A nutritional disease is caused either by insufficiency or, less often, by excess of one or more dietary essentials. Nutritional deficiencies are particularly common in developing countries but can also occur due to fad diets or restrictive eating practices in patients with behavioral or autism spectrum disorders. Infants and children are particularly at risk for deficiency states, especially malnutrition. Infants diagnosed with multiple food allergies who substitute other nutrition such as rice milk for breast milk or standard baby formulas are at particular risk. Frequently, patients have features of several nutrient deficiencies if their diet has generally been restricted. An intertriginous or acral eruption, a seborrheic dermatitis–like facial eruption, atrophic glossitis, and alopecia are common features of many nutritional deficiencies. This occurs because these nutrients are essential to overlapping metabolic pathways of fatty acid metabolism, resulting in abnormal differentiation of the epidermis and defective barrier function. The histologic findings in many types of nutritional dermatosis are also similar.
In developed countries, alcoholism is the main cause of nutritional diseases in adults. Nutritional diseases should also be suspected in postoperative patients; psychiatric patients, including those with anorexia nervosa and bulimia; patients on the autism spectrum who have textural issues with certain foods; patients on restrictive diets; patients with surgical or inflammatory bowel dysfunction, especially Crohn disease; patients who have had bowel bypass surgery; cystic fibrosis patients; and patients with severe oral erosive disease (e.g., pemphigus) that prevents eating. In the pediatric setting, nutritional deficiency may also occur because of parental ignorance of the nutritional requirements or restriction due to concern for perceived or actual food allergies.
The diagnosis of nutritional deficiency is often missed because physicians fail to take an adequate dietary history. When children have protein malnutrition, their albumin is low and thus cannot serve its role as an osmotic agent to hold serum in the vessels. Therefore children will gain weight, which clinically masks their severe deficiency in protein. The dermatitis produced by elevated glucagon levels from islet cell tumors of the pancreas (necrolytic migratory erythema) and a similar dermatosis seen in hepatitis C infection and other forms of hepatic insufficiency (necrolytic acral erythema, pseudoglucagonoma) probably also represent nutritional deficiency dermatoses. Deficiency states caused by inborn errors of metabolism are discussed in Chapter 26 . In many cases, the clinical findings and socioeconomic scenario are adequate to lead to suspicion of a specific deficiency state, and replacement therapy can confirm the diagnosis. Laboratory testing may be costly and inaccurate in some deficiency states, and patients with poor nutrition are often deficient in many nutrients simultaneously. Testing is indicated to confirm the diagnosis of zinc deficiency, as well as the inborn errors of metabolism that can mimic zinc deficiency, such as propionyl-CoA carboxylase deficiency, methylmelnonic acidemia, isoleucine deficiency, holocarboxylase synthetase deficiency, and biotinidase deficiency; to assess essential fatty acid (EFA) deficiency; and to evaluate for possible glucagonoma syndrome in a child.
Vitamin A
Hypovitaminosis A (Phrynoderma)
Vitamin A is a fat-soluble vitamin found as retinyl esters in milk, fish oil, liver, and eggs and as carotenoids in plants. Vitamin A deficiency is common in children in the developing world. It is rare in developed countries, where it is most often associated with diseases of fat malabsorption, such as bowel bypass surgery for obesity, pancreatic insufficiency, Crohn disease, inflammatory bowel disease (IBD), celiac disease, cystic fibrosis, and liver disease. Vitamin A is required for the normal keratinization of many mucosal surfaces. When it is deficient, the resultant abnormal keratinization leads to increased mortality risk from inflammatory disease of the gut and lung—diarrhea and pneumonia (especially in measles). Vitamin A supplementation of 200,000 IU/day for 2 days is recommended for children with measles; this may also prevent the risk of blindness.
Although phrynoderma had classically been ascribed to, and thought to be specific for, vitamin A deficiency, this clinical sign is in fact most frequently found as a disorder of multiple deficiencies, including vitamins A, B, C, and E and EFAs. Replacing all these deficiencies leads to rapid improvement. This explains patients in whom the cutaneous findings of phrynoderma were found without the classic eye findings of vitamin A deficiency. The skin eruption, termed follicular hyperkeratosis or phrynoderma (“toadskin”), resembles keratosis pilaris and the genodermatosis keratosis follicularis spinuloas decalvans. It consists of keratotic papules of various sizes distributed symmetrically over the extremities and shoulders, surrounding and arising from the pilosebaceous follicles ( Fig. 22.1 ). Individual lesions are usually asymptomatic firm, pigmented papules containing a central, intrafollicular keratotic plug that projects from the follicle as a horny spine and leaves a pit when expressed. Lesions are of two sizes: 1–2 mm papules closely resembling keratosis pilaris and the more diagnostic, large, 2–6 mm, crateriform papules filled with a central keratotic plug. These latter lesions may simulate a perforating disorder. The eruption of small lesions usually begins on the anterolateral aspect of the thighs or the posterolateral aspect of the upper arms, although one study showed that the elbows were the most common initial site in 84%. It then spreads to the extensor surfaces of both the upper and the lower extremities, the shoulders, abdomen, back, and buttocks and finally reaches the face and posterior aspect of the neck. The hands and feet are not involved, and lesions occur only occasionally on the midline of the trunk or in the axillary and anogenital areas. On the face, the eruption resembles acne because of the presence of many large comedones, but it differs from acne in regard to dryness of the skin. The large, dome-shaped nodules are on the elbows and knees and have a surrounding red or brown rim. There is generalized dryness, fine scaling, and hyperpigmentation. Hair casts may also be seen.

Vitamin A deficiency may mimic vitamin C deficiency (scurvy) because both conditions cause follicular hyperkeratosis, although the characteristic follicular hemorrhage is more prominent in vitamin C deficiency. Bleeding and gingival disease can be a feature of vitamin A deficiency as well as scurvy. The histologic findings of “deficiency dermatitis,” which are common to many deficiency states (zinc, EFAs, amino acids, glucagonoma, cystic fibrosis), are not features of either vitamin A or vitamin C deficiency.
In vitamin A deficiency, eye findings are prominent and often pathognomonic. These include night blindness, an inability to see bright light, xerophthalmia, xerosis corneae, and keratomalacia. The earliest finding is delayed adaptation to the dark (nyctalopia). Some patients have circumscribed areas of xerosis of the conjunctiva lateral to the cornea, occasionally forming well-defined white spots (Bitot spots); these are triangular, with the apex toward the canthus. Vitamin A deficiency is a major cause of blindness in children in developing countries.
The histologic findings of vitamin A deficiency are hyperkeratosis, horny plugs in the upper portion of the hair follicle, coiled hairs in the upper part of the follicle, severe atrophy of the sebaceous glands, and squamous metaplasia of the secretory cells of the eccrine sweat glands. If the follicles rupture, perifollicular granulomatous inflammation is found.
The diagnosis of vitamin A deficiency is confirmed by determination of the serum retinol level. The treatment is oral vitamin A, 100,000 IU/day for 2–3 days, followed by the recommended dietary requirement. Serum retinol levels are monitored to determine adequacy of supplementation and to avoid vitamin A toxicity.
Hypervitaminosis A
The skin findings of hypervitaminosis A are similar to the side effects of synthetic retinoid therapy (such as isotretinoin). Children are at greater risk for toxicity than adults. Excess megavitamin ingestion may be the cause. In adults, doses as small as 25,000 IU/day may lead to toxicity, especially in persons with hepatic compromise from alcoholic, viral, or medication-induced hepatitis. Patients on dialysis also are at increased risk, because vitamin A is not removed by dialysis. Standard hyperalimentation solutions contain significant amounts of vitamin A, and in burn victims with renal compromise, vitamin A toxicity can occur. If the patient is taking a synthetic retinoid, all vitamin A supplementation should be stopped.
Most cases of chronic hypervitaminosis A have been reported in children. There is loss of hair and coarseness of the remaining hair, loss of the eyebrows, exfoliative cheilitis, generalized exfoliation and pigmentation of the skin, and clubbing of the fingers. Moderate widespread itching may occur. Hepatomegaly, splenomegaly, hypochromic anemia, depressed serum proteins, and elevated liver function tests may be found. Bone growth may be impaired by premature closure of the epiphyses in children. Pseudotumor cerebri with papilledema may occur early, before any other signs appear. In infants, this may present as a bulging fontanelle.
In adults, the early signs are dryness of the lips and anorexia. These symptoms may be followed by joint and bone pains, follicular hyperkeratosis, branny desquamation of the skin, fissuring of the corners of the mouth and nostrils, dryness and loss of scalp hair and eyebrows, and dystrophy of the nails. Fatigue, myalgia, depression, anorexia, headache (from pseudotumor cerebri), strabismus, and weight loss frequently occur. Liver disease may be progressive and may lead to cirrhosis with chronic toxicity. Hypercalcemia often occurs in dialysis patients and be worsened by the hypervitaminosis A. Retinoids are teratogens, and birth defects may occur with excess vitamin A supplementation during pregnancy.
Bello S, et al: Routine vitamin A supplementation for the prevention of blindness due to measles infection in children. Cochrane Database Syst Rev 2016; 8: CD007719.
Bremner NA, et al: Vitamin A toxicity in burns patients on long-term enteral feed. Burns 2007; 22: 266.
Brown CA, et al: Medical complications of self-induced vomiting. Eat Disord 2013; 21: 287.
Cheruvattath R, et al: Vitamin A toxicity. Liver Transpl 2006; 12: 1888.
Duignan E, et al: Ophthalmic manifestations of vitamin A and D deficiency in two autistic teenagers. Case reports in ophthalmology 2015; 24.
Galimberti F, Mesinkovska NA: Phrynoderma. J Am Acad Dermatol 2017; 76: AB197.
Grauel E, et al: Necrolytic acral erythema. J Drugs Dermatol 2012; 11: 1370.
Halawi A, et al: Bariatric surgery and its effects on the skin and skin diseases. Obes Surg 2013; 23: 408.
Jen M, et al: Syndromes associated with nutritional deficiency and excess. Clin Dermatol 2010; 28: 669.
Monshi B, et al: Phrynoderma and acquired acrodermatitis enteropathica in breastfeeding women after bariatric surgery. J Dtsch Dermatol Ges 2015; 13: 1147.
Ragunatha S, et al: A clinical study of 125 patients with phrynoderma. Indian J Dermatol 2011; 56: 389.
Raphael BA, et al: Low prevalence of necrolytic acral erythema in patients with chronic hepatitis C virus infection. J Am Acad Dermatol 2012; 67: 962.
Romano ME, et al: Dermatologic findings in the evaluation of adolescents with suspected eating disorders. Adolesc Med State Art Rev 2011; 22: 11.
Shmaya Y, et al: Nutritional deficiencies and overweight prevalence among children with autism spectrum disorder. Res Dev Disabil 2015; 38: 1.
Tiang S, et al: Nyctalopia. BMJ Case Reports 2010 Aug 26; 2010.
Vitamin D
Although active vitamin D is produced in the skin, deficiency of vitamin D has no primary skin manifestations, except for alopecia. Low vitamin D levels correspond in some children with atopic dermatitis (AD) severity, but studies are conflicting. Some studies have found genetic polymorphisms associated with vitamin D not to be more prevalent in atopic patients, but more recently patients with polymorphisms in the CYp24a1 vitamin D–inactivating enzyme were found to have more severe AD. Some patients with AD may improve and manifest fewer infections with vitamin D supplementation. Elderly persons have decreased vitamin D cutaneous photosynthesis because of decreased sun exposure and poor intake of vitamin D, both of which predispose them to osteomalacia. Aggressive photoprotection may also reduce vitamin D levels. Patients with cutaneous lupus and other photosensitive diseases who are counseled to avoid the sun and use high sun protection factor (SPF) sunscreens are at particular risk. Other patients at risk include those who are debilitated with limited sun exposure; those taking anticonvulsants; those with fat malabsorption; and patients with human immunodeficiency virus (HIV) infection, especially dark-skinned patients living in northern climes. Vitamin D 3 supplementation of 600 IU/day should be recommended in all these groups of patients for those up to age 70, and 800 IU for older patients; pediatric dosing is lower and based on age. Dermatologists who have patients at risk should also consider measuring vitamin 25 OH vitamin D levels.
Camargo CA Jr, et al: Randomized trial of vitamin D supplementation for winter-related atopic dermatitis in children. J Allergy Clin Immunol 2014; 134: 831.
Hallau J, et al: A promoter polymorphism of the vitamin D metabolism gene CYP24A1 is associated with severe atopic dermatitis in adults. Acta Derm Venereol 2016; 96: 169.
Malloy PJ, et al: The role of vitamin D receptor mutations in the development of alopecia. Mol Cell Endocrinol 2011; 347: 90.
Manousaki D, et al: Vitamin D levels and susceptibility to asthma, elevated immunoglobulin E levels, and atopic dermatitis. PLoS Med 2017; 14: e1002294.
Pinzone MR, et al: Vitamin D deficiency in HIV infection. Eur Rev Med Pharmacol Sci 2013; 17: 1218.
Vanchinathan V, et al: A dermatologist’s perspective on vitamin D. Mayo Clin Proc 2012; 87: 372.
Wang SS, et al: Vitamin D deficiency is associated with diagnosis and severity of childhood atopic dermatitis. Pediatr Allergy Immunol 2014; 24: 30.
Vitamin K Deficiency
Dietary deficiency of vitamin K, a fat-soluble vitamin, usually does not occur in adults because it is synthesized by bacteria in the large intestine. However, deficiency may occur in adults because of malabsorption caused by biliary disease, malabsorption syndromes, cystic fibrosis, or anorexia nervosa. Drugs such as coumarin, salicylates, cholestyramine, and antibiotics such as trimethoprim-sulfamethoxazole and the cephalosporins may induce a deficiency state. Newborns of mothers taking coumarin or phenytoin and premature infants with an uncolonized intestine can be vitamin K deficient. Standard practice is to administer intramuscular (IM) vitamin K at birth; however, some parents decline this, and those children are at 81 times greater risk of developing vitamin K bleeding than those who do receive it. Additionally, a rare condition exists that predisposes to bleeding, called hereditary combined deficiency of the vitamin K–dependent clotting factors. The liver synthesizes vitamin K–dependent clotting factors II, VII, IX, and X, and requires vitamin K as a cofactor. The result of vitamin K deficiency or severe liver disease is a decrease in the vitamin K–dependent clotting factors. The resulting cutaneous manifestations are purpura, hemorrhage, and ecchymosis and are similar to those seen with coumarin skin necrosis given the shared pathophysiology. Treatment is IM vitamin K for several days. In acute crises, fresh frozen plasma is used because it contains the clotting factors.
Burke CW: Vitamin K deficiency bleeding. J Pediatr Health Care 2013; 27: 215.
Centers for Disease Control and Prevention (CDC): Notes from the field: late vitamin K deficiency bleeding in infants whose parents declined vitamin K prophylaxis—Tennessee, 2013. MMWR Morb Mortal Wkly Rep 2013; 62: 901.
Fotouhie A, et al: Gastrointestinal bleeding secondary to trimethoprim-sulfamethoxazole-induced vitamin K deficiency. BMJ Case Rep 2016 Jun 6; 2016.
Lapecorella M, et al: Effective hemostasis during minor surgery in a case of hereditary combined deficiency of vitamin K–dependent clotting factors. Clin Appl Thromb Hemost 2010; 16: 221.
Napolitano M, et al: Hereditary combined deficiency of the vitamin K–dependent clotting factors. Orphanet J Rare Dis 2010; 5: 21.
Tie JK, et al: Characterization of vitamin K–dependent carboxylase mutations that cause bleeding and nonbleeding disorders. Blood 2016; 127: 1847.
Vitamin B 1 Deficiency
Vitamin B 1 (thiamine) deficiency results in beriberi. The skin manifestations are limited to edema and red, burning tongue. Peripheral neuropathy is common, and congestive heart failure may develop. In addition to alcoholism and lack of dietary intake, deficiency in vitamin B 1 can occur from bariatric surgery and in intensive care settings without proper nutrition.
Lee LW, et al: Skin manifestations of nutritional deficiency disease in children. Int J Dermatol 2012; 51: 1407.
Leite HP, de Lima LFP: Thiamine (vitamin B 1 ) deficiency in intensive care: physiology, risk factors, diagnosis, and treatment. In R Rajendram, VR Preedy, VB Patel (Eds.), Diet and Nutrition in Critical Care (pp 959-972). New York: 2015, Springer.
Tack J, Deloose E: Complications of bariatric surgery. Best Pract Res Clin Gastroenterol 2014; 28: 741.
Vitamin B 2 Deficiency
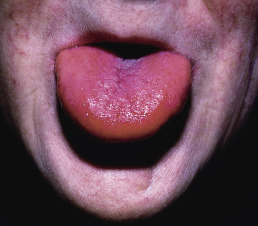
Vitamin B 2 (riboflavin) deficiency is seen most often in alcoholic patients; however, phototherapy for neonatal icterus, acute boric acid ingestion, hypothyroidism, and chlorpromazine therapy have also been reported as causes. The classic findings are the oral-ocular-genital syndrome. The lips are prominently affected with angular cheilitis (perlèche) and cheilosis. The tongue is atrophic and magenta in color ( Fig. 22.2 ). A seborrheic-like dermatitis with follicular keratosis around the nares primarily affects the face. Genital dermatitis is worse in men than in women who have riboflavin deficiency. There is a confluent dermatitis of the scrotum, sparing the midline, with extension onto the thighs. In its mildest form, the dermatitis is slightly “irritating” and pruritic, especially when sweating. As the deficiency progresses, the scrotum goes through a mild, acute dry phase with erythema and slight scale to a severe, chronic dry phase with confluent red papules that spread to involve the perianal area and inner thighs, accompanied by fissuring and pain. Balanitis and phimosis may occur, requiring circumcision. In severe deficiency, the entire scrotum becomes wet, with increasing pain and fissuring. The final stage is accompanied by massive swelling, and the scrotum may reach the size of a football. Photophobia and blepharitis angularis occur. The response to repletion is dramatic.
Roe DA: Riboflavin deficiency. Semin Dermatol 1991; 10: 293.
Tolkachjov SN, Bruce AJ: Oral manifestations of nutritional disorders. Clin Dermatol 2017; 35: 441.
Vitamin B 6
Pyridoxine Deficiency
Pyridoxine (vitamin B 6 ) deficiency may occur in patients with uremia and cirrhosis, as well as with the use of certain pharmacologic agents. Skin changes include a seborrheic dermatitis–like eruption, atrophic glossitis with ulceration, angular cheilitis, conjunctivitis, and intertrigo. Occasionally, a pellagra-like eruption may occur. Neurologic symptoms include somnolence, confusion, and neuropathy. Pyrodoxine has been used to prevent or treat chemotherapy-induced hand-foot syndrome but has not been consistently successful.
Pyridoxine Excess
A patient who ingested large doses of pyridoxine developed a subepidermal vesicular dermatosis and sensory peripheral neuropathy. The bullous dermatosis resembled epidermolysis bullosa acquisita. Exacerbation of rosacea was also reported in a patient taking isoniazide and pyridoxine.
Friedman MA, et al: Subepidermal vesicular dermatosis and sensory peripheral neuropathy caused by pyridoxine abuse. J Am Acad Dermatol 1986; 14: 915.
Macedo LT, et al: Prevention strategies for chemotherapy-induced hand-foot syndrome. Support Care Cancer 2014; 22: 1585.
Rezaković S, et al: Pyridoxine induced rosacea-like dermatitis. Acta Clin Croat 2015; 54: 99.
Vitamin B 12 Deficiency
Vitamin B 12 (cyanocobalamin) is absorbed through the distal ileum after binding to gastric intrinsic factor in an acid pH. Deficiency is caused mainly by gastrointestinal (GI) abnormalities, such as a deficiency of intrinsic factor, achlorhydria (including that induced by medications), ileal diseases, and malabsorption syndromes resulting from pancreatic disease or sprue. Aggressive treatment for the eradication of Helicobacter pylori may cause B 12 deficiency, as can metformin administration and long-term antacid ingestion. In food-cobalamin malabsorption syndrome, the body is unable to release vitamin B 12 from food or intestinal transport proteins, especially with accompanying achlorhydria. These patients have adequate dietary vitamin B 12 but often have atrophic gastritis. A Schilling test will be normal. Congenital lack of transcobalamin II can also produce B 12 deficiency. Because of the large body stores of B 12 in adults, deficiency occurs 3–6 years after GI abnormalities.
Glossitis, hyperpigmentation, and canities are the main dermatologic manifestations of vitamin B 12 deficiency. The tongue is bright red, sore, and atrophic. Linear atrophic lesions may be an early sign. The hyperpigmentation is generalized, but more often it is accentuated in exposed areas, such as the face and hands, and in the palmar creases and flexures, resembling Addison disease. The nails may be pigmented. Premature gray hair may occur paradoxically. Megaloblastic anemia is often present. Weakness, paresthesias, numbness, ataxia, and other neurologic findings occur. Repletion of vitamin B 12 can aid in chronic aphthous stomatitis in some patients.
Parenteral replacement with IM injections of B 12 , 1, leads to a reversal of the pigmentary changes in the skin, nails, mucous membranes, and hair. Megadose oral replacement of 1–2 mg/day may replace body stores by simple diffusion, independent of intrinsic factor. Neurologic defects may or may not improve with vitamin B 12 replacement.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


