Asians have anatomic and clinical characteristics to be considered before forehead lift. Because of the anatomic characteristics of Asians, for the better outcomes of blepharoplasty or augmentation rhinoplasty, forehead lift as a combined surgery must be considered beforehand. Forehead lift is frequently indicated in young Asian patients. Endoscopic browlift without visible scar is favored for patients, and it can be done in a modified multiplane fashion for better outcomes in patients with thick and redundant skin. There are rare but severe complications of endoscopic forehead lift, such as motor nerve paresis and diplopia, although they are temporary in most cases.
Key points
- •
For Asians, there are special anatomic and clinical considerations in performing forehead lift.
- •
Forehead lift has powerful clinical effects when it is combined with augmentation rhinoplasty and blepharoplasty.
- •
For the best outcome of the forehead lift in Asians, the dissection planes, incisions, and skin resections can be diversified.
- •
There are rare complications related to the endoscopic forehead lift, such as temporal facial nerve injury and diplopia.
Introduction
The rejuvenation of the upper third of the face is the key to the restoration of the patient’s youthful appearance, because the aging changes are often most pronounced in the upper one-third of the face. The aging changes of the upper face include forehead rhytides, sagging eyebrows, hooding of the upper eyelids, and periorbital wrinkles. Continuous muscle contractions lead to horizontal rhytides by the frontalis muscle, vertical glabellar rhytides by the corrugator supercilii muscle, and crow’s-feet by the orbicularis oculi muscle. In addition to repeated muscle contraction, tissue sagging also contributes to the aging changes.
Besides gravitational pull, deflation of skin and subcutaneous tissue, gradual volume loss of bone and muscle in the frontal, temporal, and orbital regions are related to the tissue sagging. The eyebrows begin to descend with infrabrow tissue, which is sagging and bulging over the eyelids. Ptotic brows and combined dermatochalasis of eyelid skin leads to the hooding of the upper eyelids. Horizontal rhytides in the nasal root also develop with sagging soft tissue in the region accentuated by the action of the procerus muscle. Combined effects of these changes clinically result in the appearance of aging face with a sense of fatigue, anger, or sadness.
With the emergence of endoscopic facial surgery in the 1990s, endoscopic forehead lift has evolved to an alternative to the classic forehead lifts with decreased numbness, smaller invisible scars, and shorter recovery period. Now the endoscopic brow lift is regarded as a standard procedure with long-term favorable outcomes.
Despite its numerous advantages, the endoscopic browlift is often criticized for a high recurrence rate, ranging up to 9% in some studies, and still there is no consensus on which forehead lift technique is the most reliable and safe. Endoscopic browlift has some clear disadvantages in patients with thick furrowed skin, and high arched foreheads. In these patients, still there is a role for the classic coronal or subcutaneous forehead lifts and they can be done as solitary or combined procedures with endoscopic browlift.
Discussion
There are anatomic and clinical differences for Asians that should be considered carefully before the forehead lift operation. Asians tend to have thicker skin and ligamentous attachments in forehead. Relieving the heavy soft tissue load in glabella, subbrow, upper eyelids, and radix area by forehead lift has a great clinical significance when it is performed in combination with other facial plastic surgeries, such as rhinoplasty and blepharoplasty.
Special Considerations for Asians
Double-eyelid surgery
The double-eyelid surgery is the most common aesthetic procedure in East Asian countries. When evaluating a patient seeking the double-eyelid surgery, the upper eyelids should be evaluated in contiguity with the eyebrows and forehead.
Roughly 50% of East Asians have some form of supratarsal folds (ie, double-eyelid creases ) and others do not. Asians without double-eyelid creases have characteristics of puffy eyelids and heavy infrabrow soft tissue. Because of abundant orbital fat that is overlying the tarsal plate, insertion of the levator aponeurosis to the dermis is hindered.
Heavy infrabrow tissue is related to thick skin and bulky subcutaneous fibrofatty layer and orbicularis oculi muscle. The retro-orbicularis fat, preaponeurotic fat, and pretarsal fat contribute to the thick eyelid skin. For these patients, when the supratarsal fold is surgically created along the thick eyelid skin, an unnaturally deep fold under the overhanging plump eyelid skin is created giving the unnatural operated look.
In case of elderly patients who exhibit redundant eyelid skin with dermatochalasis and concurrent brow ptosis, browlift must be considered to relieve the skin excess before or in combination with blepharoplasty.
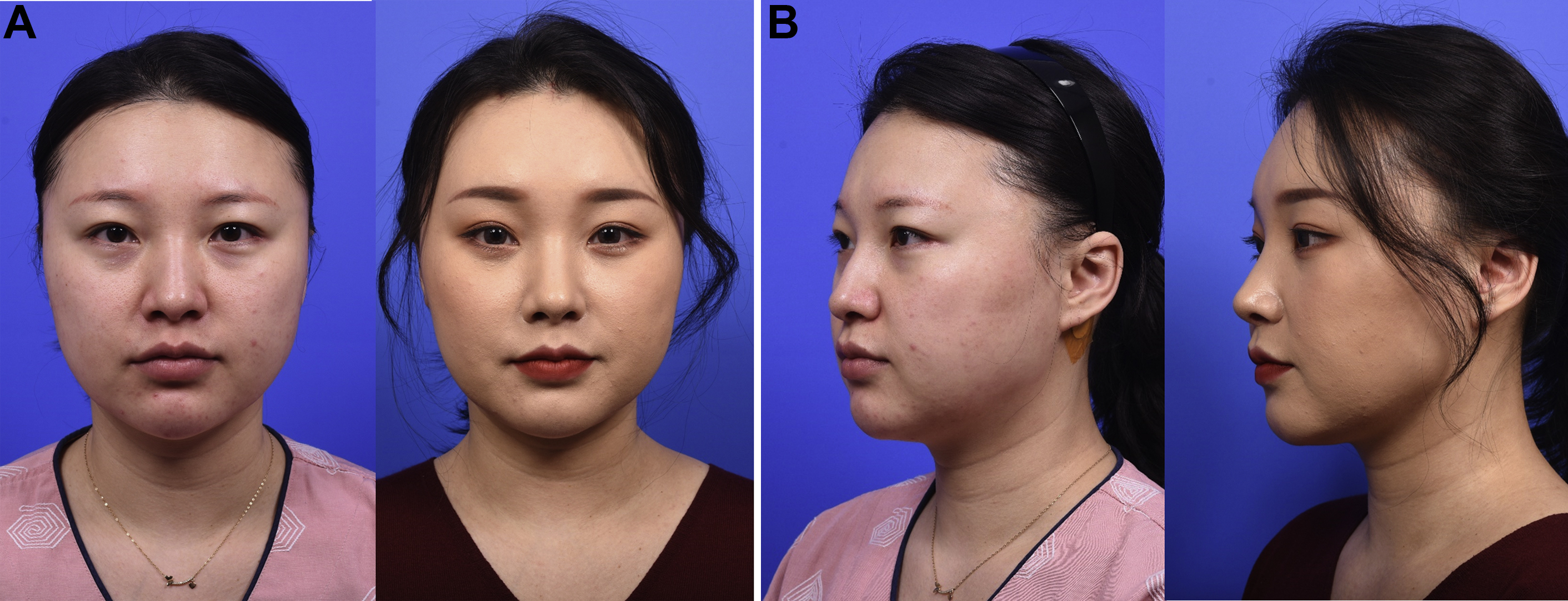
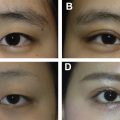
Likewise, for a more satisfying outcome of the double-eyelid surgery in younger patients with heavy eyelids, the heavy soft tissue load in the infrabrow-eyelid area must be relieved first by the browlift before or in combination with the double-eyelid surgery ( Fig. 1 ). In the same regard, for a patient who wants to increase the height of preexisting supratarsal creases, the surgeon must consider the browlift first if there is fullness of soft tissue over the upper eyelids.
Ideally, endoscopic browlift proceeds first, and at least a month and ideally 6 or more months later, double-eyelid surgery is performed. If double-eyelid surgery and the endoscopic browlift are done concurrently as combined surgeries, supratarsal creases are created first in a modestly lower position before the browlift. When the brow with infrabrow soft tissue is elevated and eyelid skin is stretched thin by the browlift, supratarsal creases on a thinned skin are more natural and shallower in shape.
Considering that the patients seeking the double-eyelid surgery are commonly young-aged, endoscopic browlift is the most suitable browlift procedure because of completely hidden scars.
Augmentation rhinoplasty
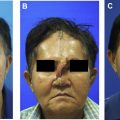
Augmentation rhinoplasty is one of the most popular aesthetic procedures in Asian countries. Although rhinoplasty and brow modification is a powerful combination, there has been little attempt to integrate analysis of the nose and brows, even though modification of the nasal-glabellar relationship maximizes the results for patients seeking rhinoplasty. Brow elevation with modifications of the glabellar muscles deepens the nasion, creates concavity, elongates the overall nasal length, and also makes the brow-tip aesthetic line narrower and more defined ( Fig. 2 ).

One of the most common mistakes by surgeons doing augmentation rhinoplasty for Asian patients is overaugmentation of the radix. Asians have flat foreheads, and the nasofrontal angle is shallow and it is rather a gentle smooth curvature than an angle, especially in females. This is the reason why forehead augmentation surgery with fat injections or alloplastic implants is common in Asian countries.
In elderly Asians, brow ptosis aggravates the ill-defined nasion with the flat nasofrontal angle and fullness of radix, where overaugmentation of radix results in an unnatural operated look that is aesthetically detrimental especially for female patients. Some younger Asian patients may also exhibit soft tissue crowding in the glabellar area, which is usually combined with heavy infrabrow soft tissue and puffy eyelids with variable degree of brow ptosis.
Browlift is remarkably beneficial in these patients as a combined surgery with augmentation rhinoplasty. Browlift relieves the fullness of the radix opening the nasofrontal angle and increases the glabella-to-nasion distance to make room for an amount of augmentation. Also the brow-tip aesthetic line is more enhanced with elevation of brows. The general length of the nose is elongated also, because browlift moves the nasal starting point higher by removing the bulging soft tissue in the nasal root, which sets the soft tissue nasion in a lower position.
As in the case of double-eyelid operation, endoscopic browlift is always preferred as a combined procedure with augmentation rhinoplasty for younger patients, because of hidden scars.
Browlift should be considered before augmentation rhinoplasty for the patient as follows:
- •
Patients with full radix, ill-defined nasion.
- •
Patients with flat forehead and low-set brows.
- •
Patients with flat nasofrontal angle, who nevertheless want significant amounts of radix augmentation.
- •
Secondary patients who complain that their nose still looks “heavy” following a primary rhinoplasty.
- •
Patients who have a history of foreign body injections in the glabella and nasal root.
Brow shape
Numerous attempts have been made to define the ideal shape and position of the eyebrows. However, although there are certain basic principles, the aesthetic ideal cannot be generalized and must be assessed in relation to sex, ethnicity, orbital shape, eye prominence, and overall facial proportions. Preferred eyebrow for any individual is influenced by culture, fashion, and the era in which one lives.
Culturally, Korean women in the present time may prefer flatter shape of the brows, compared with White women who prefer a more arched and laterally upward shape of the brows. This cultural difference is well witnessed in the brow make-up by Korean and Korean-American women. It is noticeable that the flatter and fuller brow shape is preferred by Korean women living in Korea and the more arched and slimmer brow shape preferred by Korean-American women raised in America.
Some Western surgeons try to keep the medial brow at a lower level while elevating the lateral brow, minimizing modifications of brow depressor muscles. However, for Korean women, moderate amount of medial brow elevation is well accepted and even desired by many. It is reported that the head-up type and the horizontal type of the brow were preferred for the young-looking brows by Korean women, , and this preference is more evident in young Korean women. Therefore, modification for brow depressor muscles should be sufficient enough to mobilize the medial brow in most Asian patients, if it is not contraindicated in such cases who have downturned or droopy eyebrows.
Thick skin and dense ligamentous attachments
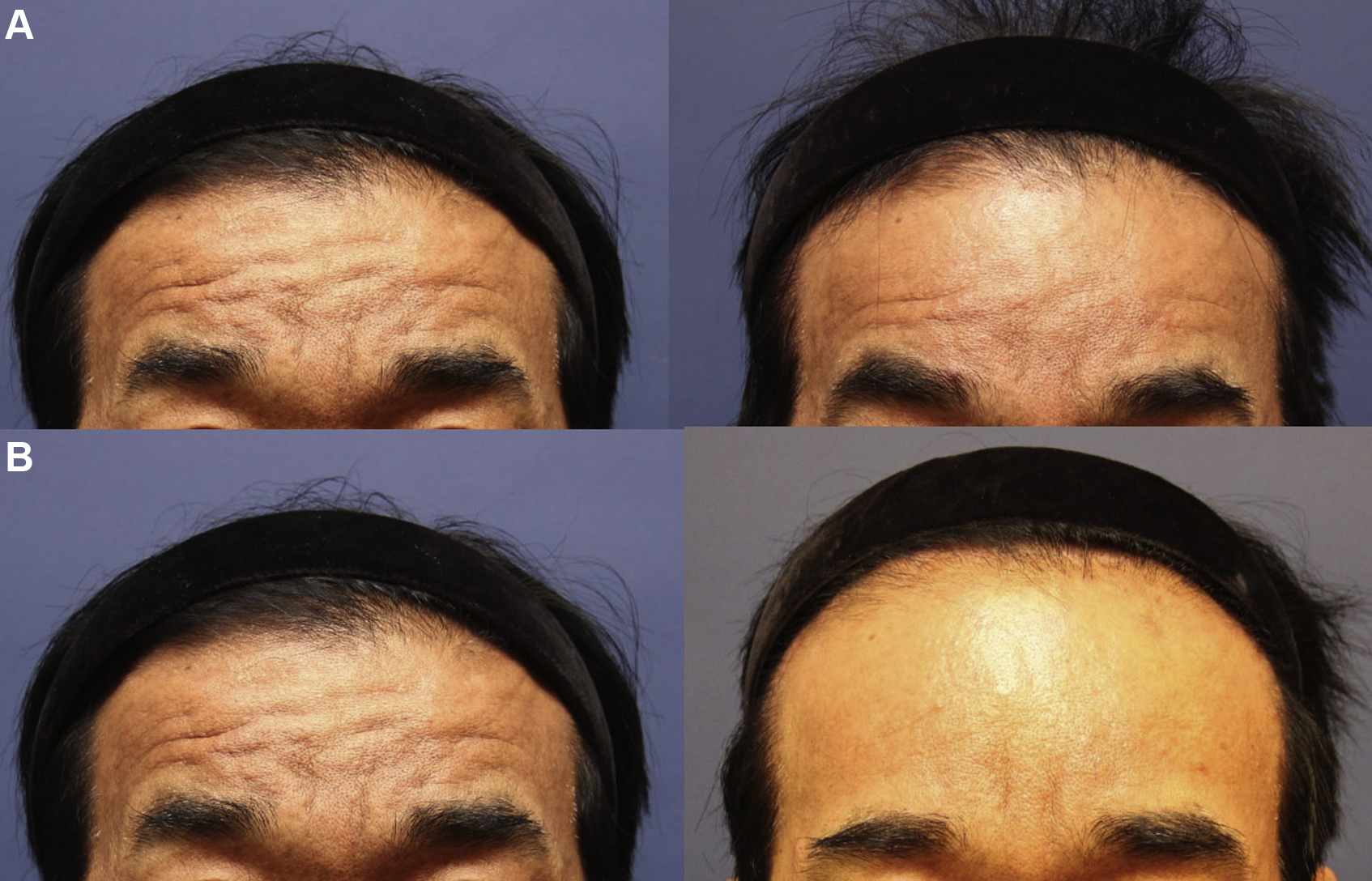
Asians generally have thicker skin than Whites. Asian male patients often have thicker forehead skin with deep transverse folds, and ligamentous attachments of the skin to the underlying bone are also dense and stout making surgical dissection more difficult. Heavy and firm forehead skin may predispose to incomplete correction or relapse of forehead rhytides with the standard endoscopic forehead lift, which may fall short in providing an adequate rejuvenation of the thick skin with deep folds.
Endoscopic browlift without skin excision does not address the problem of skin laxity or redundancy in the forehead effectively in patients who has the skin as a main problem ( Fig. 3 ).
Related posts:
 Incisional Blepharoplasty for the Asian Eye
Incisional Blepharoplasty for the Asian Eye
 Special Considerations in Facial Reconstruction in the Non-White Patient
Special Considerations in Facial Reconstruction in the Non-White Patient
 Nonincisional Blepharoplasty for Asians
Nonincisional Blepharoplasty for Asians
 Recent Trends in Orthognathic Surgery in Asia
Recent Trends in Orthognathic Surgery in Asia
 Special Consideration in Rhinoplasty for Deformed Nose of East Asians
Special Consideration in Rhinoplasty for Deformed Nose of East Asians
 Cosmetic Bone-Contouring Surgery for Asians
Cosmetic Bone-Contouring Surgery for Asians
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


