Pruritus
Pruritus, commonly known as itching, is a sensation exclusive to the skin. It may be defined as the sensation that produces the desire to scratch. Pruritogenic stimuli are first responded to by keratinocytes, which release a variety of mediators, and fine intraepidermal C-neuron filaments. Approximately 5% of the afferent unmyelinated C neurons respond to pruritogenic stimuli. Itch sensations in these nerve fibers are transmitted via the lateral spinothalamic tract to the brain, where a variety of foci generate both stimulatory and inhibitory responses. The sum of this complicated set of interactions appears to determine the quality and intensity of itch.
Itching may be elicited by many normally occurring stimuli, such as light touch, temperature change, and emotional stress. Chemical, mechanical, and electrical stimuli may also elicit itching. The brain may reinterpret such sensations as being painful or causative of burning or stinging sensations. A large group of neuromediators and their receptors have been identified. Some of the most important mediators are histamine and the H4 receptor, tryptase and its proteinase-activated receptor type 2, opioid peptides and the mu (µ) and kappa (κ) opioid receptors, leukotriene B4, prostaglandins such as PGE, thymic stromal lymphopoietin, acetylcholine, cytokines such as interleukin-31 (IL-31), and a variety of neuropeptides and vasoactive peptides (e.g., nerve growth factor, substance P) and their receptors (e.g., TRPV1). Investigation is ongoing to discover the relative importance of each of these mediators and to determine the clinical circumstances under which therapeutic targeting of these molecules will lead to relief of symptoms.
Itch has been classified into four primary categories, as follows:
- •
Pruritoceptive itch, initiated by skin disorders
- •
Neurogenic itch, generated in the central nervous system and caused by systemic disorders
- •
Neuropathic itch, caused by anatomic lesions of the central or peripheral nervous system
- •
Psychogenic itch, the type observed in parasitophobia
Patterns of Itching
There are wide variations in itching from person to person, and a person may have a variation in reactions to the same stimulus. Heat will usually aggravate preexisting pruritus. Stress, absence of distractions, anxiety, and fear may all enhance itching. Itching tends to be most severe during undressing for bed.
Severe pruritus, with or without prior skin lesions, may be paroxysmal in character with a sudden onset, often severe enough to awaken the patient. It may stop instantly and completely as soon as pain is induced by scratching. However, the pleasure of scratching is so intense that the patient, despite the realization of damaging the skin, is often unable to stop short of inflicting such damage ( Fig. 4.1 ). Itching of this distinctive type is characteristic of a select group of dermatoses: lichen simplex chronicus, atopic dermatitis, nummular eczema, dermatitis herpetiformis, neurotic excoriations, eosinophilic folliculitis, uremic pruritus, prurigo simplex, paraneoplastic itch (usually secondary to lymphoma), and prurigo nodularis. In general, only these disorders produce such intense pruritus and scratching as to induce bleeding. In individual cases, other diseases may manifest such severe symptoms.

Treatment
General guidelines for therapy of the itchy patient include keeping cool and avoiding hot baths or showers and wool clothing, which is a nonspecific irritant, as is xerosis. Many patients note itching increases after showers, when they wash with soap and then dry roughly. Using soap only in the axilla and inguinal area, patting dry, and applying a moisturizer can often help prevent such exacerbations. If itching is severe, a trial of “soaking and smearing” may provide significant relief (see winter itch later in this chapter). Patients often use an ice bag or hot water to ease pruritus; however, hot water can irritate the skin, is effective only for short periods, and over time exacerbates the condition.
Relief of pruritus with topical remedies may be achieved with topical anesthetic preparations. Many contain benzocaine, which may produce contact sensitization. Pramoxine in a variety of vehicles, lidocaine 5% ointment, eutectic mixture of lidocaine and prilocaine (EMLA) ointment, and lidocaine gel are preferred anesthetics that may be beneficial in localized conditions. EMLA and lidocaine may be toxic if applied to large areas. Topical antihistamines are generally not recommended, although doxepin cream may be effective for mild pruritus when used alone. Doxepin cream may cause contact allergy or a burning sensation, and somnolence may occur when doxepin is used over large areas. Topical lotions that contain menthol or camphor feel cool and improve pruritus. They may be kept in the refrigerator to enhance this soothing effect. Other lotions have specific ceramide content designed to mimic that of the normal epidermal barrier. Capsaicin, by depleting substance P, can be effective, but the burning sensation present during initial use frequently causes patients to discontinue its use. Topical steroids and calcineurin inhibitors effect a decrease in itching through their antiinflammatory action and therefore are of limited efficacy in neurogenic, psychogenic, or systemic disease–related pruritus.
Phototherapy with ultraviolet B (UVB), UVA, and psoralen plus UVA (PUVA) may be useful in a variety of dermatoses and pruritic disorders. Many oral agents are available to treat pruritus. Those most frequently used by nondermatologists are the antihistamines. First-generation H1 antihistamines, such as hydroxyzine and diphenhydramine, may be helpful in nocturnal itching, but their efficacy as antipruritics is disappointing in many disorders, except for urticaria and mastocytosis. Doxepin is an exception in that it can reduce anxiety and depression and is useful in several pruritic disorders. Sedating antihistamines should be prescribed cautiously, especially in elderly patients because of their impaired cognitive ability. The nonsedating antihistamines and H2 blockers are only effective in urticaria and mast cell disease. Opioids are involved in itch induction. In general, activation of µ-opioid receptors stimulates itch, whereas κ-opioid receptor stimulation inhibits itch perception; however, the interaction is complex. Additionally, opioid-altering agents such as naltrexone, naloxone, nalfurafine, and butorphanol have significant side effects and varying modes of delivery (intravenous, intranasal, oral). Initial reports of benefit in one condition are often followed by conflicting reports on further study. Specific recommendations in select pruritic conditions are detailed in those sections. These agents appear most useful for cholestatic pruritus. Central reduction of itch perception may be effected by anticonvulsants, such as gabapentin and pregabalin, and antidepressants, such as mirtazapine and the selective serotonin reuptake inhibitors (SSRIs). These take 8–12 weeks to attain full onset of action. Thalidomide, through a variety of direct neural effects, immunomodulatory actions, and hypnosedative effects, is also useful in select patients.
Chan IH, Murrell DF: Itch management. Curr Probl Dermatol 2016; 50: 54.
Elmariah SB, et al: Topical therapies for pruritus. Semin Cutan Med Surg 2011; 30: 118.
Matsuda KM, et al: Gabapentin and pregabalin for the treatment of chronic pruritus. J Am Acad Dermatol 2016; 75: 619.
Matterne U, et al: Prevalence, correlates and characteristics of chronic pruritus. Acta Derm Venereol 2011; 91: 674.
Misery L, et al: Neuropathic pruritus. Nat Rev Neurol 2014; 10: 408.
Pereira MP, et al: Chronic pruritus in the absence of skin disease. Am J Clin Dermatol 2016; 17: 337.
Sharma D, Kwatra SG: Thalidomide for the treatment of chronic refractory pruritus. J Am Acad Dermatol 2016; 74: 363.
Ständer S, et al: Emerging drugs for the treatment of pruritus. Expert Opin Emerg Drugs 2015; 20: 515.
Stull C, et al: Advances in the therapeutic strategies for the treatment of pruritus. Expert Opin Pharmacother 2016; 17: 671.
Valdes-Rodriguez R, et al: Chronic pruritus in the elderly. Drugs Aging 2015; 32: 201.
Weisshaar I, et al: European guideline on chronic pruritus. Acta Derm Vernereol 2012; 92: 563.
Yosipovitch G, et al: Chronic pruritus. N Engl J Med 2013; 368: 1625.
Internal Causes of Pruritus
Itching may be present as a symptom in a number of internal disorders. The intensity and duration of itching vary from one disease to another. The most important internal causes of itching include liver disease, especially obstructive and hepatitis C (with or without evidence of jaundice or liver failure), renal failure, diabetes mellitus, hypothyroidism and hyperthyroidism, hematopoietic diseases (e.g., iron deficiency anemia, polycythemia vera), neoplastic diseases (e.g., lymphoma [especially Hodgkin disease and cutaneous T-cell lymphoma], leukemia, myeloma), internal solid-tissue malignancies, intestinal parasites, carcinoid, multiple sclerosis, acquired immunodeficiency syndrome (AIDS), connective tissue disease (particularly dermatomyositis) and neuropsychiatric diseases, especially anorexia nervosa.
The pruritus of Hodgkin disease is usually continuous and at times is accompanied by severe burning. The incidence of pruritus is 10%–30% and is the first symptom of this disease in 7% of patients. Its cause is unknown. The pruritus of leukemia, except for chronic lymphocytic leukemia, has a tendency to be less severe than in Hodgkin disease.
Internal organ cancer may be found in patients with generalized pruritus that is unexplained by skin lesions. However, no significant overall increase of malignant neoplasms can be found in patients with idiopathic pruritus. A suggested workup for chronic, generalized pruritus includes a complete history, thorough physical examination, and laboratory tests, including complete blood count (CBC) and differential; thyroid, liver, and renal panels; fasting blood glucose; hepatitis C serology; human immunodeficiency virus (HIV) antibody (if risk factors are present); urinalysis; stool for occult blood; serum protein electrophoresis; and chest x-ray evaluation. Presence of eosinophilia on the CBC is a good screen for parasitic diseases, but if the patient has been receiving systemic corticosteroids, blood eosinophilia may not be a reliable screen for parasitic diseases, and stool samples for ova and parasites should be submitted. Additional radiologic studies or specialized tests are performed as indicated by the patient’s age, history, and physical findings. A biopsy for direct immunofluorescence is occasionally helpful to detect dermatitis herpetiformis or pemphigoid.
Treatment of the itch associated with some of these internal conditions is discussed later in this chapter or under those specific diseases in other chapters; however, in other conditions listed previously treatment of the underlying disease state (e.g., treating the cancer, replacing thyroid hormone in hypothyroidism) causes relief of the pruritus. Be aware that disease specific therapies can exacerbate itching during treatment, for instance in cancer patients treated with biologic agents such as the anti EGFR monocolonal antibiodies.
Cassano N, et al: Chronic pruritus in the absence of specific skin disease. Am J Clin Dermatol 2010; 11: 399.
Rowe B, Yosipovitch G: Malignancy-associated pruritus. Eur J Pain 2016; 20: 19.
Santoni M, et al: Risk of pruritus in cancer patients treated with biological therapies. Crit Rev Oncol Hematol 2015; 96: 206.
Tarikci N, et al: Pruritus in systemic diseases. Scientific World Journal 2015; 2015: 803752.
Weisshaar I, et al: European guideline on chronic pruritus. Acta Derm Vernereol 2012; 92: 563.
Chronic Kidney Disease
Chronic kidney disease (CKD) is the most common systemic cause of pruritus; 20%–80% of patients with chronic renal failure have itching. The pruritus is often generalized, intractable, and severe; however, dialysis-associated pruritus may be episodic, mild, or localized to the dialysis catheter site, face, or legs.
The mechanism of pruritus associated with CKD is multifactorial. Xerosis, secondary hyperparathyroidism, increased serum histamine levels, hypervitaminosis A, iron deficiency anemia, and neuropathy have been implicated. Complications such as acquired perforating disease, lichen simplex chronicus, and prurigo nodularis may develop and contribute to the degree and severity of pruritus ( Fig. 4.2 ).

Many patients have concomitant xerosis, and aggressive use of emollients, including “soaking and smearing” (see winter itch later in this chapter), may help. A trial of γ-linolenic acid cream twice daily was effective, as was one using baby oil. Gabapentin given three times weekly at the end of hemodialysis sessions can be effective, but its renal excretion is decreased in CKD, so a low initial dose of 100 mg after each session with slow upward titration is recommended. A mainstay of CKD-associated pruritus has been narrow-band (NB) UVB phototherapy, but a randomized controlled trial (RCT) failed to confirm its efficacy. Broad-band UVB may be best in the CKD patient. Naltrexone, topical tacrolimus, and ondansetron also were reported to be useful in initial trials, but subsequent studies indicated these agents are ineffective. Nalfurafine, 5 µg once daily after supper, has demonstrated improvement and was relatively well tolerated over a 1-year study. Thalidomide, intranasal butorphanol, and intravenous lidocaine are less practical options. Patients on peritoneal dialysis have a lower severity of pruritus than those on hemodialysis. Renal transplantation will eliminate pruritus.
Berger TG, et al: Pruritus and renal failure. Semin Cutan Med Surg 2011; 30: 99.
Combs SA, et al: Pruritus in kidney disease. Semin Nephrol 2015; 35: 383.
Ko MJ, et al: Narrowband ultraviolet B phototherapy for patients with refractory uraemic pruritus. Br J Dermatol 2011; 165: 633.
Mettang T: Uremic itch management. Curr Probl Dermatol 2016; 50: 133.
Mettang T, Kremer AE: Uremic pruritus. Kidney Int 2015; 87: 685.
Wu HY, et al: A comparison of uremic pruritus in patients receiving peritoneal dialysis and hemodialysis. Medicine (Baltimore) 2016; 95: e2935.
Biliary Pruritus
Chronic liver disease with obstructive jaundice may cause severe generalized pruritus, and 20%–50% of patients with jaundice have pruritus. Intrahepatic cholestasis of pregnancy, primary sclerosing cholangitis, and hereditary cholestatic diseases such as Alagille syndrome all have pruritus in common. Another disease, primary biliary cirrhosis, is discussed separately next because of its many other cutaneous manifestations. Hepatitis C may be associated with pruritus as well.
Itching of biliary disease is probably caused by central mechanisms. The pathophysiology is not well understood, but it appears that lysophosphatidic acid, formed by the action of the enzyme autotaxin on lysophosphatidylcholine, is central. The serum conjugated bile acid levels do not correlate with the severity of pruritus, and the theory invoking endogenous opioids as the main cause has not been upheld.
Pruritus of chronic cholestatic liver disease is improved with cholestyramine, 4 to 16 g daily. Rifampin, 150 to 300 mg/day, may be effective but should be used with caution because it may cause hepatitis. Naltrexone, up to 50 mg/day, is useful but has significant side effects. If used, naltrexone should be started at ![]() tablet (12.5 mg) and increased by
tablet (12.5 mg) and increased by ![]() tablet every 3 to 7 days until pruritus improves. Sertraline, 75 to 100 mg/day, is another option. UVB phototherapy was effective in a small case series. Ursodeoxycholic acid is effective for the pruritus in intrahepatic cholestasis of pregnancy, but not for the itching from other causes. Liver transplantation is the definitive treatment for end-stage disease and provides dramatic relief from the severe pruritus.
tablet every 3 to 7 days until pruritus improves. Sertraline, 75 to 100 mg/day, is another option. UVB phototherapy was effective in a small case series. Ursodeoxycholic acid is effective for the pruritus in intrahepatic cholestasis of pregnancy, but not for the itching from other causes. Liver transplantation is the definitive treatment for end-stage disease and provides dramatic relief from the severe pruritus.
Primary Biliary Cirrhosis.
Primary biliary cirrhosis occurs almost exclusively in women older than 30. Itching may begin insidiously and may be the presenting symptom in a quarter to half of patients. With time, extreme pruritus develops in almost 80% of patients. This almost intolerable itching is accompanied by jaundice and a striking melanotic hyperpigmentation of the entire skin; the patient may turn almost black, except for a hypopigmented “butterfly” area in the upper back. Eruptive xanthomas, planar xanthomas of the palms ( Fig. 4.3 ), xanthelasma, and tuberous xanthomas over the joints may be seen.

Dark urine, steatorrhea, and osteoporosis occur frequently. Serum bilirubin, alkaline phosphatase, serum ceruloplasmin, serum hyaluronate, and cholesterol values are increased. The antimitochondrial antibody test is positive. The disease is usually relentlessly progressive with the development of hepatic failure. Several cases have been accompanied by scleroderma.
Bunchornatavakul C, et al: Pruritus in chronic cholestatic lever disease. Clin Liver Dis 2012; 16: 331.
Carey EJ, et al: Primary biliary cirrhosis. Lancet 2015; 386: 1565.
Decock S, et al: Cholestasis-induced pruritus treated with ultraviolet B phototherapy. J Hepatol 2012; 57: 637.
Hegade VS, et al: Drug treatment of pruritus in liver diseases. Clin Med (London) 2015; 15: 354.
Kremer AE, et al: Pathogenesis and management of pruritus in PBC and PSC. Dig Dis 2015; 33 Suppl 2: 164.
Polycythemia Vera.
More than one third of patients with polycythemia vera report pruritus; it is usually induced by temperature changes or several minutes after bathing. The cause is unknown.
Aspirin has been shown to provide immediate relief from itching; however, there is a risk of hemorrhagic complications. PUVA and NB UVB are also effective. A marked improvement is noted after an average of six treatments, with complete remission often occurring in 2–10 weeks. Paroxetine, 20 mg/day, produced clearing or near-complete clearing in a series of nine patients. Interferon (IFN) alpha-2 has been shown to be effective for treating the underlying disease and associated pruritus.
Saini KS, et al: Polycythemia vera–associated pruritus and its management. Eur J Clin Invest 2010; 40: 828.
Pruritic Dermatoses
Winter Itch
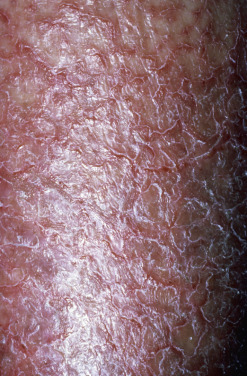
Asteatotic eczema, eczema craquelé, and xerotic eczema are other names for this pruritic condition. Winter itch is characterized by pruritus that usually first manifests and is most severe on the legs and arms. Extension to the body is common; however, the face, scalp, groin, axillae, palms, and soles are spared. The skin is dry with fine flakes ( Fig. 4.4 ). The pretibial regions are particularly susceptible and may develop eczema craquelé, exhibiting fine cracks in the eczematous area that resemble the cracks in old porcelain dishes.
Frequent and lengthy bathing with plenty of soap during the winter is the most frequent cause. This is especially prevalent in elderly persons, whose skin has a decreased rate of repair of the epidermal water barrier and whose sebaceous glands are less productive. Low humidity in overheated rooms during cold weather contributes to this condition. In a study of 584 elderly individuals, the prevalence of asteatosis (28.9%) was second only to seborrheic dermatitis as the most common finding.
Treatment consists of educating the patient on using soap only in the axillae and inguinal area and lubricating the skin with emollients immediately after showering. Preparations containing lactic acid or urea applied after bathing are helpful in some patients but may cause irritation and may worsen itching in patients with erythema and eczema.
For those with more severe symptoms, long-standing disease, or a significant inflammatory component, a regimen referred to as “soaking and smearing” is dramatically effective. The patient soaks in a tub of plain water at a comfortable temperature for 20 minutes before bedtime. Immediately on exiting the tub, without drying, triamcinolone, 0.025%–0.1% ointment, is applied to the wet skin. This will trap the moisture, lubricate the skin, and allow for excellent penetration of the steroid component. An old pair of pajamas is then donned, and the patient will note relief even on the first night. The nighttime soaks are repeated for several nights, after which the ointment alone suffices, with the maintenance therapy of limiting soap use to the axillae and groin, and moisturization after showering. Plain petrolatum may be used as the lubricant after the soaking if simple dryness without inflammation is present. Folliculitis may complicate this therapy.
Gutman A, et al: Soak and smear therapy. Arch Dermatol 2005; 141: 1556.
Kimura N, et al: Prevalence of asteatosis and asteatotic eczema among elderly residents in facilities covered by long-term care insurance. J Dermatol 2013; 40: 770.
Pruritus Ani
Pruritus is often centered on the anal or genital area (less frequently in both), with minimal or no pruritus elsewhere. Anal neurodermatitis is characterized by paroxysms of violent itching, when the patient may tear at the affected area until bleeding is induced. Manifestations are identical to lichen simplex chronicus elsewhere on the body. Specific etiologic factors should always be sought and generally can be classified as dermatologic disease, local irritants (which may coexist with colorectal and anal causes), and infectious agents.
Allergic contact dermatitis is a common dermatologic cause or secondary complication of pruritus ani. It occurs from various medicaments, fragrance in toilet tissue, or preservatives in moist toilet tissue, with one study reporting 18 of 40 consecutive patients being patch test positive. Seborrheic dermatitis, psoriasis, lichen planus, lichen sclerosis, and atopic dermatitis all may cause perianal itching, and an examination of other classic sites of involvement with these conditions should be carefully undertaken. Extramammary Paget disease and Bowen disease, although not often itchy, may be present and will not improve with therapy. Biopsy of resistant dermatitic-appearing skin should be done in nonresponsive pruritus ani.
Irritant contact dermatitis from gastrointestinal contents, such as hot spices or cathartics, or failure to cleanse the area adequately after bowel movements may be causal. Anatomic factors may lead to leakage of rectal mucus on to perianal skin and thus promote irritation. Physical changes such as hemorrhoids, anal tags, fissures, and fistulas may aggravate or produce pruritus.
Mycotic pruritus ani is characterized by fissures and a white, sodden epidermis. Scrapings are examined directly with potassium hydroxide mounts, and cultures will usually reveal Candida albicans, Epidermophyton floccosum, or Trichophyton rubrum. Other sites of fungal infection, such as the groin, toes, and nails, should also be investigated. Erythrasma in the groin and perianal regions may also occasionally produce pruritus. The diagnosis is established by coral red fluorescence under the Wood’s light. β-Hemolytic streptococcal infections have also been implicated, especially in young children. The use of tetracyclines may cause pruritus ani, most often in women, by inducing candidiasis. Diabetic patients are susceptible to perianal candidiasis.
Pinworm infestations may cause pruritus ani, especially in children and sometimes in their parents. Nocturnal pruritus is most prevalent. Other intestinal parasites, such as Taenia solium, T. saginata, amebiasis, and Strongyloides stercoralis, may produce pruritus. Pediculosis pubis may cause anal itching; however, attention is focused by the patient on the pubic area, where itching is most severe. Scabies may be causative but often will also involve the finger webs, wrists, axillae, areolae, and genitalia.
Lumbosacral radiculopathy also may be present with pruritus ani, as assessed by radiographs and nerve conduction studies; paravertebral blockade may help these patients.
Treatment
Meticulous toilet care should be followed, no matter what the cause of the itching. After defecation, the anal area should be cleansed whenever possible, washed with mild soap and water. Cleansing with wet toilet tissue is advisable in all cases. Medicated cleansing pads (Tucks) should be used regularly. A variety of moist toilet tissue products are now available. Contact allergy to preservatives in these products is occasionally a problem. An emollient lotion (Balneol) is helpful for cleansing without producing irritation.
Once the etiologic agent has been identified, a rational and effective treatment regimen may be started. Topical corticosteroids are effective for most noninfectious types of pruritus ani; however, use of topical tacrolimus ointment will frequently suffice and is safer. Pramoxine, a nonsteroidal topical anesthetic, is also often effective, especially in a lotion form combined with hydrocortisone. In pruritus ani, as well as in pruritus scroti and vulvae, it is sometimes best to discontinue all topical medications and treat with plain water sitz baths at night, followed immediately by plain petrolatum applied over wet skin. This soothes the area, provides a barrier, and eliminates contact with potential allergens and irritants.
Abu-Asi MJ, et al: Patch testing is clinically important for patients with peri-anal dermatoses and pruritus ani. Contact Dermatitis 2016; 74: 298.
Nasseri YY, et al: Pruritus ani: diagnosis and treatment. Gastroenterol Clin North Am 2013; 42: 801.
Sahnan K, et al: Anal itching. BMJ 2016; 355: i4931.
Silvestri DL, et al: Pruritus ani as a manifestation of systemic contact dermatitis. Dermatitis 2011; 22: 50.
Suys E, et al: Randomized study of topical tacrolimus ointment as possible treatment for resistant idiopathic pruritus ani. J Am Acad Dermatol 2012; 66: 327.
Pruritus Scroti
The scrotum of an adult is a susceptible site for circumscribed neurodermatitis (lichen simplex chronicus) ( Fig. 4.5 ). Psychogenic pruritus is probably the most frequent type of itching seen. Why it preferentially affects the scrotum, or in women the vulva (see pruritus vulvae ), is unclear. Lichenification may result, can be extreme, and may persist for many years despite intensive therapy.

Infectious conditions may complicate or cause pruritus on the scrotum but are less common than idiopathic scrotal pruritus. Fungal infections, except candidiasis, usually spare the scrotum. When candidal infection affects the scrotum, burning rather than pruritus is frequently the primary symptom. The scrotum is eroded, weepy, or crusted. The scrotum may be affected to a lesser degree in cases of pruritus ani, but this pruritus usually affects the midline, extending from the anus along the midline to the base of the scrotum, rather than the dependent surfaces of the scrotum, where pruritus scroti usually occurs. Scrotal pruritus may be associated with allergic contact dermatitis from topical medications, including steroidal agents.
Topical corticosteroids are the mainstay of treatment, but caution should be exercised. The “addicted scrotum syndrome” may be caused by the use of high-potency topical steroidal agents. As with facial skin, after attempts to wean patients off the steroid, severe burning and redness may occur. Although usually seen after chronic use, this may occur even with short-term high-potency steroids. The scrotum is frequently in contact with inner thigh skin, producing areas of occlusion, which increases the penetration of topical steroid agents. Topical tacrolimus ointment is useful in overcoming the effects of overuse of potent topical steroids. Another alternative is gradual tapering to less potent corticosteroids. Other useful nonsteroidal alternatives include topical pramoxine, doxepin, and simple petrolatum, which is applied after a sitz bath as described for pruritus ani.
Krishnan A, et al: Scrotal dermatitis. Oman Med J 2013; 28: 302.
Tan ES, et al: Effective treatment of scrotal lichen simplex chronicus with 0.1% tacrolimus ointment. J Eur Acad Dermatol Venereol 2015; 29: 1448.
Pruritus Vulvae
The vulva is a common site for pruritus of different causes. Pruritus vulvae ( Fig. 4.6 ) is the counterpart of pruritus scroti. In a prospective series of 141 women with chronic vulvar symptoms, the most common causes were unspecified dermatitis (54%), lichen sclerosus (13%), chronic vulvovaginal candidiasis (10%), dysesthetic vulvodynia (9%), and psoriasis (5%). In prepubertal children, such itching is most frequently irritant in nature, and girls generally benefit from education about improved hygienic measures.

Vaginal candidiasis is a frequent cause of pruritus vulvae. This is true especially during pregnancy and when oral antibiotics are taken. The inguinal, perineal, and perianal areas may be affected. Microscopic examination for Candida albicans and cultures for fungus should be performed. Trichomonas vaginalis infection may cause vulvar pruritus. For the detection of T. vaginalis, examination of vaginal secretions is often diagnostic. The organism is recognized by its motility, size (somewhat larger than a leukocyte), and piriform shape.
Contact dermatitis from sanitary pads, contraceptives, douche solutions, fragrance, preservatives especially in moist towelettes, colophony, benzocaine, corticosteroids, and a partner’s condoms may account for vulvar pruritus. Urinary incontinence should also be considered. Lichen sclerosus is another frequent cause of pruritus in the genital area in middle-age and elderly women. Lichen planus may involve the vulva, resulting in pruritus and mucosal changes, including erosions and ulcerations, resorption of the labia minora, and atrophy.
When burning rather than itching predominates, the patient should be evaluated for signs of sensory neuropathy.
Treatment
Candidiasis and Trichomonas treatments are discussed in Chapters 15 and 20 , respectively. Lichen sclerosus responds best to pulsed dosing of high-potency topical steroids or to topical tacrolimus or pimecrolimus. Topical steroidal agents and topical tacrolimus may be used to treat psychogenic pruritus or irritant or allergic reactions. The use of silk fabric underwear may limit irritation. Patch testing will assist in identifying the inciting allergen. High-potency topical steroids are effective in treating lichen planus, but other options are also available (see Chapter 12 ). Topical lidocaine, topical pramoxine, or an oral tricyclic antidepressant (TCA) may be helpful in select cases. Phototherapy using a comb light device may be effective. Any chronic skin disease that does not respond to therapy should prompt a biopsy.
Caro-Bruce E, et al: Vulvar pruritus in a postmenopausal woman. CMAJ 2014; 186: 688.
Haverhock E, et al: Prospective study of patch testing in patients with vulvar pruritus. Australas J Dermatol 2008; 49: 80.
Ozalp SS, et al: Vulval pruritus. J Obstet Gynaecol 2015; 35: 53.
Utas S, et al: Patients with vulvar pruritus. Contact Dermatitis 2008; 58: 296.
Virgili A, et al: Phototherapy for vulvar lichen simplex chronicus. Photodermatol Photoimmunol Photomed 2014; 30: 332.
Puncta Pruritica (Itchy Points)
“Itchy points” consists of one or two intensely itchy spots in clinically normal skin, sometimes followed by the appearance of seborrheic keratoses at exactly the same site. Curettage, cryosurgery, punch biopsy, or botulinum toxin A injection of the itchy points may cure the condition.
Boyd AS, et al: Puncta pruritica. Int J Dermatol 1992; 31: 370.
Salardini A, et al: Relief of intractable pruritus after administration of botulinum toxin A. Clin Neuropharmacol 2008; 31: 303.
Aquagenic Pruritus and Aquadynia
Aquagenic pruritus is itching evoked by contact with water of any temperature. Most patients experience severe, prickling discomfort within minutes of exposure to water or on cessation of exposure to water. There are two groups of patients: about one third consist of an older, primarily male population who have polycythemia vera, hypereosinophilic syndrome, or myelodysplastic syndrome, and two thirds are younger women who develop aquagenic pruritus as young adults and who have no known underlying disease and may have a family history of similar symptoms.
Aquagenic pruritus must be distinguished from xerosis as water may be perceived as an irritant in severely dry skin, and in these cases an initial trial of “soaking and smearing,” as previously described for winter itch, is recommended. Treatment options for aquagenic pruritus include the use of antihistamines, sodium bicarbonate dissolved in bath water, propranolol, atenolol, SSRIs, acetylsalicylic acid (ASA, aspirin), pregabalin, montelukast, and NB UVB or PUVA phototherapy. One patient found tight-fitting clothing settled the symptoms after only 5 minutes.
Shelley et al. reported two patients with widespread burning pain that lasted 15–45 minutes after water exposure, calling this reaction “aquadynia” and considering the disorder a variant of aquagenic pruritus. Clonidine and propranolol seemed to provide some relief.
Cao T, et al: Idiopathic aquagenic pruritus. Dermatol Ther 2015; 28: 118.
Heitkemper T, et al: Aquagenic pruritus. J Dtsch Dermatol Ges 2010; 8: 797–804.
Herman-Kideckel SM, et al: Successful treatment of aquagenic pruritus with montelukast. J Cut Med Surg 2012; 16: 151–152.
Koh MJA, et al: Aquagenic pruritus responding to combine ultraviolet A/narrowband ultraviolet B therapy. Photodermatol Photoimmunol Photomed 2009; 25: 169–170.
Shelley WB, et al: Aquadynia. J Am Acad Dermatol 1998; 38: 357.
Scalp Pruritus
Pruritus of the scalp, especially in elderly persons, is rather common. Lack of excoriations, scaling, or erythema excludes inflammatory causes of scalp pruritus such as seborrheic dermatitis, psoriasis, dermatomyositis, or lichen simplex chronicus. Most such cases remain are neuropathic or idiopathic, but some represent chronic folliculitis. Treatment with topical tar shampoos, salicylic acid shampoos, corticosteroid topical gels, mousse, shampoos, and liquids can be helpful. In patients who have severe scalp pruritus with localized itch, an intralesional injection of corticosteroid suspension may provide relief. Minocycline or oral antihistamines may be helpful. In other patients, low doses of antidepressants, such as doxepin, are useful.
Cohen AD, et al: Similarities between neuropathic pruritus sites and lichen simplex chronicus sites. Isr Med Assoc J 2014; 16: 88.
Shumway NK, et al: Neurocutaneous disease: Neurocutaneous dysesthesias. J Am Acad Dermatol 2016; 74: 215.
Drug-Induced Pruritus
Medications should be considered a possible cause of pruritus with or without a skin eruption. For example, pruritus is frequently present after opioid use. Also, chloroquine and to a lesser degree other antimalarials produce pruritus in many patients, especially African Americans, treated for malaria. SSRIs and drugs causing cholestatic liver disease are other frequent causes.
Hydroxyethyl starch (HES) is used as a volume expander, a substitute for human plasma. One third of all patients treated will develop severe pruritus with long latency of onset (3–15 weeks) and persistence. Up to 30% of patients have localized symptoms. Antihistamines are ineffective.
Ebata T: Drug-induced itch management. Curr Probl Dermatol 2016; 50: 155.
Ständer S, et al: Hydroxyethyl starch-induced pruritus. Acta Derm Venereol 2014; 94: 282.
Chronic Pruritic Dermatoses of Unknown Cause
Prurigo simplex is the preferred term for the chronic itchy idiopathic dermatosis described here. Papular dermatitis, subacute prurigo, “itchy red bump” disease, urticarial dermatitis, the eruption of senescence of Berger, and Rosen papular eruption in black men most likely represent variations of prurigo simplex. The term prurigo continues to lack nosologic precision.
Prurigo simplex is characterized by the lesion known as the prurigo papule, which is dome shaped and topped with a small vesicle. The vesicle is usually present only transiently because of its immediate removal by scratching, so that a crusted papule is more frequently seen. Prurigo papules are present in various stages of development and are seen mostly in middle-age or elderly persons of both genders. The trunk and extensor surfaces of the extremities are common sites, symmetrically distributed. Other areas include the face, neck, lower trunk, and buttocks. The lesions usually appear in crops, so that papulovesicles and the late stages of scarring may be seen at the same time. At times eczematous morphology may be intermixed.
The histopathology of prurigo simplex is nonspecific but often suggests an arthropod reaction. Spongiosis accompanied by a perivascular mononuclear infiltrate with some eosinophils is often found.
Many conditions may cause pruritic erythematous papules. Scabies, atopic dermatitis, insect bite reactions, papular urticaria, dermatitis herpetiformis, contact dermatitis, pityriasis lichenoides et varioliformis acuta (PLEVA), transient acantholytic dermatosis (TAD), papuloerythroderma of Ofuji, dermatographism, and physical urticarias should be considered. Biopsy may be helpful in differentiating dermatitis herpetiformis, PLEVA, TAD, and on occasion, unsuspected scabies.
Treatment
The medications for initial treatment of prurigo simplex and its variants should be topical corticosteroids and oral antihistamines. Early in the disease process, moderate-strength steroids should be used; if the condition is found to be unresponsive, a change to high-potency forms is indicated. “Soaking and smearing” may be necessary. Intralesional injection of triamcinolone will eradicate individual lesions. For more recalcitrant disease, UVB or PUVA therapy may be beneficial. If such interventions do not provide relief, low-dose azathioprine, mycophenolate, or methotrexate may be needed.
Berger TG, et al: Pruritus in elderly patients—eruptions of senescence. Semin Cutan Med Surg 2011; 30: 113.
Clark AR, et al: Papular dermatitis (subacute prurigo, “itchy red bump” disease). J Am Acad Dermatol 1998; 38: 929.
Hannon GR, et al: Urticarial dermatitis. J Am Acad Dermatol 2014; 70: 264.
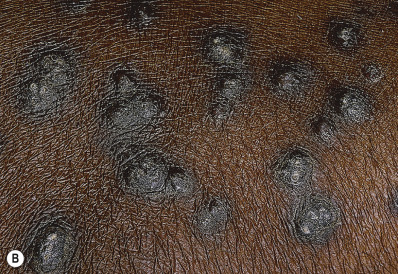
Prurigo Pigmentosa
Prurigo pigmentosa is a rare dermatosis of unknown cause characterized by the sudden onset of erythematous papules or vesicles that leave reticulated hyperpigmentation when they heal ( Fig. 4.7 ). The condition mainly affects Japanese, although numerous cases have been reported in Caucasians. Women outnumber men 2 : 1. The mean age of onset is 25. It is associated with weight loss, dieting, anorexia, post bariatric surgery, pregnancy, diabetes, and ketonuria. It is exacerbated by heat, sweating, and friction and thus occurs most often in the winter and spring. The areas most frequently involved are the upper back, nape, clavicular region, and chest. Mucous membranes are spared. Histology of early lesions shows neutrophils in the dermal papillae and epidermis. Following this, a lichenoid dermatitis with variable psoriasiform hyperplasia occurs. Direct immunofluorescence yields negative findings. The cause is unknown. Minocycline, 100–200 mg/day, is the treatment of choice. Dapsone and alteration of the diet are also effective; topical steroids are not effective. Recurrence and exacerbations are common.
Beutler BD, et al: Prurigo pigmentosa. Am J Clin Dermatol 2015; 16: 533.
Hijazi M, et al: Prurigo pigmentosa. Am J Dermatopathol 2014; 36: 800–806.
Zeng X, et al: Prurigo pigmentosa. J Eur Acad Dermatol Venereol 2016; 30: 1794.










