Pruritic Dermatoses
John C. Hall MD
Pruritus, or itching, brings more patients to the physician’s office than any other skin disease symptom. Itchy skin is not easily cured or even alleviated. Decreased quality of life due to pruritus can be as significant as with pain. Many hundreds of proprietary over-the-counter and prescription drugs are touted as effective anti-itch remedies, but none is 100% effective. Many are partially effective, but it is unfortunate that the most effective locally applied chemicals frequently irritate or sensitize the skin.
Pruritus is a symptom of many of the common skin diseases, such as contact dermatitis, atopic eczema, seborrheic dermatitis, hives, scabies, insect bites, some drug eruptions, and many other dermatoses. Relief of itching is of prime importance in treating these diseases.
In addition to the pruritus that occurs as a symptom of many skin diseases, there are other clinical forms of pruritus that deserve special consideration. These special types include generalized pruritus of the winter, senile, and essential varieties and localized pruritus of the lichen simplex type, which affects the ears, anal area, lower legs in men, back of the neck in women, and genitalia. Localized pruritus of unknown etiology should alert one to the possibility of underlying peripheral nerve or central nervous system pathology.
Generalized Pruritus
Diffuse itching of the body without perceptible skin disease usually is due to winter dry skin or senile skin.
Winter Pruritus
Winter pruritus, or pruritus hiemalis, is a common form of generalized pruritus, although most patients complain of itching confined mainly to their legs. Every autumn, a certain number of elderly patients, and occasionally young ones, walk into the physician’s office complaining bitterly of the rather sudden onset of itching of their legs. Men often also itch around the waist. These patients have dry skin caused by the low humidity in their furnace-heated homes, or occasionally from the low humidity resulting from cooling air conditioning. Clinically, the skin shows excoriations and dry, curled, scaling plaques resembling a sun-baked, muddy beach at low tide. The dry skin associated with winter itch is to be differentiated from ichthyosis, a congenital, inherited dermatosis of varying severity, which is also worse in the winter.
SAUER’S NOTE
When the presenting complaint is generalized itching of the skin, always stroke the skin on the forearm with your nail or a tongue depressor. After 5 minutes or so, if there is a wheal reaction at the stroking site, you have a diagnosis of dermographism. This is a common problem that is easily overlooked.
Treatment of winter pruritus consists of the following:
1. Bathing should involve as cool water as possible and as little soap as possible. Soap can be limited to the face, axillae, groin, genitalia, hands, and feet.
2. A bland soap, such as Dove, Oilatum, Cetaphil, or Basis, is used sparingly.
3. An oil is added to the bath water, such as Lubath, RoBathol, Nivea, or Alpha Keri. (The patient should be warned to avoid slipping in the tub.) The oil can be rubbed on after a shower.
4. Emollient lotions are beneficial, such as Complex 15 (phospholipid), CeraVe (ceramides), Curel (petrolatum), Eucerin, Aquaphor (esterified lanolin, quite greasy), Pen Kera, or Moisturel (not as greasy and noncomedogenic). α-Hydroxy acid preparations include AmLactin 12% cream and lotion (over the counter), Lac-Hydrin 5% (over the counter), Lac-Hydrin 12% (prescription only), and Eucerin Plus. Urea products (in these higher concentrations may be irritating except on palms or soles) that are beneficial include Kera Lotion (35%),Keracream (40%),Vanamide (40%), Carmol 40 cream and lotion (40%), and Eucerin Plus lotion (also has lactic acid as an α-hydroxy acid). Lubricants should be applied immediately after bathing for the most benefit.
5. A low-potency corticosteroid ointment applied twice daily is effective. Triamcinolone ointment 0.1% is midpotency and very inexpensive. A 1% hydrocortisone can be mixed with any of the mentioned moisturizers or used as a nonspecific ointment.
6. Oral antihistamines are sometimes effective, such as chlorpheniramine (Chlor-Trimeton), 4 mg h.s. or q.i.d, or diphenhydramine (Benadryl), 50 mg h.s. There are newer nonsedating antihistamines such as Claritin 10 mg q.d.
(over the counter), Clarinex 10 mg q.d., Zyrtec (may be slightly sedating and also more effective) 10 mg q.d., and Allegra 60 or 180 mg q.d. Some dermatologists do not think the nonsedating antihistamines are as effective as the sedating antihistamines. A commonly used sedating antihistamine is hydroxyzine, 10 mg every 8 hours while awake. The dose can be titrated to 25 mg, 50 mg, or rarely 100 mg. The soporific effect, or drowsiness, often becomes less severe with prolonged use.
(over the counter), Clarinex 10 mg q.d., Zyrtec (may be slightly sedating and also more effective) 10 mg q.d., and Allegra 60 or 180 mg q.d. Some dermatologists do not think the nonsedating antihistamines are as effective as the sedating antihistamines. A commonly used sedating antihistamine is hydroxyzine, 10 mg every 8 hours while awake. The dose can be titrated to 25 mg, 50 mg, or rarely 100 mg. The soporific effect, or drowsiness, often becomes less severe with prolonged use.
7. Doxepin (Sinequan) starting at 10 mg/d and working up to 50 mg/d has been used with some success but can be sedating.
8. Neurontin (gabapentin) 300 mg/d and over weeks to months working up to doses as high as 1,800 mg/d in divided doses has been shown to be successful by some authors.
9. Ultraviolet light in the form of psoralens and ultraviolet light (PUVA) (increases risk of skin malignancy) and narrow band UVB may be beneficial.
Senile Pruritus
Senile pruritus is a resistant form of generalized pruritus in the elderly patient. It can occur at any time of the year and may or may not be associated with dry skin. There is some evidence that these patients have a disorder of keratinization. This form of itch occurs most commonly on the scalp, shoulders, sacral areas, and legs. Clinically, some patients have no cutaneous signs of the itch, but others may have linear excoriations. Scabies should be ruled out, as well as the diseases mentioned under the next form of pruritus to be considered, essential pruritus.
Treatment is usually not very satisfactory. In addition to the agents mentioned previously in connection with winter pruritus, the injection of 40 mg of triamcinolone acetonide suspension (Kenalog-40) intramuscularly every 4 to 6 weeks for two or three injections is quite beneficial. I do not like to repeat this more often than three to four times a year to avoid systemic corticosteroid side effects. Topical antipruritic agents can be used, such as pramoxine hydrochloride (Pramosone with either 1% or 2.5% hydrocortisone is a prescription or Aveeno Anti-itch lotion, which is available over the counter). Menthol (0.5%), phenol (0.5%), or sulfur (2% to 5%) can be added to any appropriate base (see Chapter 4).
Essential Pruritus
Essential pruritus is the rarest form of the generalized itching diseases. No person of any age is exempt, but it occurs most frequently in the elderly patient. The itching is usually quite diffuse, with occasional “bites” in certain localized areas. All itching is worse at night, and no exception is made for this form of pruritus. Before a diagnosis of essential pruritus is made, the following diseases must be ruled out by appropriate studies:
Drug reaction
Diabetes mellitus
Uremia
Lymphoma (mycosis fungoides, leukemia, or lymphoma [especially Hodgkin’s disease]), as a paraneoplastic syndrome from any metastatic underlying malignancy
Primary sclerosing cholangitis, which has very severe pruritus
Liver disease (especially hepatitis B or C even without jaundice)
Bullous pemphigoid before the blisters are present
AIDS and other immunosuppressed states
Stress or more severe psychiatric illness such as psychosis or parasitophobia
Hyperthyroidism
Post-brain tissue damage such as a stroke, brain cancer, or trauma
Intestinal parasites
Intrahepatic cholestasis of pregnancy—early diagnosis in the second half of pregnancy with elevation of total serum bile acids should prompt early treatment with ursodeoxycholic acid
Telangiectasia macularis eruptiva perstans (may need skin biopsy to find)
Cutaneous T-cell lymphoma “incognito” (may need skin biopsy to find)
Drugs, especially opiates such as morphine
Treatment is the same as for senile and winter pruritus. Narrow band UVB is a safe and sometimes effective nonspecific treatment for pruritus. For more recalcitrant severe cases, here is a list of other therapies that can be tried: psychotherapy (including hypnosis), acupuncture, in dialysis patients more intense dialysis and magnesium-free dialysis, systemic metronidazole (primary sclerosing cholangitis), ursodeoxycholic acid (primary biliary cirrhosis), sertraline (75 to 100 mg daily), naltrexone (12.5 mg to start and up to 50 mg daily), rifampicin (150 mg t.i.d.), ondansetron (8 mg t.i.d.), gabapentin, nalfurafine, ketotifen, cholestyramine (liver and gallbladder disease), oral activated charcoal, thalidomide, intravenous lidocaine, bupropion, doxepin (10 to 30 mg h.s.), and pimozide.
Localized Pruritic Dermatoses
Lichen Simplex Chronicus
Other common terms for lichen simplex chronicus (LSC) include localized neurodermatitis and lichenified dermatitis. There are pros and cons for all the terms.
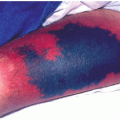
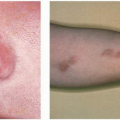
LSC (Fig. 11-1) is a common skin condition characterized by the occurrence of single or, less frequently, multiple patches of chronic itching and thickened, scaly, dry skin in one or more of several classic locations. It is unrelated to atopic eczema according to some experts, but others feel it is an adult form of eczema.
Primary Lesions
This disease begins as a small, localized, well-demarcated, pruritic papule or patch of dermatitis that might have been
an insect bite, chigger bite, contact dermatitis, or other minor irritation that may or may not be remembered by the patient. Because of various etiologic factors, a cycle of itching, scratching, more itching, and more scratching supervenes, and achronic dermatosis develops. Emotional stress is thought to lower the itch threshold and cause exacerbation of the disease. The itching is intense and paroxysmal in nature.
an insect bite, chigger bite, contact dermatitis, or other minor irritation that may or may not be remembered by the patient. Because of various etiologic factors, a cycle of itching, scratching, more itching, and more scratching supervenes, and achronic dermatosis develops. Emotional stress is thought to lower the itch threshold and cause exacerbation of the disease. The itching is intense and paroxysmal in nature.
 FIGURE 11-1 ▪ Localized LSC of the leg. This is a common location. Note the lichenification and excoriations owing to the marked pruritus. (Courtesy of K.U.M.C.; Duke Labs, Inc.) |
Secondary Lesions
These include excoriations, lichenification, and, in severe cases, marked verrucous thickening of the skin, with pigmentary changes. In severe cases, healing is bound to be followed by some scarring.
Presentation and Characteristics
Distribution.




Related posts:


Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
