The lower eyelids and midface are considered to be a contiguous aesthetic unit although they are different anatomic structures. Through in-depth understanding of complex anatomy and aging theory and appropriate surgical strategies according to the type of aging, surgical outcome of aging lower eyelid/midface can be more and more predictable. This article discusses the characteristics and theories of aging and 5 types of lower eyelid/middle face aging based on 4 key factors, namely, protruding fat in the orbital, excess skin on the lower eyelid, sagging midface and soft tissue deflation. Various combinations of surgical strategies are adopted accordingly.
Key points
- •
Knowing the anatomic structure of ligament, spaces, and superficial/deep fat compartment in lower eyelid/midface helps to ensure good outcomes.
- •
The theories of aging process and theirrelation to anatomic structure must be understood.
- •
Selection of surgical strategies is made according to the degree of the 4 aging factors: baggy lower eyelid, redundant of lower eyelid skin, fat deflation and malar descent.
- •
We provide a detailed description of the surgical method and effect of orbicularis oculi muscle and suborbicularis oculi fat lift in midface rejuvenation.
Introduction
The lower eyelid and midface are a central component of face. The degree of aging in these areas determines most of the “old” look of the patient. However, solving only lower baggy eyelid is no longer considered enough to achieve a “younger looking” visage and even results in a “tired looking” face if the patient has aging signs simultaneously coming from the midface or the lid–cheek junction, such as a tear trough deformity, nasojugal fold, malar fat ptosis, or midcheek groove. Although the lower eyelid and the midface are different anatomic structure, nowadays the current concepts consider they are aesthetic contiguous units, which should be managed simultaneously for optimal rejuvenation results .
Facial anatomy of ligamentous structure, space, and fat compartment
The midcheek is defined from the upper limits of the lateral canthus level to the lower limits of the oral commissure level. It can be divided into a bony support part, on which soft tissue is supported by maxilla and zygoma (midface), and an unsupported part, which is include the orbital cavity (lower eyelid) and oral cavity (upper lip). Although the anatomy of these areas is complex, recent cadaver studies and advanced tools have defined the anatomic structure of the middle cheek clearly, especially the ligamentous structures, spaces, and superficial/deep fat compartments. An understanding of the aging-related anatomic structure allows surgeons to adopt corresponding surgical strategies and also make the surgical outcome more predictable.
Ligament Structure
The ligamentous structure supports the soft tissues on top of the underlying bones or muscles. The relaxation of the ligamentous structure causes these soft tissues to hang on the loosening ligament line. Furthermore, resorption of the bone to which the ligament is attached or soft tissue deflation or descent results in grooves or depressions in the related ligamentous structure, such as a tear trough deformity or groove (tear trough ligament), palpebral–malar deformity (orbital retaining ligament), midcheek deformity or groove (zygomaticocutaneous ligament), or nasolabial deformity (maxillary ligament). The ligamentous structure can divide the midcheek into the lid–cheek, malar, and nasolabial zones.
Spaces
There are several spaces in the midcheek between the retaining ligament structures that provide gliding planes for movement of superficial over deep structures. Usually, no important structures pass within these spaces, which can be opened by blunt dissection easily in this avascular space. Three key spaces are identified and related for dissection in midface lift: the preseptal, prezygomatic, and premaxillary spaces.
Preseptal space
This inferior boundary of this space is palpebral origin of the orbicularis oculi muscle (OOM) medially and the orbicularis retaining ligament (ORL) laterally. The lateral boundary is the lateral orbital thickening. The floor and roof of the space is formed by the orbital septum and preseptal and pretarsal OOM, respectively. Hence, the space is located in the lower eyelid predominately. The space provides an ideal dissection plane for lower eyelid surgery.
Prezygomatic space
The triangular prezygomatic space is bounded superiorly by the ORL, inferiorly by the zygomatic ligament, and posteriorly by the preperiosteal fat; the origins of zygomaticus major and minor and anteriorly by orbital part of OOM and suborbicularis oculi fat (SOOF). Around midpupil line, the upper ORL boundary merges with its lower boundary into the vertex of the triangular space. This space helps the surgeon to approach the malar area and to identify the SOOF structure for a midface lifting procedure.
Premaxillary space
The premaxillary space is bounded superiorly by the tear trough ligament and the origin of the orbital part of OOM; inferiorly by maxillary ligament; medially by the nasal side wall, levator labii superioris alaeque nasi, and nasalis; and laterally by a 5-mm-wide loose areolar tissue. The floor is the levator labii superioris and the roof is the orbital part of the OOM. The release of the tear trough ligament and the origin of the palpebral and orbital OOM is considered to be adequate when the dissection is going into the premaxillary space and the levator labii superioris can be seen.
Fat Compartment
The face can be layers of the following structures: skin, superficial subcutaneous fat, superficial musculoaponeurotic system, deep fat, and deep fascia or periosteum. The superficial subcutaneous fat and deep fat of the midcheek are highly compartmentalized. Rohrich and Pessa performed a facial anatomic study by injecting methylene blue into facial soft tissue and tracked its diffusion by natural septa boundaries to further identify the different facial compartments. The midcheek superficial fat can be divided into orbital fat compartment, cheek fat compartment, and nasolabial fat (NLF) compartment. The inferior orbital fat of the orbital fat compartment is located in the lower eyelid with the lower boundary being the ORL. The NLF lies anteriorly to the deep medial cheek fat and medially to the SOOF; the superior border is the ORL. The superficial cheek fat compartment comprises the medial cheek fat, middle cheek fat, and lateral temporal cheek fat. The superficial medial cheek fat lies lateral to the NLF and the upper border is the ORL and the lateral orbital compartment. The inferior orbital fat, NLF, and superficial medial cheek fat are often referred to as malar fat. The deep fat, which lies below the superficial musculoaponeurotic system, is either anterior or posterior to the mimetic muscle. The deep fat includes the SOOF, which lies deep to the subcorbicularis oculi muscle with medial and lateral components and the deep medial cheek fat, which is located deep to the upper lip levators with a medial and a lateral part. The medial deep medial cheek fat lies deep and medial to NLF and the lateral deep medial cheek fat lies deep to the superficial medial cheek fat. The deflation and hypertrophy of different fat compartments with age causes the aged appearance in midface. ,
Aging appearance of lower eyelid and midface
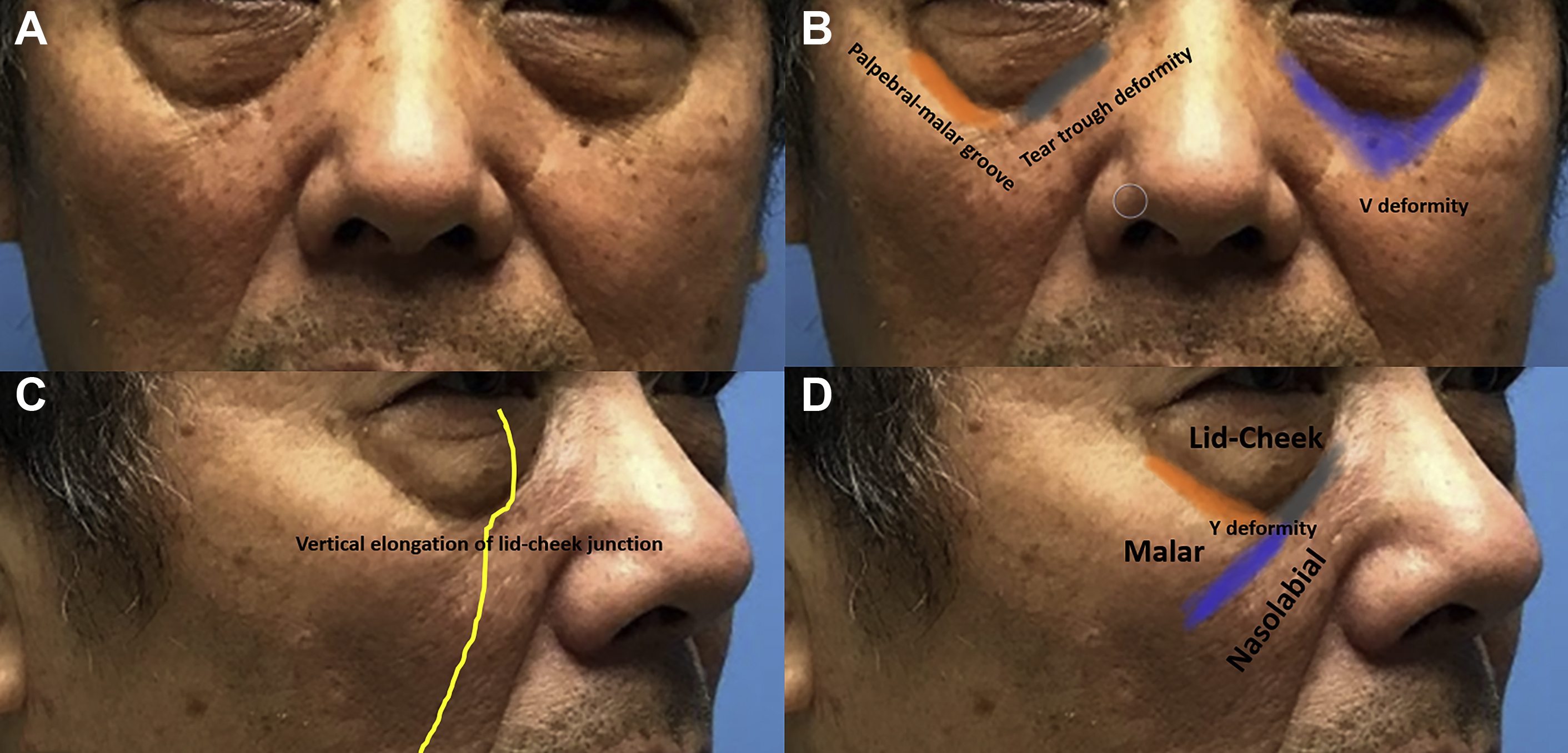
An aging lower eyelid/midface has characteristics of (1) wrinkles and redundant skin of lower eyelids ( Fig 1 A), (2) baggy lower eyelids (see Fig 1 A), (3) vertical elongation of lid–cheek junction (see Fig 1 C); (4) tear trough deformity/nasojugal fold (see Fig 1 B); (5) a palpebral–malar groove (see Fig 1 B); (6) a visible inferior orbital rim (see Fig 1 A); (7) a V deformity or depression (see Fig 1 B); (8) a midcheek groove with a Y deformity (see Fig 1 D); (9) a midface descend; and (10) a prominent nasolabial fold (see Fig 1 ).
Baggy Lower Eyelids
Protrusion of the orbital fat is caused by distension of the globe suspension system (capsulopalpebral fascia [CPF], Lockwood’s suspensory ligament, lateral canthus tendon, and orbital septum), which results in the globe descend. The lowering globe further compresses the intraorbital fat with subsequent forward displacement.
Tear Trough Deformity
The investigators found that a tear trough deformity is due to a lack of fat under the level of inferior arcus marginalis and the true osseocutaneous tear trough ligament between the palpebral and the orbital OOM. The tear trough ligament is derived from maxillary bone and inserts into dermis through the intersection between the palpebral and the orbital OOM. The triangular gap formed by the junction of OOM, medial lip elevators, and levator alaeque nasi also contributes to tear trough formation. The tear trough deformity may be congenital or be enhanced by aging process of maxillary bone resorption or the deep medial cheek fat deflation or malar fat decent.
Palpebral Malar Groove
The origin of OOM is attached firmly medial to the inferior orbital rim to the level of the medial corneoscleral limbus. However, when it goes further laterally, the muscle is only attached to the rim indirectly by orbital retaining ligament. The orbital retaining ligament is a bilamellar structure with a distance of 5 to 7 mm between the upper and the lower lamella. The distance narrows medially, lengthens centrally, and narrows again laterally until the ORL merges with the lateral orbital thickening. With the aging process, the tear trough deformity extends laterally along the laxity of the ORL and results in a palpebral malar groove. The deflation of inferior orbital fat and deep lateral cheek fat or descend malar fat causes the central V deformity with a hollowing of the central area under the deepening lid–cheek junction (tear trough and palpebral malar groove). The Y deformity is formed if the V deformity connects from the tear trough depression medially to the midcheek groove laterally. The Y deformity can separate the midcheek into the lid–cheek, malar, and nasolabial zones.
Aging theory of the midcheek
Before lower eyelid and midface surgery, surgeons should know the theory of aging. Five theories were postulated, including skin aging, ligament loosening, skeletal atrophy, gravitational soft tissue descent, and soft tissue volume loss.
Skin Aging
The process of aging skin is via both intrinsic and extrinsic factors. , The characteristics of intrinsic skin aging are the flattening between the interface of epidermis and dermis, the thinning of dermis and subcutaneous tissue, the loss of elasticity of skin owing to disorganization and reduction of elastic fiber, and the decreased number of fibroblast and its production of collagen types 1 and III. , The majority of external factors are owing to photoaging and tobacco consumption. Both factors can be independent or have a synergic negative effect on skin and causing premature wrinkles by production of intracellular reactive oxidative intermediates resulting in impairing the collagen synthesis, the production of abnormal elastin and proteoglycan, and thinning of the epidermis. Furthermore, the repetitive dynamic expressive muscle contractions such as OOM cause fine and deep wrinkles around the periorbital region. Combining this pathophysiology, aging skin shows fine wrinkles or deep depressed rhytids with laxity and redundance of the skin. Because the skin of the lower eyelid is thinner than that of the midface, the appearance of aging lower eyelid skin is more obvious than aging midface skin.
Skeletal Aging
Several authors observe that the facial skeleton continues remodeling through life by comparing young and old facial bone morphology with 3-dimensional computed tomography scans. The outcome shows the posterior displacement of the maxillary, resorption of the superomedial and inferolateral orbital rim, and the pyriform aperture. The resorption of this midfacial skeleton further pulls back the retaining ligament and results in greater depression or hollowing at the ligament area, such as the tear trough–nasojugal groove and its lateral extension palpebromalar groove by the tear trough–ORL or midcheek groove by the zygomaticocutaneous ligament. Furthermore, the midface soft tissue migrates inferiorly owing to the loss of support by the retruded maxillary. This process further enhances the aging appearance of nasal labial fold and V and Y deformities.
Ligament Loosening
The retaining ligament is considered to function as binding the soft tissue from the dermis to the underlining skeletal periosteum or the deep fascia of the parotid gland and masseter muscle. Mendelson and colleagues have described clearly the ligament structures (tear–trough–ORL, zygomaticocutaneous ligament) and spaces (preseptal, prezygoma, premaxillary) in between the structure and underlines 3 segments (lid–cheek, malar, and nasolabial) in the midface. , In youth, the ligament is firm, the space is tight, and it is able to hold and stabilize the soft tissue. However, the repeated facial expression and dynamic movement of the soft tissue in the midface with the intrinsic aging process loosens the ligament structure and makes the space expand. The weakness of the ligament structure and expansion space leads to soft tissue descent in the boundaries of these spaces. They also address that totally releasing the tear–trough–orbital retaining ligament is the key point to lift the ptotic midface structure.
Gravitational Soft Tissue Descent
The concept of the midface lift surgery is based on the soft tissue descent owing to gravity at the midface region. In youth, the malar fat stabilizing the upper midface part can cover the inferior orbital rim and blend the lid–cheek junction. Owing to ligamentous attenuation and gravity effect, the malar fat loses support and descends inferiorly. This inferior migration leads to the unveiling of the inferior orbital rim and the obvious tear trough deformity, palpebral malar groove, a V-shaped deformity, and a Y deformity with the midcheek groove. The migrated malar fat, which is accumulated and hanging above the line of the muscular attachment of nasolabial fold, further deepen the aging appearance of nasolabial fold. However, the aging midface appearance can be reverted 10 to 15 years when the patient is in the supine position. When the patient is lying down for the surgery, you can find the bulging baggy eyelid is decreased; the tear trough, palpebral malar depression, midcheek groove, and prominent nasolabial fold are diminished owing to the descended malar fat that drifts back to the original position and makes the hollowing groove appear full again. This phenomenon further supports the gravitational theory of midface aging.
Soft Tissue Volume Loss
The volumetric theory of facial aging is described by Lambros 20 and the concepts are gradually accepted and popularized recently through research by Rohrich and Passa. The main concept is compartmentalization of the facial soft tissue. The aging of midface appearance results from the deflation or hypertrophy of different fat compartments. The fat tissue can generally be divided into superficial and deep compartments. The tear trough or nasojugal groove is resulted from the deflation of deep periorbital fat (medial SOOF) followed by the loss of smooth blend between the medial SOOF and the superior border of malar fat (the lid–cheek junction). The further deflation of deep medial cheek fat and deep medial cheek fat makes the ptosis of the superficial medial cheek fat and NLF and leads to elongation of the tear trough laterally, with a visible inferior orbital rim and V deformity of the central medial cheek hollowing and prominent of nasolabial fold. Hence, the volume augmentation over the deep compartment fat can greatly diminish the tear trough, V deformity, and nasolabial fold and create more fullness of the anterior cheek and smooth the lid–cheek junction. , These points further elucidate the importance of volumetric theory in midface aging. A trend of aging is found with the gradual deflation of the deep facial compartment and hypertrophy of some superficial compartments, especially the inferior part adjacent to the natural crease.
Algorithm for the management of the lower eyelid and midface
The management of midface rejuvenation depends on the severity of aging in skin laxity, prominence of baggy eyelids, midface descent, and/or midface volume deficiency. The most important thing is to achieve a balance between surgeon’s technique and the patient’s expectation. Hence, there is no single surgical technique that can solve all kinds of lower eyelid and midface problem. The surgeon should examine the patient carefully, discuss the procedure and expectations in detail with the patient, and provide various techniques, listing their advantages and disadvantages. This author’s choice of surgical technique is based the following 4 aging factors of the lower eyelid and midface, namely, lower baggy eyelids, Skin laxity or redundancy of the lower eyelid, superficial/deep fat compartment deflation, and midface decent.
Lower Baggy Eyelid
If the patient has the sign of bulging fat herniation over the lower eyelid, the appropriate surgical strategy is either fat transposition or fat excision with CPF/septum hernia repair, depending on the signs of aging. Usually, for lower eyelid bulging fat without a tear trough deformity, visible inferior orbital rim, or V deformity, fat excision with a CPF hernia repair procedure is suffiecient. , , However, if the tear trough deformity, V deformity/depression, or visible inferior orbital rim are noted, the bulging fat is transposed to cover and augment the depression area of these deformity. Be careful with patients who have psuedoherniation of the lower baggy eyelid, in which the fat is not herniated or excessive, and the appearance of psuedoherniation is due to the severe depression of tear trough deformity and V deformity and skeletonization of inferior orbital rim. In this situation, the fat cannot be excised or transposed to avoid a hollowed appearance of the lower eyelid postoperatively. Instead, CPF hernia repair to avoid herniation in the future with a midface lift and/or fat grafting over the depressed area to blend the lid–cheek junction results in better outcome. Transconjunctval or subciliary approach depends on the skin laxity of the lower eyelids. If the patient is young and the skin is tight, a transconjunctival is preferred. In contrast, if the patient is old and redundant skin of the lower eyelid is noted and a midface lift will be performed in the same time, a subciliary incision is preferred.
Skin Laxity or Redundant of Lower Eyelid
The thinnest skin is found over the lower eyelid; redundancy and laxity of skin at this region is more and more obvious as age advances. Hence, skin removal is inevitable for the recovery of the youthful lower eyelid. Although skin tightening by laser or chemical peeling can achieve a similar result, the effect is better in Caucasian than Asian patients. After laser resurfacing or peeling hyperpigmentation, which are commonly seen in Asian patients, dark circles and a sleepy appearance result. The skin removal should be both conservative to avoid postoperative ectropion and liberal enough to achieve the desired aesthetic outcome. There is no standard or scientific rule to judge how much skin should be removed to achieve the best aesthetic result and avoid complications. Fortunately, as surgeons perform more cases and gain more experience, they develop better judgment for the skin excision. In general, after midface lifting by medial and lateral SOOF anchoring to the inferior orbital and lateral orbital periosteum, respectively, the patient is instructed to open their eyes and mouth to their maximum degree, and the width of skin excision can be judged at this time. The cutting line of lower skin muscle flap is just above the upper margin of subciliary incision without forcefully pulling the lower skin–muscle flap upward. This is one reasonable method to judge skin removal. The other method is the pinch test, where the patient sits in front of surgeon and the surgeon uses the curved forceps to pinch the skin that needs to be removed from the incision line and see if it causes ectropion. The least width of pinched skin that does not cause ectropion is the skin you can remove.
Superficial and Deep Fat Compartment Deflation
Soft tissue volume loss and skeletal resorption over the midface lead to the pseudoptosis of malar fat. The inferior migration of malar fat owing to the loss of support by posterior displacement of the midface skeleton and deep medial cheek fat compartment deflation further elongate the tear trough depression from the medial to the lateral side of inferior orbital rim, which is named the palpebral malar groove. These structures make the inferior orbital rim skeletonized and visible, the V deformity or depression owing to central hollowing below the visible inferior orbital rim, and the Y deformity or depression if the depression along the zygomatico–cutaneous ligament is obvious. Hence, the strategy to solve the volume loss is fat graft augmentation over the deep portion of midface fat compartment to give the support of the superficial fat compartment and fullness of the cheek and further fat graft contouring in the superficial fat compartment to blend the lid–cheek junction, depression, and any irregular area.
Midface Decent
A midface lift can correct the malar fat descent resulting from a gravitational effect and ligamentous laxity. The reposition of malar fat can diminish the visible of inferior orbital rim and V-deformity/depression and make the upper anterior cheek more fullness. The dissection planes are reported either via subperiosteal or preperiorsteal plane through the prezygomatic and premaxillary spaces. The subperiosteal approach has been often used previously owing to its simplicity and the concept of whole composite flap lift including the skin, OOM, SOOF, and the zygomatic major and minor muscle and lip levators. , Fixation can be either on the deep temporal fascia via a transtemporal approach or on lateral orbital thickening and inferior orbital rim via a subciliary approach. However, prolonged swelling, ecchymosis, and other possible complications are noted with this approach. The intact tight periosteum cannot be lifted until the distal inferior periosteum is released. Hence, an intraoral incision is sometimes needed, which in turn carries the risk of infection. Furthermore, because the ligament structure from the periosteum to the dermis remains intact, the deformity owing to the tear trough ligament and ORL complex cannot be resolved completely. During the animation and speech process, before the periosteum is firmly attached to the new position, the contraction of the levator lip, zygomatic major and minor muscles cause the midface descent to recur readily. With a clear understanding of the anatomic structure of the midface, preperiosteal dissection is now safer and more effective for the midface lift. , , Preperiosteal dissection through the bloodless and predissected prezygomatic and premaxillary space can actually break the ligament connection from periosteum to dermis and separate the superficial component (skin, OOM, and SOOF) from the deep structure (lip levator muscle, zygomatic major and minor). Hence, the superficial components can easily slide upward on the deep structure. The superficial components will not be affected by contraction of the deep animated muscle. These advantages mean that it has less swelling and ecchymosis compared with subperiosteal dissection, and it can raise the malar fat more stably without being disturbed by deep muscle pulling.
Surgical Strategy According to the Four Aging Factors
Based on the 4 key aging factors, different surgical strategies can be adopted ( Table 1 ). If the patient only has volume loss-predominant aging (type I aging) with tear trough groove and/or midcheek groove and nasolabial fold. The volume augmentation by autologous fat grafting or fillers is sufficient to solve patient’s problem. In type II aging, some patients present with prominent and protruding baggy lower eyelids without skin aging, volume deflation, or malar descent. The bulging fat excision and/or CPF/septum hernia repair through transconjunctival approach is appropriate to correct the problem ( Fig 2 ). However, with progression of aging process, the protruded intraorbital fat with tear trough and mild central V deformity owing to volume loss will happen. In this type III aging, skin is not redundant and aging malar is not descended, the herniated fat can be transferred to augment the tear trough deformity and central V deformity ( Fig 3 ). Optional autologous fat grafting can be added to increase the fullness of anterior cheek if the herniated fat is not enough to fill the deformity. In type IV aging, the skin is redundant, the baggy lower eyelid is prominent, and the midface is drooping, but the volume deflation is not obvious. In this type of aging, a subciliary incision to excise the herniated fat with a CPF hernia repair procedure and SOOF lift is adequate to correct the deformity ( Fig 4 ). On occasion, the baggy lower eyelid is not obvious and intraorbital fat removal is not required. The CPF is repaired to the arcus marginalis to prevent the anticipated herniation in the future. In type V aging, the skin is redundant, the midface is descending, and deflation is moderate to severe; fat transposition to cover the visible inferior orbital rim is indicated for obvious baggy lower eyelids with a simultaneous SOOF lift and autologous structural fat grafting ( Fig 5 ). Alternatively, CPF repaired to the arcus marginalis is combined with a SOOF lift and autologous fat graft in type V aging, with not obviously herniated intraorbital fat. The choice of septum or CPF hernia repair depends on the strength of septum. If the septum is already degenerated into a thin, lax membranous structure, which is usually found in type IV or V aged patient, CPF hernia repair may be a good choice for preventing fat herniation in the future. If the septum structure is still strong and intact, septum hernia repair to arcus marginalis is first choice, usually in the type II or III (young) patient. However, the distinctions between the types are not always so straightforward. In addition, surgeon preference of surgical strategy differs. Surgeons should develop their own algorithm according to their experiences and adopt their familiar surgical strategies according to the aging types and the communications with patient.
Related posts:
 Forehead Lift for Asians
Forehead Lift for Asians
 Incisional Blepharoplasty for the Asian Eye
Incisional Blepharoplasty for the Asian Eye
 Special Considerations in Facial Reconstruction in the Non-White Patient
Special Considerations in Facial Reconstruction in the Non-White Patient
 Recent Trends in Orthognathic Surgery in Asia
Recent Trends in Orthognathic Surgery in Asia
 Special Consideration in Rhinoplasty for Deformed Nose of East Asians
Special Consideration in Rhinoplasty for Deformed Nose of East Asians
 Cosmetic Bone-Contouring Surgery for Asians
Cosmetic Bone-Contouring Surgery for Asians
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


