Abstract
The anatomical components of facial aging include the skin, fat compartments, mimetic muscles, ligamentous support, and bony skeleton. Understanding the underlying processes that govern facial aging is important to be able to properly examine the patient. A detailed preoperative facial analysis requires both a gross overview of the face and its asymmetries, along with a focused examination of the various parts of the face: forehead, periorbital, midface, nose, perioral, chin, and neck. Surgical and nonsurgical options are available to treat the aging face. Skin care is a universal aspect in plastic surgery and is particularly important for the aging face.
5 The Facial Aging Face Consultation
Key Points
The anatomical components to facial aging include the skin, fat compartments, mimetic muscles, ligamentous support, and bony skeleton.
Understanding the underlying processes that govern facial aging is important to be able to properly examine the patient.
A detailed preoperative facial analysis requires both a gross overview of the face and its asymmetries, along with a focused examination of the various parts of the face: forehead, midface, periorbital, perioral, and neck.
Surgical and nonsurgical options are available to treat the aging face.
Skin care is a universal aspect to facial plastic surgery and is particularly important for the aging face.
5.1 Components of Aging
The combination of facial fat descent, attenuation of retaining ligaments, and diminished fat volume and skeletal support produces the characteristic changes associated with the aging face.
5.1.1 Fat
Gravity is a constant force applied to the structural fat compartments and bony contours of the face.
Changes in facial fat during facial aging can be understood as either (1) volume loss, or (2) change in volume distribution.
Landmark studies by Rohrich and Pessa described anatomical units of deep and superficial fat compartments of the face, separated by distinct septae.3 These fibrous septae of connective tissue extend from the fascial layer to the dermis (Fig. 5.1).
There are 22 superficial facial fat compartments:
Forehead: Central, middle temporal, lateral temporal-cheek.
Periorbital: One supraorbital fat compartment and two infraorbital fat compartments.
Midface: Nasolabial, medial cheek, middle cheek, lateral temporal-cheek (same as above).
Lower face: Two jowl fat compartments and submental fat compartment.
Three key fat compartments that influence midface volume loss are the nasolabial, deep medial, and deep lateral fat compartments. The deep midfacial fat compartment is medial to the zygomaticus major muscle (Fig. 5.2).
Change in volume distribution is attributed to the decline in the structural supportive function of the facial ligaments. Lambros described “radial expansion” of the soft tissues of the face as a result of weakening of the fibrous attachments between skin, fat, and deep fascia resulting in an outward expansion from the bony skeleton.
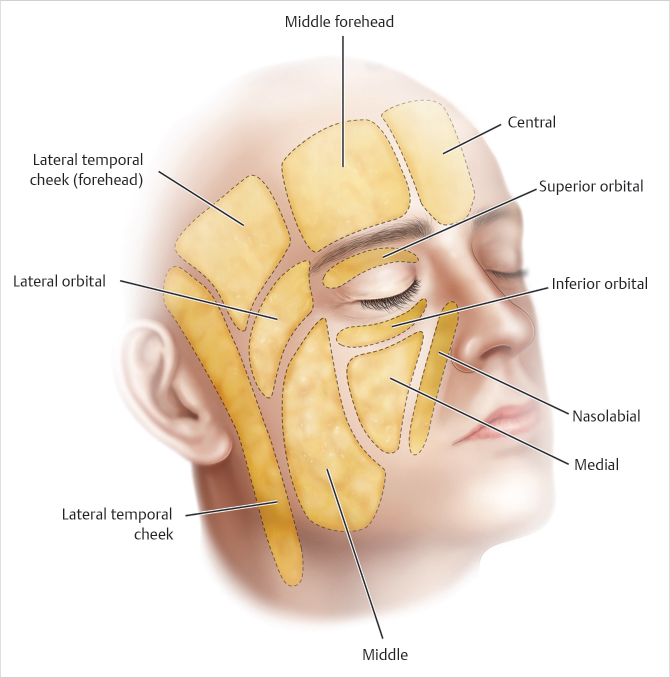
Fig. 5.1 Superficial fat compartments of the face.
(Reproduced with permission from Leatherbarrow B, ed. Oculoplastic Surgery. 3rd ed. Thieme; 2019.)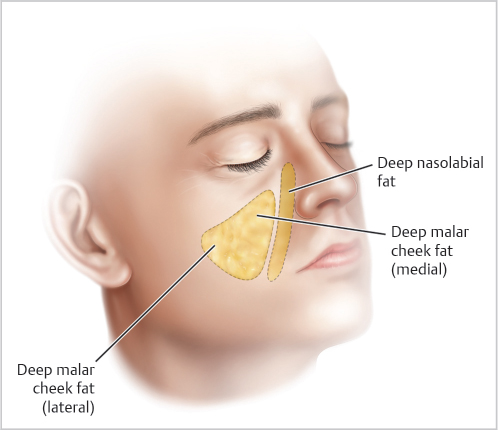
Fig. 5.2 Key fat compartments relevant to facial rejuvenation.
(Reproduced with permission from Rohrich R, Ahmad J, eds. The Dallas Rhinoplasty and Dallas Cosmetic Surgery Dissection Guide. 1st ed. Thieme; 2018.)
5.1.2 Skeletal
The morphologic changes of the facial bony skeleton impact the soft tissues of the face.
Prior studies have demonstrated skeletal changes in orbit, maxilla, and mandible influencing the relative prominence and position of facial soft tissues.
5.1.3 Muscle
Volumetric changes in the facial bones and fat compartments impact the facial mimetic muscles with changes in laxity and muscle tension.
5.1.4 Skin
The aging skin reflects the effect of a series of factors that influence the appearance of skin. These include speech and animation, sun and environmental exposure, weight changes, medical health, and other insults including smoking.
Collagen and elastin are the primary components of the skin. Toxic injury to these components lead to the process of aging. Atrophy of skin appendages and decreased extracellular matrix of the skin further influence the overall thinning of skin with age.
5.2 Consultation
An individualized approach to facial rejuvenation allows maximal patient satisfaction.
The surgeon should spend the initial minutes of the consultation listening to the patient’s concerns about his or her appearance. Common concerns with facial aging focus on the periorbital and neck regions.
5.2.1 Medical History
Medical and surgical history should be taken to identify any potential reasons for delayed wound healing or bleeding.
A complete list of medications should be obtained. This includes both prescribed and over-the-counter medications that can cause bleeding during a procedure (anticoagulant, antiplatelet, antihypertensives, immunosuppressive, hormone replacement medications).
Herbal medications may cause bleeding. Patients should be specifically asked if they are taking any herbal supplements (Remember the four G’s: Ginger, Ginkgo biloba, Garlic, or Ginseng).
Smoking history.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


