Most chronic external or lower genital symptoms fall into one of two main categories: those who describe itching and scratching and those who report symptoms of pain, burning, rawness, irritation, aching, soreness, or hypersensitivity. Most chronic itching with scratching results from dermatoses. Chronic superficial burning, soreness, and pain, as distinct from pelvic pain, can result from a number of conditions. Pain syndromes rather than specific, observable abnormalities represent the largest proportion of these patients, and most women with self-reported chronic pain were found to have vulvodynia on further evaluation (1). Idiopathic vulvovaginal pain is extremely common, with as many as 1 in 20 women each year developing unexplained, chronic vulvovaginal pain (2). However, there is very little data on pain syndromes in men, although these certainly are recognized by clinicians. The diagnosis and therapy of superficial male genital pain is extrapolated from data and experience with vulvovaginal pain and anecdotal reports regarding experience of a very few individual clinicians.
The International Society for the Study of Vulvovaginal Disease has classified vulvar pain into several main categories (see Table 5-1 and Appendix 1). In the absence of a similar classification for male genital pain, these categories can be used for both genders. This classification serves as a differential diagnosis for patients with superficial genital pain.
The categories of disorders producing genital pain are skin disease, infection, and specific neurological disorders such as diabetic neuropathy, pudendal neuralgia, or postherpetic neuralgia. Those patients who have no observable skin disease, no infection, and no specific neurologic abnormality fall into the category of genital pain syndrome: vulvodynia, penodynia, scrotodynia, and anodynia.
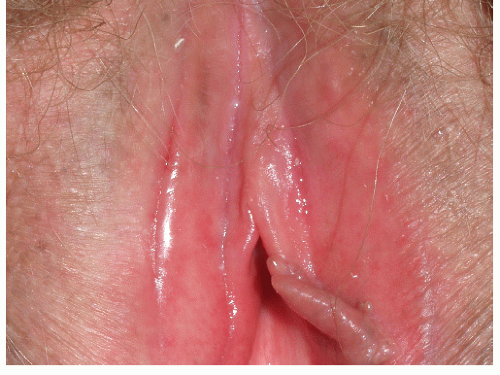
The patient who presents with burning, irritation, and pain-type symptoms should be evaluated in an organized fashion (see Table 5-2). The skin should be examined carefully, using simple magnification if needed. Most patients who report symptoms of burning, irritation, or rawness also report redness, and, often, edema. Redness that is mild, poorly demarcated, and without scaling or thickening is frequently within the range of normal, as genital skin is frequently red in asymptomatic individuals (Fig. 5-1).
At times, patients present with objective skin disease or infection, but discomfort is disproportionate to the degree of skin disease noted, the skin disease may be in a different location than the pain, or pain may persist after the infection or skin disease is cleared. These patients have an underlying pain syndrome either unassociated with the skin disease or triggered by it. The skin disease or infection must be controlled but without clearing of the symptoms before a pain syndrome is definitively diagnosed.
CAUSES OF GENITAL PAIN
Many clinicians and most patients initially assume that genital pain without obvious clinical findings is due to infection, either yeast or sexually transmitted disease. Chronic, unremitting pain is not due to infection, and negative cultures and a lack of response to antimicrobial therapy also signifies a different diagnosis. Most yeast infections are primarily pruritic rather than painful, with the character and degree of vulvovaginal discomfort different as measured on the McGill scale (Fig. 5-2) (3). Sexually transmitted diseases generally either do not cause superficial genital pain (gonorrhea, syphilis, Chlamydia, warts) or they produce intermittent symptoms with visible skin findings (herpes simplex virus infection.) However, trichomonas, particularly in women, certainly produces irritation and burning, although often accompanied by itching.
TABLE 5.1 Causes of chronic genital pain
Infection, especially herpes simplex infection, rubbed/scratched yeast infection, trichomonas, fissures associated with infection
Dermatoses (noninfectious skin disease), especially lichen planus, excoriated/eroded lichen simplex chronicus or lichen sclerosus, irritant contact dermatitis, cicatricial pemphigoid, pemphigus vulgaris, desquamative inflammatory vaginitis, atrophic vaginitis, fissures unassociated with infection, and malignancies/eroded tumors
TABLE 5.2 Evaluation of the patient with genital pain
History
Neurologic history; diabetes, herpes zoster in the genital distribution
Agents applied to the genital skin include soaps, medications, pads/liners
Washing techniques, frequency, etc.
Estrogen status
Physical Examination
Evaluation of affect
Inspection of mucous membranes for evidence of subtle erosive mucosal disease, especially lichen planus
Gross neurologic examination for allodynia, numbness, paresthesias of the anogenital skin and proximal medial thighs.
Examination of the external genitalia with magnification if required for subtle fissures, erosions, signs of scarring/agglutination, or other specific lesions
Assessment of vaginal mucosa for redness, erosions, etc.
Microscopic examination of vaginal secretions for signs of infection, inflammation, and atrophic changes (in addition to yeast forms, evaluation for white blood cells, parabasal cells, lack of lactobacilli)
Culture if examination is suspicious for infection
Biopsy of any specific skin lesion; no biopsy of redness alone or of painful area in normal- appearing skin
The most common skin disease that causes symptoms of burning is irritant contact dermatitis, especially due to overwashing and medications (Figs. 5-3 and 5-4). Allergic contact dermatitis more often produces itching than burning and irritation. Erosive dermatoses most often produce pain and burning as well as itching. Lichen planus is often erosive (Fig. 5-5), as are other blistering diseases such as pemphigus vulgaris or cicatricial pemphigoid (see Chapter 9). However, dermatoses that are primarily pruritic also can be painful when patients have rubbed and scratched the skin; this is usually clear from the history of itching and the findings of excoriations (Fig. 5-6). In women, skin disease causing vulvar burning includes skin disease of the vagina. Even in the face of negative cultures, vaginal inflammation (not infection) can produce introital symptoms. The vaginal skin conditions that most often produce pain symptoms are erosive lichen planus and desquamative inflammatory vaginitis (Fig. 5-7), both of which are characterized by purulent vaginal secretions which irritate the modified mucous membranes of the vulva (Fig. 5-8). Because the vaginal mucosa can be difficult to visualize, especially in the patient with pain, a wet mount can be crucial to rule out inflammatory vaginal disease (Fig. 5-9).
FIG. 5-1. The vulva is normally red, particularly the vestibule and the modified mucous membranes; this patient has no symptoms.
The patient with pain and visible erosions does not present a diagnostic dilemma. However, erosions can be subtle at times; vaginal and introital erosions can be missed in women, and fissures are overlooked easily in both men and women. Specific skin lesions other than poorly demarcated, nonscaling redness that are not morphologically diagnosable should be biopsied.
FIG. 5-2. Although Candidiasis is more pruritic than painful, yeast is the most common cause of fissures, which burn and are often described as “paper cuts.” See Chapter 9.
FIG. 5-3. Fissures can be extremely subtle, but they are often very uncomfortable, producing stinging and burning. This patient had irritant contact dermatitis from overwashing as a cause of his fissure and burning.
Specific neurologic disease can sometimes be identified by history. For example, a diabetic with burning of the feet and genitalia most likely has diabetic neuropathy, and the patient with past herpes zoster of the genital area has postherpetic neuralgia. Postherpetic neuralgia only follows herpes zoster, not herpes simplex virus infection. Multiple sclerosis is sometimes associated with pain syndromes.
Pudendal nerve entrapment syndrome is an occasional cause of anogenital pain (4,5). This can be difficult to diagnose, at least partly because there are several types, and there is considerable individual variation in the anatomy and course of this nerve. There is no one standard evaluation and diagnostic regimen. This condition is suggested by sensory abnormalities in the saddle distribution of the pudendal nerve. There is pain or numbness of the genitalia and adjacent buttock, the proximal, medial thigh, and/or rectal area. Classically, the pain is worst when sitting and minimized by standing or lying. The diagnosis can be implicated further by a careful physical examination, magnetic resonance imaging examination performed by specialists in this disease, and magnetic resonance neurography. Management consists of injections of botulinum toxin, anesthetics, and corticosteroids. Some find benefit from medications for neuropathy and pelvic floor therapy. Those patients who do not improve with these therapies require surgical release of the entrapped nerve.
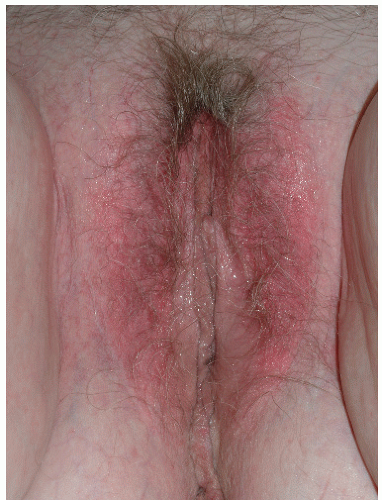
FIG. 5-4. Irritant contact dermatitis is a common cause of poorly demarcated redness and burning; this was contact dermatitis to a panty liner.
FIG. 5-5. Subtle lichen planus can mimic vestibulodynia (vestibulitis); the well-demarcated nature of the vestibular erythema in this patient is the clue that the redness is abnormal. A biopsy of the edge of this red plaque showed lichen planus.
FIG. 5-6. Although excruciating itching was a presenting complaint of this patient, burning and rawness as a result of excoriations followed bouts of scratching. The lichenified skin and excoriations are typical for lichen simplex chronicus.
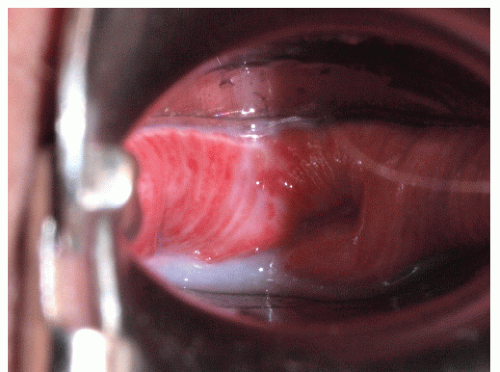
FIG. 5-7. This vagina of desquamative inflammatory vaginitis is diffusely red or speckled with monomorphous red, tiny macules/papules, whereas vaginal lichen planus usually shows patchy redness.
Patients with normal genital skin, to include the vagina, negative cultures, and no specific diagnosable neuropathy, are diagnosed as vulvodynia, penodynia, scrotodynia, or penodynia.
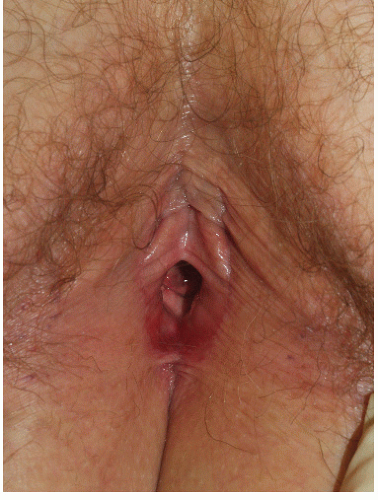
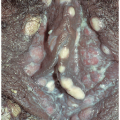
FIG. 5-8. Redness of the introitus and puffiness of the labia minora result from an irritant contact dermatitis to the purulent vaginal secretions of vaginal skin disease.
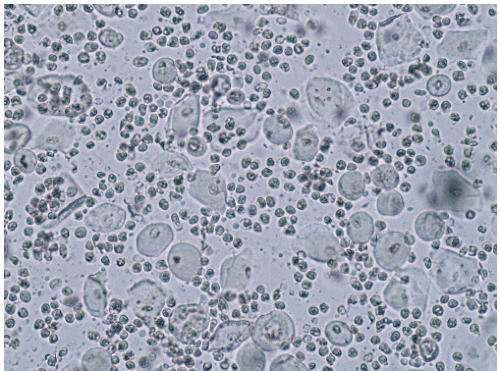
FIG. 5-9. Inflammatory vaginal disease of any cause is characterized by grossly and microscopically purulent vaginal secretions; increased numbers of white blood cells, either neurotrophils or lymphocytes occur, usually in a setting of parabasal cells and absent lactobacilli. These nonspecific findings are common to desquamative inflammatory vaginitis, atrophic vaginitis, and any erosive vaginal disease, including lichen planus, cicatricial pemphigoid, and pemphigoid vulgaris.
Vulvodynia
Vulvodynia is defined as vulvar discomfort characterized by chronic burning, stinging, rawness, irritation, aching, soreness, or throbbing in the absence of objective findings of skin disease, infection, or specific neurologic disease. Itching is not a prominent symptom.
Clinical Presentation
Vulvodynia is an extraordinarily common condition. Several studies report a life-time incidence of 10% to 17% and a current prevalence of 3.8% to 7% (1,6,7). Although initially believed to occur most often in Caucasians, these studies have indicated that patients of African genetic background experience vulvodynia at the same rate as white patients (6), and Hispanics may have an increased risk of developing this disease. The risk of Asian individuals is not known. Vulvodynia is most often reported after the age of 20, but this may simply correlate with the increasing numbers of sexually active people about that age. However, the onset of vulvodynia occurs fairly frequently after menopause as well, independent of atrophic changes. Vulvodynia is found uncommonly in prepubertal girls (8).
Women often report that symptoms began with a yeast infection, although idiopathic vulvar symptoms are frequently empirically treated as yeast. The most common and most troublesome symptom is superficial dyspareunia, often described as sensations of burning, rawness, tearing, or aching. As noted above, other factors that commonly produce discomfort include tight clothing, wiping after urination, tampon use, and gynecologic examinations. Most women indicate the vestibule as the area of greatest discomfort, although extension beyond the vestibule, either by touch/pressure in the office or by history, is usual. At times, pain symptoms extend to the perianal area.
FIG. 5-10. Patchy redness of the vestibule just distal to the hymeneal ring is common in women with vestibulodynia.
A physical examination reveals no skin changes except for variable erythema, especially in the vestibule, and pain to touch with a cotton-tipped applicator that typically is either limited to, or worst, in the vestibule (Fig. 5-10). A vaginal wet mount and fungal preparation are normal. On evaluation of the pelvic floor, tightness to insertion of a finger, tenderness to palpation of the pelvic floor muscles, and overall weakness of these muscles are common.
Vulvodynia occurs most often in women with other chronic pain syndromes, including headaches, fibromyalgia, irritable bowel syndrome, interstitial cystitis, and temporomandibular joint syndrome. Other pelvic floor symptoms are common as well, to include incontinence, frequency, urgency, and constipation. Depression and anxiety are generally prominent, and sexual dysfunction is universal.
Diagnosis
The diagnosis of vulvodynia is made by the presence of pain in the absence of objective, definable causes of vulvovaginal pain, other than, at times, minor redness, pain to touch, or abnormal pelvic floor examinations. Skin disease is excluded by a careful examination, and, when indicated by the presence of specific lesions, a biopsy. Vaginal secretions must be normal, without signs of inflammation, atrophy, or infection on wet mount (see Chapter 15). A routine culture to exclude infection as a major or minor factor should be performed for most patients. A history to explore the possibility of neurologic disease as a factor must be done, with referral to a specialist gynecologist in the occasional instance of pudendal neuralgia or a neurologist in the unlikely event of serious considerations of other specific neurologic disease such as multiple sclerosis.
Most women with vulvodynia experience pain to pressure with a cotton tipped applicator; this pain is nearly always present in the vestibule, but sometimes extends beyond this area. In addition to pain with touch and pressure, most patients with vulvodynia also report discomfort in the absence of touch or friction, at least occasionally with flares. The occasional patient describes only background burning and irritation but no pain with touch or pressure.
Appendix 1 reports the classification of recognized patterns of vulvodynia. There are two major patterns of vulvodynia; those patients with pain to pressure in the vestibule and no extension beyond this area are said to have vestibulodynia (previously called the vulvar vestibulitis syndrome, vestibular adenitis, or infection of the minor vestibular glands). Those patients who have more generalized or migratory discomfort are diagnosed with generalized vulvodynia. However, vulvodynia can be localized to other areas, such as the clitoris, and pain can be either spontaneous or occurring in response to touch, pressure, or friction. This author believes that a careful history and examination shows overlap among the patterns of vulvodynia in most patients, and several studies support this contention (9,10). The importance of differentiation among the patterns lies in a search for differing etiologies, the allowance for studies with uniformity in patient population, and the success of excisional surgery only in patients with vestibulodynia pattern. Otherwise, treatments are the same for all groups.
Only gold members can continue reading. Log In or Register to continue