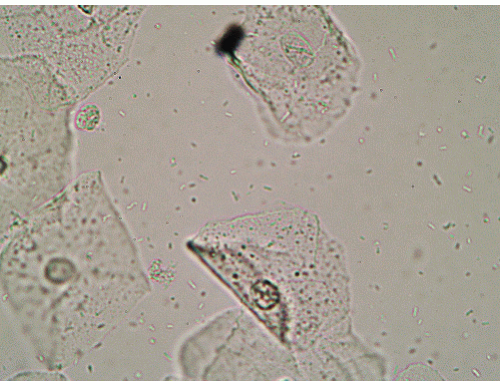
The normal vaginal secretions of a well-estrogenized woman are notable for three obvious characteristics (Fig. 15-2). First, desquamated epithelial cells are mature, shed from a resilient, normally thickened epithelium. These cells are large and flat with a small nucleus and crisp borders that are often folded to reveal the flattened nature of the cell. Second, abundant lactobacilli are present, providing an acid pH lower than 5. Finally, the presence of white blood cells is expected, but white blood cells should not greatly outnumber epithelial cells.
Infectious Vaginal Disease
Most clinicians presume the term vaginitis to be synonymous with infection. In fact, many clinicians oversimplify further and expect all vulvovaginal symptoms, especially when accompanied by abnormal secretions, to be caused by yeast, Trichomonas, or bacterial vaginosis. Certainly, these are the most common, striking, or easily diagnosable forms of vaginitis, but other less well-described processes also occur.
Candida Vaginitis
Candida vaginitis, particularly that produced by Candida albicans, is extremely common. It also generally takes the initial blame for any vulvovaginal itching or burning, whether or not yeast actually is identified on microscopic smears or cultures. At least half of patients referred to specialty clinics for chronic or recurrent candidiasis actually experience symptoms on the basis of another process.
Clinical Presentation Itching is the usual presentation of vaginitis caused by C. albicans and C. tropicalis. Chronic infection or colonization with C. albicans produces irritation or burning in a much smaller subset of women. Although C. albicans vaginitis classically is accompanied by a white, clumped, cottage cheese-like discharge that is often not particularly copious, vaginal secretions often appear normal clinically. Vestibular erythema is usual, and some patients develop more extensive erythema, skin-fold fissures, and scale, as well as peripheral satellite pustules, erosions, or collarettes (Fig. 15-3).
Vaginitis produced by non-albicans yeast, including C. glabrata, C. parapsilosis, C. krusei, and Saccharomyces cerevisiae, are most often asymptomatic. When vaginal cultures were performed in 223 symptomatic and asymptomatic women, 17% of cultures positive for yeast in asymptomatic women showed C. glabrata, whereas 4% of cultures in symptomatic women showed C. glabrata (1). When symptoms occur, women generally report irritation and burning more than itching. Vaginal secretions are clinically unremarkable, and microscopically show subtle budding yeasts without hyphae or pseudohyphae. Vulvar manifestations are limited to vestibular erythema or no objective abnormalities; scaling, fissuring, and satellite pustules do not occur.
FIG. 15-1. The symptoms of vaginitis often occur as a result of contact dermatitis from irritating vaginal secretions that inflame the introitus and modified mucous membranes of the vulva. This is manifested by nonspecific redness and edema, so that the cause of the vaginitis often cannot be ascertained from the appearance of the vulva.
Diagnosis The diagnosis of a C. albicans infection requires identification of the organism on a microscopic examination of vaginal secretions. This can be achieved by an experienced examiner on a microscopic smear. However, the ease of this examination is generally underestimated by the nondermatologist; when the index of suspicion is high but a smear is negative, or a smear is positive but the patient does not improve as expected, a vaginal culture should be performed.
FIG. 15-2. Normal vaginal secretions exhibit large, flattened and folded mature squamous epithelial cells, one or fewer white blood cells for each epithelial cell, and abundant lactobacilli.
FIG. 15-3. Vaginal candidiasis frequently secondarily infects the vulva, and this redness, fissuring, and shininess are characteristic.
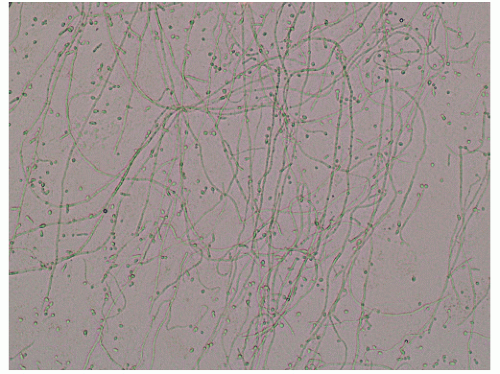
The identification of non-albicans Candida on microscopic smear is much more difficult. Only C. albicans and C. tropicalis exhibit hyphae, pseudohyphae, and budding yeasts that are normally seen with the 10× objective (Fig. 15-4). Non-albicans Candida infections reveal only tiny, budding yeasts that can be seen best with the 40× objective (Figs. 15-5 and 15-6). However, a non-albicans Candida infection usually exhibits multiple budding yeasts, so nearly every field shows at least one yeast form. The presence of non-albicans Candida is best evaluated on a saline preparation rather than a smear treated with potassium hydroxide. Debris from the lysis of cells by potassium hydroxide can obscure the small budding yeasts.
FIG. 15-4. Vaginal secretions of candidiasis exhibit branching pseudohyphae and tiny, budding yeasts on a microscopic examination of vaginal secretions.
FIG. 15-5. Wet mounts of vaginal secretions of patients with non-albicans Candida vaginal infection show tiny, budding yeasts seen best with a higher power objective such as 40×. This shows the classic “bowling pin” appearance of C. glabrata.
Biopsies of yeast vaginitis are performed only if the diagnosis is not suspected by the clinician, because less expensive and painful methods of diagnosis are usual. However, a typical tissue sample of acute vaginal candidiasis reveals inflammation consisting primarily of lymphocytes with some plasma cells and neutrophils, with stromal edema and spongiosis. Fungal elements are often seen within the most superficial portions of the vaginal epithelium. Less inflammation is seen in chronic candidiasis.
C. albicans vaginitis often coexists with, precipitates, and drives eczema. Therefore, C. albicans vaginitis should be considered in the differential diagnosis of eczema or any other itchy vulvovaginal disease. Vulvar psoriasis and lichen sclerosus are other itchy dermatoses that are often misdiagnosed as Candida vaginitis.
FIG. 15-6. The very round configuration of these yeast buds is characteristic of S. cerevisiae. Although non-albicans Candida yeast forms are harder to identify because there are no mycelia, they generally are distributed throughout the wet mount so the trained eye can identify them fairly quickly.
C. ALBICANS VAGINITIS: Diagnosis
Pruritus, often of the vestibule, occasionally extending to the entire vulva, perianal skin, and crural creases
Changes that range from a normal vulva or vestibular erythema and vaginal redness with vaginitis alone, to generalized redness, peripheral peeling, satellite papules, pustules or collarettes, and fissures when the vulva is affected
Vaginal secretions that range from normal clinically to clumped, “dry” secretions
pH below 5
Wet mount showing hyphae/pseudohyphae/budding yeast
Culture (when recurrent or recalcitrant) revealing C. albicans
FREQUENTLY RECURRENT, OR RECALCITRANT, C. ALBICANS VAGINITIS: Diagnosis
Culture that shows yeast; wet mount and symptoms should be confirmed by culture if patient does not respond
Non-albicans Candida infection tends to produce burning, so the usual diseases considered in the differential diagnosis of vulvodynia should be considered in patients suspected with non-albicans Candida infection. Vulvodynia is a primary condition in the differential diagnosis of this condition, as are erosive dermatoses such as lichen planus, and other vaginal infectious and inflammatory processes should be considered such as desquamative inflammatory vaginitis (DIV).
NON-ALBICANS CANDIDA VAGINITIS: Diagnosis
Usually, no symptoms. Occasionally, irritation, burning, rawness
Normal vulva and vagina
Vaginal secretions that are normal clinically
pH below 5
Wet mount showing budding yeast without hyphae or pseudohyphae
Culture C. glabrata, C. parapsilosis, C. lusitaniae, C. krusei, Saccharomyces cerevisiae, etc.
Pathophysiology The most common cause of vulvovaginal yeast infections is C. albicans, but the proportion of non-albicans Candida is increasing. A study of 223 Australian women showed that of the 21% of women colonized with yeast, 73% were found to have C. albicans (2). In another study, 44.2% exhibited C. albicans, 28% had C. glabrata, and 16.2% had S. cerevisiae (1). Although most physicians in the United States do not find that non-albicans Candida infections represent this large a proportion of all infections, the fact that non-albicans Candida is usually asymptomatic and these organisms are relatively resistant to therapy leads to underdiagnosis. Older women may be more likely to experience non-albicans Candida than younger women (3).
The simple presence of C. albicans does not provide a diagnosis of Candida vaginitis. A recent study showed 21% of normal, asymptomatic women show evidence of vaginal Candida by culture (2). A yeast infection is produced by higher numbers of organisms and an inflammatory response to these organisms. Cutaneous vulvar candidiasis is associated with superficial invasion of the epithelium by yeast.
Several known factors contribute to the development of a yeast infection. Patients who are immunosuppressed by virtue of medication or disease are more likely to develop a symptomatic yeast infection. A common local immunosuppressing medication is a topical corticosteroid. Systemic antibiotic medications also predispose women to Candida vaginitis, and the combination of corticosteroids and antibiotics is especially likely to provoke a yeast infection. Patients with diabetes mellitus are at increased risk of the development of Candida infections, as are pregnant women (4).
TABLE 15.1 Oral medications for vulvovaginal yeast infections
150 mg once for uncomplicated infection; recommended by the Centers for Disease Control and Prevention in weekly dosing for frequently recurrent candidiasis
a All have potential hepatotoxicity, ranging from life-threatening idiosyncratic disease with ketoconazole to only theoretic disease produced by weekly fluconazole. All have potential medication interactions; ketoconazole and itraconazole have the largest number of potential interactions.
b Not approved by the United States Food and Drug Administration for the treatment of vulvovaginal candidaisis, although shown to be very effective. There are several different regimens shown to be effective.
Management There are multiple effective and safe options for treating C. albicans vaginitis. Oral or topical azoles are the most frequently prescribed medications (Table 15-1). A one-time dose of fluconazole 150 mg orally produces the same rate of success as a course of a topical azole. In addition to the convenience and high compliance rate with onedose therapy, this medication has the advantage of avoiding irritation from the alcohols, preservatives, and stabilizers in topical creams, and it also has the advantage of treating both the vulva and vagina simultaneously. The most common side effects are headache, occurring in about 13% of patients (as compared with 7% of those receiving placebo), and nausea, occurring in 7% of patients. Oral ketoconazole is rarely used for this condition now, because of the risk of hepatotoxicity and the availability of fluconazole. Itraconazole is another oral azole that is known to be effective but does not have indication approval for vulvovaginal candidiasis. This medication has the additional disadvantage of several important medication interactions. In addition, both ketoconazole and itraconazole require multiple doses to eradicate vulvovaginal yeast.
Topical azoles are equally beneficial as compared with oral fluconazole and effect symptom control slightly faster. There are multiple similar products available, with dosing ranging from one vaginal suppository (clotrimazole vaginal troche 500 mg) to suppositories or creams inserted daily for 7 days. Advantages include the availability of clotrimazole and miconazole without a prescription and the avoidance of exposure to an oral medication. Generic, over-the-counter preparations are effective and very inexpensive, whereas some prescription topical azoles are the most expensive of all available anticandidal therapies. When significant vulvar candidiasis is present, an anticandidal cream should be applied to the vulva two to four times a day, in addition to the topical vaginal medication, until the skin is clear.
Nystatin is a time-honored therapy for C. albicans infection, but generally it is not used. This medication is less effective than the newer azoles, although its availability in a soothing, ointment base is a distinct advantage for patients with significant inflammation, and I use this regularly in combination with fluconazole for women with prominent vulvar involvement. Nystatin ointment or vaginal tablets are inserted into the vagina daily for 2 weeks. When significant vulvar disease is present, nystatin cream or ointment should be applied to the vulva four times a day until the skin is clear.
Fluconazole 150 mg once (80% cure), may repeat in 1 week if symptoms persist
Any topical azole suppository or cream, per package insert
Topical azole or nystatin twice daily to vulva when needed
FREQUENTLY RECURRENT C. ALBICANS: Management
Fluconazole 150 mg weekly for 3 to 6 months; rarely needed q 3 days (confirm persistent yeast with a culture) or
Vagina azole or boric acid 600 mg per vagina 2 to 3 times a week for 3 to 6 months if fluconazole is contraindicated
May continue longer than 6 months if needed
Probiotic and diet have not been shown beneficial, except diet control for diabetes
Unfortunately, many non-albicans Candida infections, especially those caused by C. glabrata and S. cerevisiae, are unresponsive to azole therapy, including fluconazole, terconazole, and butoconazole, despite in vitro sensitivities that would indicate sensitivity to these medications (4). These yeast forms sometimes are extraordinarily difficult to eradicate (Table 15-2). Although an azole can be tried first for these non-albicans Candida infections, patients should be advised that their infection likely will not clear. The occurrence of resistant non-albicans Candida organisms is related to characteristics of the organism rather than the presence of immunosuppression in the host. However, resistant C. albicans is uncommon except in immunosuppressed patients. Resistance to therapy increases during treatment, so low-dose or intermittent therapy should be avoided.
Before aggressive anticandidal therapy is instituted under the assumption that poor response to therapy is the result of resistance, a fungal vaginal culture should be performed to confirm the diagnosis. Some clinicians also advocate sensitivities, whereas others state that sensitivities are unreliable because they are based on expected concentrations of medication achievable in blood rather than that occurring in the vagina.
An alternative therapy shown to be effective for non-albicans Candida infections resistant to azole is boric acid capsules, which are prescribed by instructing a pharmacist to place 600 mg of boric acid in a gelatin capsule (5). This capsule is inserted in the vagina daily for 2 weeks. Boric acid capsules are irritating in some patients, particularly those who are already irritated by their infection. Most women experience significant improvement but not necessarily cure, with symptoms recurring off therapy, requiring maintenance therapy with boric acid. Nystatin vaginal tablets or ointment are sometimes more beneficial than azoles.
Arguably most effective is intravaginal flucytosine. Fourteen 500-mg capsules of flucytosine are dissolved in 45 g of a hydrophilic cream base, and a 6.4-g vaginal applicator filled with cream is inserted in the vagina daily for a week. This is extremely expensive and many compounding pharmacies will not provide this due to the cost of the medication, which must be bought in large quantities. Pharmalogics, Inc; phone number (248) 552-0070 currently will fill and mail this medication. Resistance occurs quickly.
Amphotericin cream is available commercially and can be inserted daily, but it is sometimes irritating. A compounded 80-mg amphotericin vaginal suppository is less irritating to some patients, but there are no data on the effectiveness of intravaginal amphotericin. There are several recipes for these suppositories, and these are generally available from any compounding pharmacy. I have treated five patients and cleared one of a non-albicans Candida infection. One report described a compounded suppository of amphotericin and flucytosine. Although butoconazole has demonstrated in vitro activity against non-albicans Candida, I have not had success with this medication in the treatment of recalcitrant vulvovaginal non-albicans Candida infections.
Gentian violet is another potent fungicidal substance. Unfortunately, this is also an extreme irritant in some patients, occasionally producing even blisters and erosions. It is also extremely messy. The usual regimen consists of a weekly application of a 1% solution painted on the vaginal walls with a saturated gauze swab. However, to avoid the occasional blistering reaction to a higher concentration of gentian violet, I use a 0.25% solution for the first treatment, followed by 0.5% a few days later, and then 0.75% solution before graduating to a full 1.0% solution. Medication is applied weekly in the office for 4 to 6 weeks, while the patient is maintained on daily topical therapy with nystatin or boric acid.
TABLE 15.2 Therapies for resistant non-albicans Candida vaginal infections
Sometimes irritating, poisonous if ingested orally
Nystatin vaginal tablets or ointment
Insert b.i.d. × 1 month
Inexpensive, nonirritating
Gentian violet
Painting in the office weekly
One of the more effective medications
Can produce erosive contact dermatitis, stains skin and clothing
Flucytosine fourteen 500-mg capsules dissolved in 45 g of hydrophilic cream base
6.4 g inserted hs × 1-2 weeks
Well tolerated, fairly effective
Expensive
Amphotericin suppositories
Insert hs for 2-4 weeks
—
Expensive, can be irritating
Amphotericin/flucytosine vaginal suppositories
Insert hs
—
Expensive, can be irritating
hs, at bedtime.
a All are often ineffective, and often several in sequence or together must be used for the best chance of success.
b All except nystatin are unavailable commercially and must be compounded. Terconazole and butoconazole have been shown in a laboratory setting to exhibit increased activity against non-albicans Candida; this has not been confirmed in patients in published clinical trials, and this author has not found them to be useful.
The average patient with C. albicans vaginitis experiences resolution of symptoms within 2 or 3 days. Immediate recurrence is not usual but it is relatively common. Patients who have had severe vulvovaginal candidiasis can require longer time for their symptoms to resolve, and an occasional patient experiences frequently recurrent yeast infections. When recurrence of C. albicans is documented, further recurrences can be prevented with once weekly dosing of fluconazole 150 mg (6). This medication, in my experience, can be discontinued after several months without recurrence once the skin has completely healed and barrier function has returned. There is evidence, however, that long-term therapy with fluconazole sometimes leads to decreased sensitivity of C. albicans to this medication (7).
The use of probiotics has been a popular means of preventing vulvovaginal yeast for years. Although common wisdom dictates that the presence of lactobacilli protects from vulvovaginal candidiasis, vaginal yeast is rarely seen in those patients who have no lactobacilli; atrophic vagina, bacterial vaginosis. A recent study suggests that numerous lactobacilli on wet mount increase rather than decrease the risk of vulvovaginal candidiasis (8). This has not been confirmed, and there are studies that suggest benefit of lactobacillus therapy, and others that show no benefit (9).
NON-ALBICANS CANDIDA VAGINITIS: Management
Trial of fluconazole 150 mg once; may repeat in 3 days; or, any topical azole suppository or cream, per package insert
Clinical PresentationTrichomonas vaginitis produces extreme itching and irritation. Dysuria and lower abdominal pain are common, and most patients experience a copious yellow or green vaginal discharge.
Bright red erythema of the vestibule is usual on physical examination. The vagina is inflamed also, and the cervix often is red and covered with discrete, punctate, bright red, and hemorrhagic macules and papules, producing the classic but nonspecific “strawberry cervix.” A copious, purulent, frothy vaginal discharge is typical. The vaginal pH is high, as occurs with most extremely inflammatory vaginal diseases and conditions characterized by an absence of lactobacilli.
Trichomonas can occur in men, but it is generally asymptomatic. A purulent urethral discharge occurs in some patients.
Diagnosis This diagnosis is often made easily on a wet mount if it is examined immediately under high power. The presence of trichomonads is often obvious when they are active, but the diagnosis sometimes is more difficult. Trichomonads are approximately the size of a white cell, but these flagellate organisms are teardrop shaped rather than round and they are extremely active, so their motion is not missed easily. However, as trichomonads cool, they lose their characteristic teardrop shape, becoming round and still, making differentiation from white blood cells very difficult. Neutrophils are abundant. However, a recent study showed, compared to cultures, a false negative rate of 36.93% in a group of 200 women, with no false positives (10). A similar study shows 81% to 85% sensitivity of the diagnosis on wet mount as compared to diagnosis with a DNA probe (11). Therefore, when there is a high index of suspicion, cultures or DNA probes are indicated in the absence of a positive wet mount. There are no specific histologic findings on biopsy.
Trichomonads are sometimes reported on Papanicolaou smears. Although the accuracy of this is dependent on the individual examiner, some series show good correlation of this report with the presence of trichomoniasis (12,13).
The differential diagnosis of Trichomonas vaginitis includes all causes of a purulent vaginitis, including DIV and inflammation associated with an atrophic vaginal epithelium, an intravaginal foreign body, or any erosive vaginal skin disease.
Pathophysiology Trichomoniasis is caused by the protozoan Trichomonas vaginalis. This disease is always sexually transmitted. The vagina is the primary area of involvement, but the organism is sequestered in other areas in both men and women, including the paraurethral ducts, the urethra, and Skene glands. Circumcision reduces infection rate with trichomonads in men (14).
TRICHOMONAS VAGINITIS: Diagnosis
Discharge, irritation, itching, burning
Red mucous membranes and modified mucous membranes; sometimes a classic “strawberry cervix”
White or yellow copious vaginal secretions
pH higher than 5
Wet mount showing motile trichomonads; if negative and high index of suspicion, DNA probe/polymerase chain reaction for trichomonads
Management Trichomoniasis must be treated orally because topical therapies do not eliminate organisms sequestered within the urethra and paraurethral ducts. In addition, sexual partners must be treated to prevent immediate reinfection. Oral metronidazole, at a dose of 500 mg twice a day for 1 week or a single 2-g dose, is usually effective, as is tinidazole as a one-time dose of 2 g. Women should be warned about the disulfiram-like effect of metronidazole with alcohol consumption in some patients, but tinidazole is better tolerated. In addition, some level of resistance to metronidazole was encountered in 1.16% of women in a genitourinary clinic in the United Kingdom (15); either tinidazole or a prolonged course of metronidazole generally effects cure in these patients (15,16).
An occasional patient is allergic to metronidazole, or does not clear with one of these medications. Acetarsol pessaries, furazolidone, fenticonazole, and naturopathic treatments with plant extracts have been used (15,17,18 and 19). Other topical azoles can provide some measure of comfort as well. Most patients improve rapidly without recurrence.
Only gold members can continue reading. Log In or Register to continue