Abstract
Modern facelift techniques have advanced in terms of better understanding of anatomy and maneuvers that produce the longest-lasting results. What was once a skin-only procedure has now evolved into surgery that addresses deeper tissues (superficial musculoaponeurotic system [SMAS] and platysma) independent of the skin, with a high degree of safety and a relatively short recovery period.
11 SMAS Plication with Extended Platysma–SMAS Flap
Key Points
The superficial musculoaponeurotic system (SMAS) plication must be planned and executed meticulously.
Adequate SMAS plication can achieve improvement in the volume over the zygoma, restore malar deflation, and correct lower facial laxity.
Release of the submental crease, mandibular retaining ligaments, and platysma retaining ligaments allows for effective skin redraping and smooth chin and jawline contour.
11.1 Preoperative Steps
11.1.1 Planning
Patients are encouraged to bring their youth photographs.
Although limitations are discussed, a similar shape and greatly improved appearance can be obtained reliably.
Almost always, the two sides of the face will be noticeably asymmetric. For instance, there will be a dominant cheek, wider palpebral aperture, long and short side, asymmetric brows, etc. These differences should be noted preoperatively.
Skin quality, elasticity, extent of soft tissue descent (i.e., jowling), and underlying bony support are evaluated, as these qualities will all influence the final result.
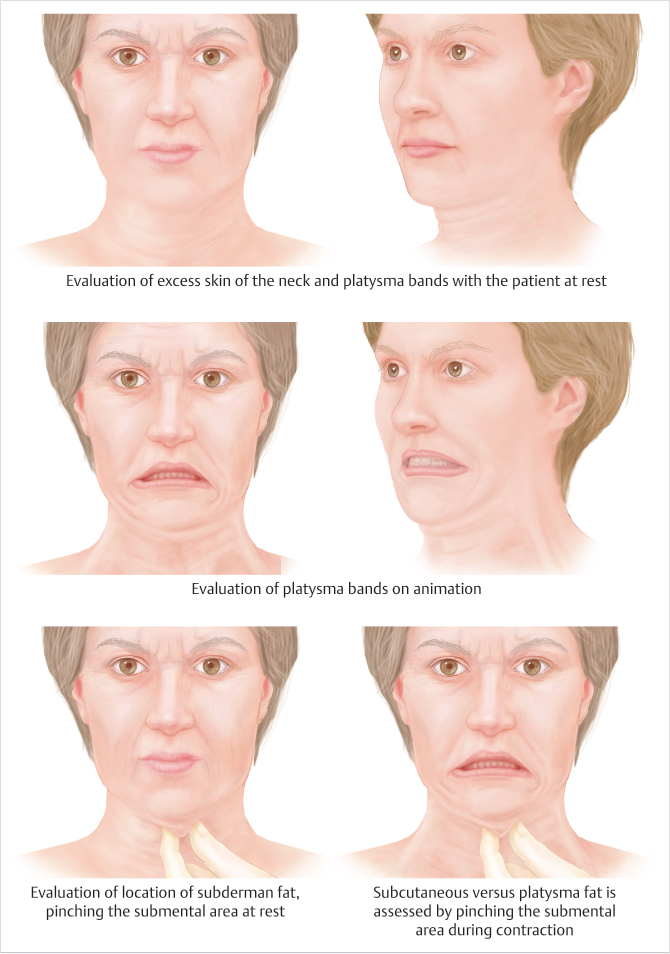
The neck is evaluated at rest and by having the patient tense the platysma muscle (i.e., grimace). Significant banding, an obtuse cervicomental angle, indistinct thyroid cartilage bulge, noticeable pre- and subplatysmal fat, and excess skin are all signs of neck aging (Fig. 11.1).
If patients exhibit significant signs of deflation in addition to descent of facial soft tissues, then autologous fat grafting should be considered.
11.2 Operative Steps
See Video 11.1.
11.2.1 Preparation
The patient is marked preliminarily in the preoperative holding area and then brought to the operating room.
After administration of general anesthesia, a neurosurgical headrest is used to allow proper head positioning and to allow the surgeon to operate slightly closer to the patient.
A solution consisting of 150 cc of normal saline, 50 cc of 1% lidocaine, and 1 ampule of epinephrine is injected into the neck and the first side of the face.
11.2.2 Open Neck Treatment
A #10 blade is used to open the submental incision and undermine the flap for 1 or 2 cm.
Facelift scissors are then used to elevate the subcutaneous flap above the platysma muscle down to the level past the thyroid cartilage, commonly caudal to the first cervical crease.
A single port liposuction cannula is used to remove fat off the medial borders of the left and right platysma muscle for better visualization.
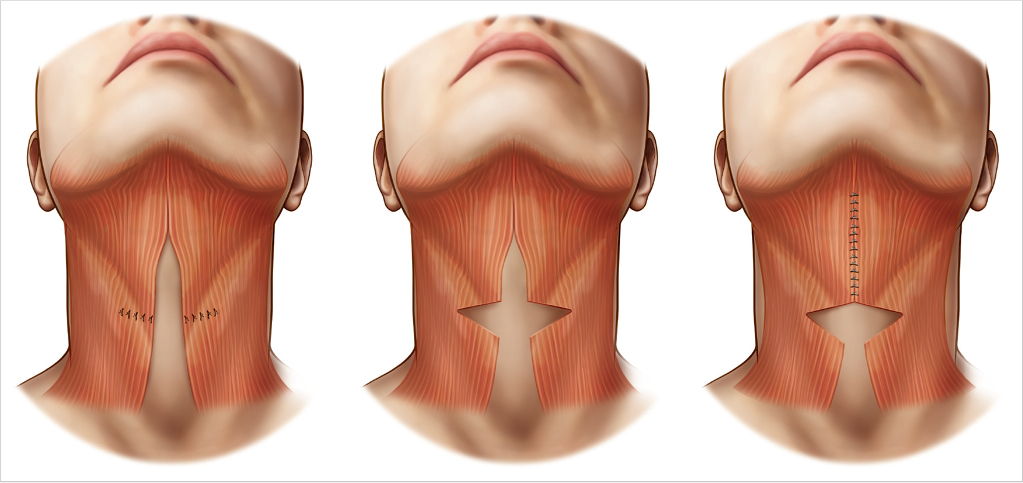
Interrupted 3–0 buried Mersilene sutures are placed to approximate the platysma in the midline (starting at the thyroid cartilage and working up), followed by a running layer on top of this repair (with 3–0 or 4–0 Mersilene).
Commonly at this point, a several centimeter wedge of platysma is resected caudal to the repair if significant banding is present; this maneuver breaks the continuity of the band (Fig. 11.2).
Hemostasis is achieved; then a temporary gauze is placed.
11.2.3 Lateral Approach
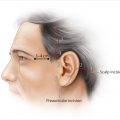
Either a pretragal or retrotragal incision is used. With the exception of secondary cases, an incision hidden in the temporal hair is also used. A full retrotragal incision is used in an S-shaped pattern, with a small non-hair bearing segment of incision in the retroauricular sulcus, which is covered by the ear.
After making the preauricular stab incisions, the cheek flap is preliminarily undermined by suctioning with a 2.4-mm cannula. This facilitates flap dissection.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


