Abstract
Facelift and necklift incision planning is a critical aspect of the facelift and necklift operation. It directly influences the final aesthetic result. Detailed preoperative assessment and proper incision design will influence both scar placement and quality. Proper scar placement should highlight regional anatomic proportions and subunits, rather than the scar itself. Understanding the anatomic subunits of the preauricular incision will guide the surgeon during incision design and preserve the intricacies of this anatomy. Tension free closure is an important requirement for optimal wound healing. A systematic approach to skin excision and closure helps to provide consistency in results.
6 Facelift and Necklift: Incision Planning
Key Points
A detailed analysis must be performed prior to incision planning to minimize secondary deformities in the facelift and necklift patient.
Proper scar placement should highlight regional anatomic proportions and subunits, rather than the scar itself.
Incision design and tension free closure are primary factors for optimal scar quality and location.
6.1 Preoperative Steps
The facelift and necklift incisions are comprised of four segments: Temporal, preauricular, retroauricular, and occipital. Additionally, the necklift operation has a separate submental incision.
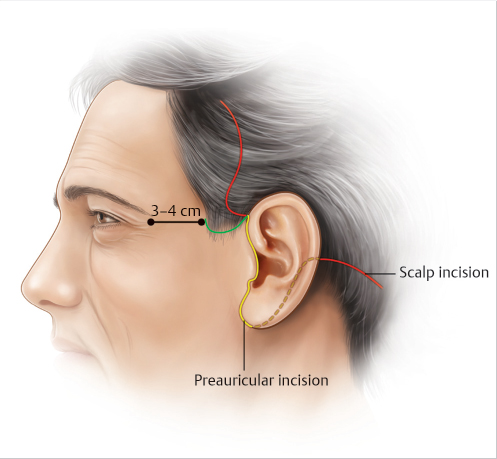
6.1.1 Temporal Incision (Fig. 6.1)
Options for incision placement include (1) within hair-bearing region, posterior to temporal hairline, or (2) anteriorly, along the temporal hairline.
Youthful individuals have approximately 4 cm of distance between lateral canthus and anterior temporal hairline.
In patients with minimal skin redundancy, the incision may be placed behind the temporal hairline without a noticeable change in hairline position.
Connell described a prehelical flap that serves as a “rescue flap.” This avoids a hairless notch above the root of the helix when performing this temporal incision (Fig. 6.1).
Appropriate rotation of the facial skin in a lateral vector will avoid vertical displacement of temporal hair and side burn elevation.
The anterior temporal hairline is an alternative approach but can result in a visible scar in some patients with an abrupt transition between the cheek and the temporal hair.
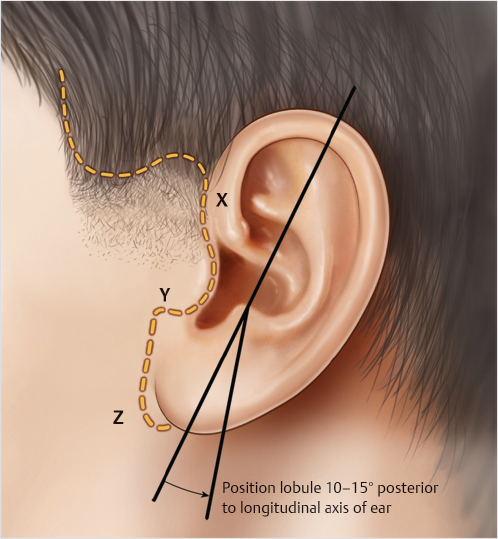
6.1.2 Preauricular Incision (Fig. 6.2)
There are five subunits in the preauricular aesthetic: helix width, pretragal hollow, tragal height, superior and inferior intertragal notches, and earlobe–cheek junction. They should be carefully respected when designing the preauricular portion of the incision.
The preauricular incision can be divided into three segments: helix, tragus, and lobule.
Helix:
This portion is a parallel curve to the posterior helical margin.
It should mimic the visual transverse width (X) of the helical cartilage (Fig. 6.2).
The hypopigmented scar will help create a normal appearing helical margin of anatomic proportion.
Tragus:
The tragal cartilage is a rectangular structure. Close attention to its anatomical subunits will allow for precise incision placement.
After the helical segment, the incision follows the depression of the superior intertragal notch.
The incision is then carried along the tragal rim to the inferior intertragal notch.
The intratragal incision is preferred in men as they provide a better disguise for the color difference between the whiter ear skin and the blush colored cheek skin.
From here, the incision turns anteriorly before turning again inferiorly at a 90-degree angle, anterior to the lobular-facial sulcus. This preserves the inferior intertragal notch, which would otherwise be blunted (Fig. 6.2).
Lobule:
The incision at the perilobular region should preserve 2 mm of natural sulcus between the earlobe and cheek.
Secondary deformity in the preauricular segment is seen when the incision does not properly follow the helical or tragal cartilages as detailed. An anteriorly placed incision results in a conspicuous scar.
In males, more so than females, the preauricular region may have varied color gradient and surface irregularity. An incision placed in the preauricular crease may still risk the potential for a visible scar.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


