Diseases of the Mucous Membranes
John C. Hall MD
The mucous membranes of the body adjoin the skin at the oral cavity, nose, conjunctiva, penis, vulva, and anus. Histologically, these membranes differ from the skin in that the horny layer and the hair follicles are absent. Disorders of the mucous membranes are usually associated with existing skin diseases or internal diseases. Only the most common diseases of the mucous membranes are discussed herein. At the end of the chapter is a listing of the uncommon conditions of these areas.
Geographic Tongue
Geographic tongue is an extremely common condition of the tongue that usually occurs without symptoms. When these lesions are noticed for the first time by the individual, they may initiate fears of cancer.
Presentation and Characteristics
Clinical Appearance
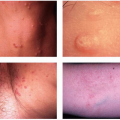
Irregularly shaped (maplike or geographic) pale red patches are seen on the tongue (Fig. 34-1). Close examination reveals that the filiform papillae are flatter or denuded in these areas. The patches slowly migrate over the tongue surface and heal without scarring.
 FIGURE 34-1 ▪ Geographic tongue. (Courtesy of Neutrogena Corp.) |
Course
The disorder may come and go but may be constantly present in some persons.
Cause
The cause is unknown, but the lesions seem to be more extensive during a systemic illness. It has been suggested by some authors that geographic tongue is a form of psoriasis.
Subjective Symptoms
Some patients complain of burning and tenderness, especially when eating sour or salty foods.
Differential Diagnosis
Syphilis, secondary mucous membrane lesions: similar clinically, but acute in onset; usually more inflammatory; other cutaneous signs of syphilis; dark field examination and serology positive (see Chapters 22 and 26); does not come and go as rapidly.
Treatment
1. Reassure patient that these are not cancerous lesions.
2. There is no effective or necessary therapy. However, if patient complains of burning and tenderness, prescribe triamcinolone (Kenalog) in Orabase 15.0 Sig: Apply locally q.i.d. half hour p.c. and h.s.
Gingival Enlargement
Excessive growth of periodontal tissue with raising and blunting of the gingival margins.
Presentation and Characteristics
Clinical Appearance
If inflammation is present, the gingiva appears shiny, red, smooth, soft, and friable, with easy bleeding. If noninflammatory, it is firm with loss of stippling and contains a reddish-purple hue.
Course
Improvement is common if the underlying cause is treated.
Cause
Systemic diseases include primary amyloidosis, sarcoidosis, acromegaly, Kaposi’s sarcoma, Wegener’s granulomatosis, leukemia, aplastic anemia, lymphomas, Crohn’s disease, scurvy, and neurofibromatosis.
Drug causes include phenytoin, calcium channel blockers, and cyclosporine. Less common drugs include lithium, tacrolimus, sertraline, birth control pills, ketaconazole, erythromycin, and other antisiezure medicines in addition to phenytoin. Poor dental hygiene with chronic gingivitis may be causative. It can be congenital, idiopathic, or physiologic in pregnancy or puberty.
Symptoms
Pain, tenderness, halitosis, poor speech, difficult mastication and unsightly appearance are all reasons to initiate therapy.
Treatment
Therapy is focused on the treatment of the underlying cause as well as aggressive oral hygiene. Surgical reduction is the last approach to be considered.
Aphthous Stomatitis
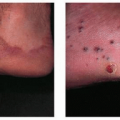
Canker sores are extremely common, painful, superficial ulcerations of the mucous membranes of the mouth (Fig. 34-2).
Presentation and Characteristics
Course
One or more lesions develop at the same time and heal without scarring in 5 to 10 days. They can recur at irregular intervals. It is the most common oral inflammatory disease (affects 20% of population). It usually begins in adolescence and peaks in incidence in the third to fourth decade, after which the disease becomes less severe and less frequent.
 FIGURE 34-2 ▪ (A) Recurrent aphthous ulcer of the tongue. (B) Aphthous ulcer in patient with cyclic neutropenia. (Courtesy of Neutrogena Corp.) |
Clinical Appearance
Lesions are usually located on nonkeratinized mucosa (buccal, labial sulci, lateral and ventral tongue, soft palate, oropharynx).
There are three subtypes: (1) minor lesions (80%) are less than 5 mm to 1 cm, especially buccal and labial, and heal spontaneously in 7 to 10 days without a scar, (2) major (10%) are 5 to 10 mm deep, heal in weeks to months and often scar; other names are Sutton’s ulcers or periadenitis mucosa necrotica recurrens, and (3) herpetiform (10%) occur on dorsal tongue, palate, or other keratinized mucosa, are small (1 to 3 mm) and grouped on coalescent ulcers, and heal in 1 to 4 weeks.
Cause
The cause is unknown, but certain foods, especially chocolate, nuts, and fruits, can precipitate the lesions or may even be causative. Trauma from biting or dental procedures can initiate lesions (pathergy). Some cases in women recur in relation to menstruation. A viral cause has not been proved. A pleomorphic, transitional L-form of an α-hemolytic Streptococcus sp (Streptococcus sanguis) has also been implicated as causative. Stress, nutritional deficiency, smoking cessation, and allergy may be triggers. Numerous underlying illnesses include Behçet’s disease, human immunodeficiency virus (HIV), inflammatory bowel disease, cyclic neutropenia, FAPA (fever, aphthous stomatitis, pharyngitis, adenitis), and MAGIC (mouth and genital ulcers with inflamed cartilage and gluten-sensitive enteropathy). The disease can also be a sign of deficiencies of iron, zinc, folate, and B vitamins 1, 2, 6, and 12.
Differential Diagnosis
Syphilis,Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree