Abstract
In 1992, the senior author (Daniel C. Baker) discovered that an alternative to formally elevating the superficial musculoaponeurotic system (SMAS) flap was to perform a “lateral SMASectomy” by removing a portion of the SMAS in the region of its fixed and mobile junction. Excision and suturing of the superficial fascia in this region allow the surgeon to achieve results similar to a formal SMAS flap, but the technique is simpler and less invasive. The width of SMAS resection depends upon the fullness of the patient’s face and whether debulking is advantageous. However, in order to preserve facial fat in thin patients, SMASectomy is not performed. Instead, SMAS plication is performed in these patients to augment and sculpt the face.
8 SMASectomy
Key Points
There are several advantages of lateral SMASectomy in comparison with traditional superficial musculoaponeurotic system (SMAS) elevation.
The procedure does not require traditional SMAS flap elevation. There is less concern about tearing of the superficial fascia.
The potential for facial nerve injury is less because most of the deep dissection is over the parotid gland.
If SMAS flaps are not elevated, they tend to hold suture fixation more strongly, and the potential for postoperative dehiscence and relapse of contour is decreased.
The design of the lateral SMASectomy is along the anterior border of the parotid.
The SMASectomy is performed at the interface of the superficial fascia fixed by the retaining ligaments and the more mobile anterior superficial facial fascia. Upon closure, this brings the mobile SMAS up to the junction of the fixed SMAS producing a durable elevation of both superficial fascia and facial fat.
8.1 Preoperative Steps
8.1.1 Instructions for Patients to Reduce the Incidence of Infection
Wash neck, behind the ears, and the external ear canal with Hibiclens soap twice daily for 5 days preoperatively. DO NOT USE ON FACE.
Shampoo hair daily including morning of surgery.
Use Bactroban ointment (mupirocin 2%—prescription). Swab the inside of each nostril and the external ear canal (DO NOT PUT DEEP INSIDE).
8.1.2 Anesthesia
All facelifts are performed under monitored intravenous propofol sedation.
Patients are given oral clonidine, 0.1 to 0.2 mg, 30 minutes prior to surgery to control their blood pressure.
The face and neck are infiltrated with local anesthesia, 0.5% lidocaine with 1:200,000 epinephrine, through use of a 22-gauge spinal needle.
The face is injected prior to scrubbing in order to provide the requisite 10 minutes for vasoconstriction.
8.2 Operative Steps
See Video 8.1.
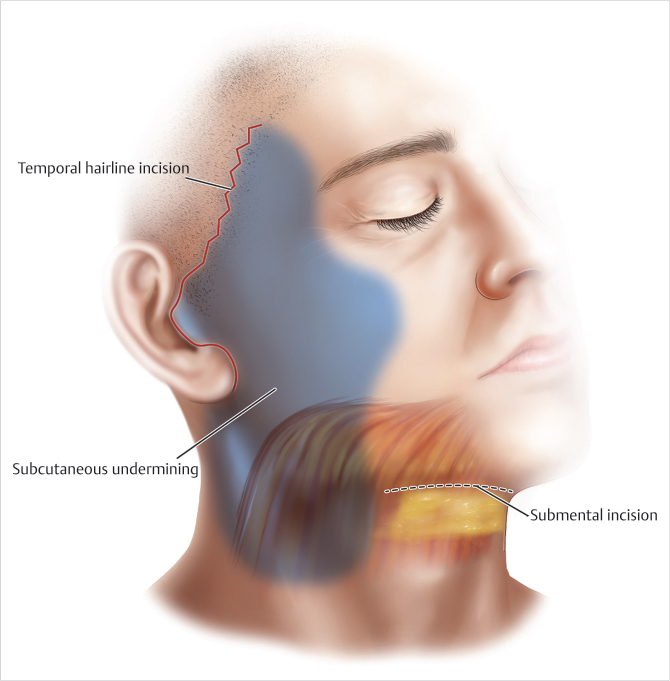
8.2.1 Incisions
If the temporal hairline shift is assessed as minimal, the preferred incision is within the temporal hair. In this incision, it is often necessary to excise a triangle of skin below the temporal sideburn at the level of the superior root of the helix to preserve the sideburn.
When a larger skin shift is anticipated, if the distance between the lateral canthus and temporal hairline is greater than 5 cm, a beveled incision a few millimeters within the temporal hairline is preferable. This is an effort to avoid the alternative of a receding temporal hairline, which is usually never acceptable for a female patient.
The choice of preauricular incision is up to the surgeon. When executed properly, all of these incisions heal well and are imperceptible. The senior author (Daniel C. Baker) prefers a curved incision anterior to the helix, which then continues inferiorly anterior to the tragus in a natural skin fold.
Intratragal incisions are carried out in those patients whose cheek and tragal skin are similar, and the tragal cartilage is not sharp or prominent. Closure must be performed without tension, and the flap overlying the tragus is defatted to dermis.
8.2.2 Skin Flap Elevation
All skin flap undermining is performed under direct vision (with scissors dissection) to minimize trauma of the subdermal plexus and preserve 5 mm of subcutaneous fat on the undersurface of the flap.
Subcutaneous dissection in the temporal region is preferable because the skin seems to redrape better. Subcutaneous dissection in the temporal region must be performed carefully to avoid penetrating the superficial temporal fascia that protects the frontal branch of the facial nerve.
All dermal attachments between the orbicularis oculi muscle and the skin are separated up to the lateral canthus (Fig. 8.1).
Dissection extends across the zygoma to release zygomatic ligaments but stops several centimeters short of the nasolabial fold. The senior author does not believe that further dissection provides significant benefits; on the contrary, the only result is increased bleeding.
In the cheek, dissection releases the masseteric-cutaneous ligaments and, if necessary, the mandibular ligaments.
Subcutaneous dissection continues over the angle of the mandible and sternocleidomastoid for 5 to 6 cm into the neck, which exposes the posterior half of the platysma on muscle. If a submental incision has been made, the facial and lateral neck dissection is connected through and through to the submental dissection.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


