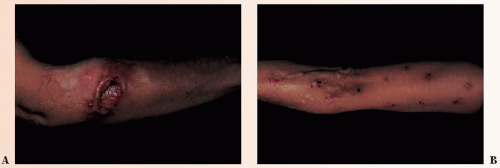
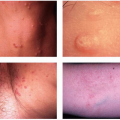
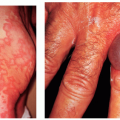
 FIGURE 38-1 ▪ Nonspecific skin changes indicating an underlying psychologic disease state. (A) Delusional excoriation on the arm (“have to get the hairs out”). (B) Neurotic excoriations on the arm. |
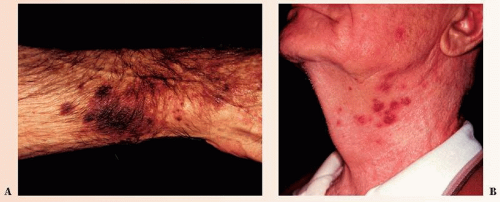 FIGURE 38-2 ▪ Nonspecific skin changes resulting from an internal disease. Purpura of the arm (A) and folliculitis of the neck (B) in a patient with myelogenous leukemia. (Courtesy of Syntext Laboratories, Inc.) |
TABLE 38-1 ▪ Internal Malignancies with Cutaneous Manifestations | |||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||
Lentigines: multiple lentigines are present at birth and may cover the entire body, including the palms and soles but sparing the lips and oral mucosa. The pigment can be seen in the iris and retina as well
Electrocardiogram conduction defects
Ocular hypertelorism
Pulmonary stenosis
Abnormalities of genitalia
Retardation of growth
Deafness (sensorineural)
vascular compromise, may eventuate in neuropathic foot ulcers (Fig. 38-4).
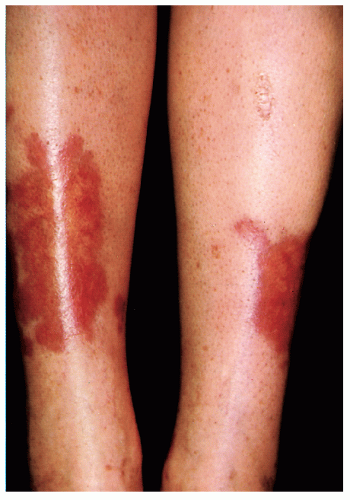 FIGURE 38-3 ▪ Necrobiosis lipoidica diabeticorum on the anterior tibial area of the legs. (Courtesy of Smith Kline & French Laboratories.) |
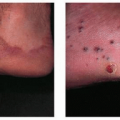
 FIGURE 38-4 ▪ Mal perforans ulcer on the great toe of a diabetic man. |
 FIGURE 38-5 ▪ Necrobiosis lipoidica. |
Addisonian hyperpigmentation
Precocious puberty
Virilization
Pattern alopecia in females
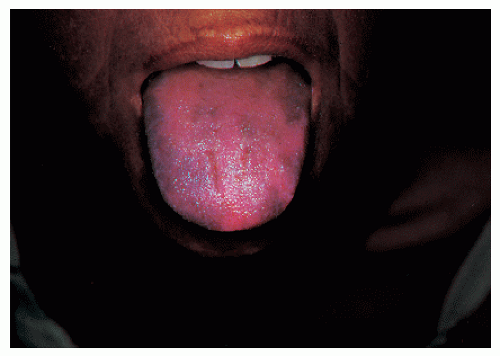 FIGURE 38-6 ▪ Hyperpigmentation of skin and tongue in a white woman with Addison’s disease. |
attendant nonscarring alopecia and soft nails with distal onycholysis. Graves’ disease is associated with ophthalmopathy (proptosis, exophthalmos, and lid lag), thyroid dermopathy (pretibial myxedema), and acropachy.
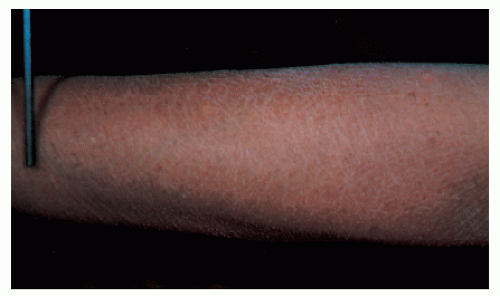 FIGURE 38-7 ▪ Year-round dry skin associated with hypothyroidism. (Courtesy of Reed and Carnick.) |
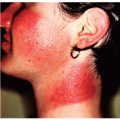
 FIGURE 38-8 ▪ Pyoderma gangrenosum associated with ulcerative colitis. (Part D courtesy of Schering Corp.) |
nodule or pustule breaks down to form an enlarging ulcer with a raised, undetermined border and a boggy, necrotic base. Pyoderma gangrenosum has also been observed with Crohn’s disease as well as hematologic malignancies, monoclonal gammopathies, and various arthritides.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


