The major needs for cosmetic facial bone surgery come from anatomic differences in facial shape and in personal preference. Especially when consulting patients with different national or ethnic backgrounds, careful attention should be paid during consultation for the ideal or desirable facial shape that they have in mind. Patients generally seek a slim and smooth-contoured face. Surgery of the cosmetic facial bone has developed from surgical experiences in facial bone trauma and congenital anomalies. A limited approach is recommended for satisfactory aesthetic outcome. Surgeons should understand the basic procedures of L-shaped osteotomy of the zygoma and intraoral mandible reduction.
Key points
- •
Zygoma reduction decreases the width of cheekbones in order to achieve slim, smooth, and feminine facial aesthetic lines. The purpose of mandible reduction is to make the lower face appear slim, oval, and have a smooth contour.
- •
The 2 surgical methods in this article (L-shaped osteotomy of the zygoma and intraoral mandible reduction) are the most widely used and accepted surgical methods.
- •
The zygomatic body and arch are usually moved posteromedially during surgery; the point of maximal malar projection should be evaluated and transposed to a new ideal position.
- •
Mandible reduction does not simply mean angle reduction but making the overall frontal jaw line slim and natural.
Introduction
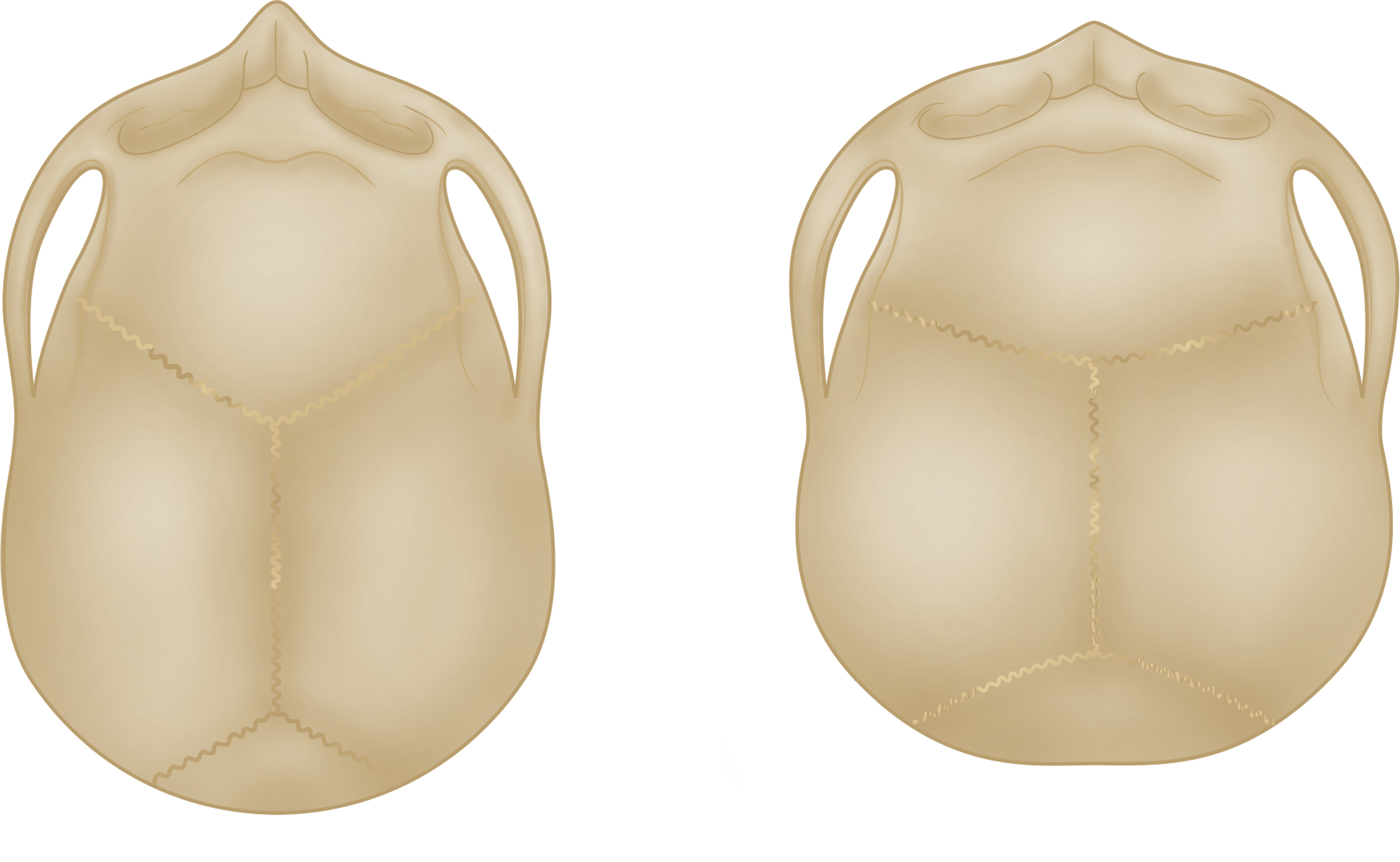
Many investigators have emphasized the difference between white people and Asians, and the facial bone is one of the major factors that create differences in those groups. For example, most caucasians are dolichocephalic, whereas most Asians are brachycephalic ( Fig. 1 ). Facial shape in the frontal view also differs. The faces of caucasians tend to be long and narrow, whereas the faces of Asians tend to be wide and short. Consequently, Asian faces usually give a square impression.
What Is the Ideal Face?
A study showed there is a huge difference between Asians and caucasians in terms of the ideal face. Regarding the vertical proportion of the face, Asians prefer a short chin compared with white people because it gives a more feminine and soft impression. Asians usually regard a broad face as unattractive and aesthetically unpleasing, especially in women, because it gives the face a masculine appearance. Prominent cheekbones are a trademark of strong personality, which is not desired in Asian regions. Recently, size of the face is the issue, and Asian people prefer a small face in proportion with the whole body. It is extremely important for surgeons to understand each patient’s end-image of the surgery as well as the motivation for considering facial bone surgery.
Facial bone surgery has evolved for more than 100 years but has only recently been applied to cosmetic fields. , It is still a minor portion of Western cosmetic surgery, whereas it may be more popular in Asians. Aesthetic facial bone surgery can be divided into the surgery of the middle face, lower face, and chin, but this article focuses more on the middle and lower face.
Patient assessment and consultation
Analysis of the individual’s entire face should come from a thorough understanding of facial skeletal types, and establishment of proper surgical indications for each technique is mandatory in order to achieve aesthetically pleasing results. Direct physical examination is most important when collaborating with the patient’s aesthetic concerns and establishing a surgical plan. A computed tomography (CT) scan with three-dimensional reconstruction is essential to evaluate the shape of the facial bone precisely to plan surgery.
Frontal Evaluation
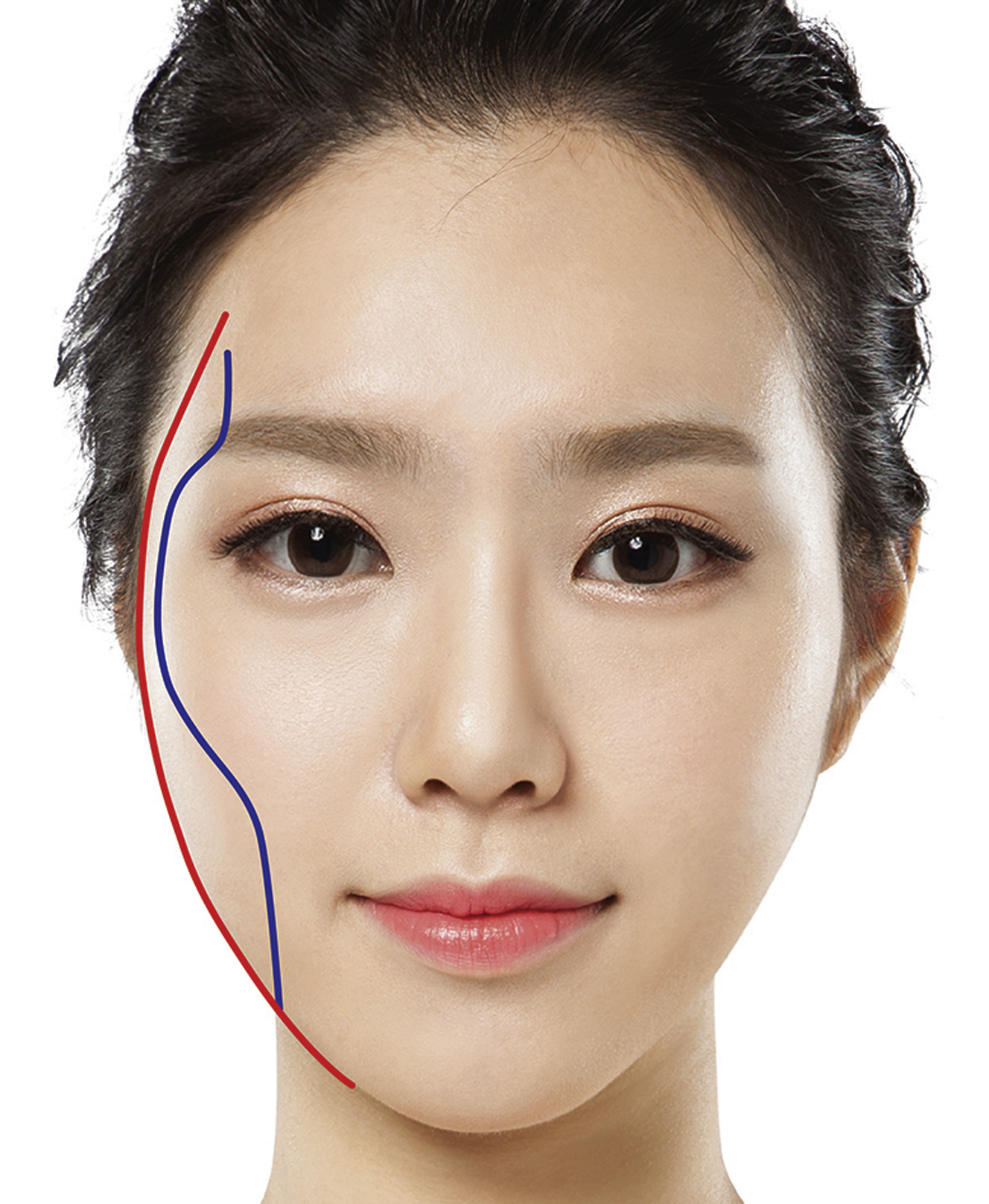
Frontal evaluation can be simplified by visualizing an anterior and posterior facial plane. The anterior facial plane is defined by the superior temporal line, lateral border of the lateral orbital rim, malar prominence, midface, and mentum ( Fig. 2 , blue line). The posterior facial plane is defined by the contour line of the head and zygomatic arch (see Fig. 2 , red line). A combination of variable forms of these 2 planes defines the variety of facial shapes encountered in clinical practice. Anterior and posterior facial lines that are wide and parallel to each other in the midface area lead to a wide facial appearance. Severity of zygoma protrusion is usually determined by bizygomatic distance. In patients in whom the cheek bones protrude outward, the facial line connecting the temple-zygoma-cheek-mandible angle becomes convoluted and gives a harsh look to the face (see Fig. 2 ). In patients in whom the mandible angle flares out, the facial shape forms a square and gives a masculine impression.
The length and shape of the chin should be examined. The chin plays a key role in overall facial impression ( Fig. 3 ).

Three-Quarter Oblique Evaluation
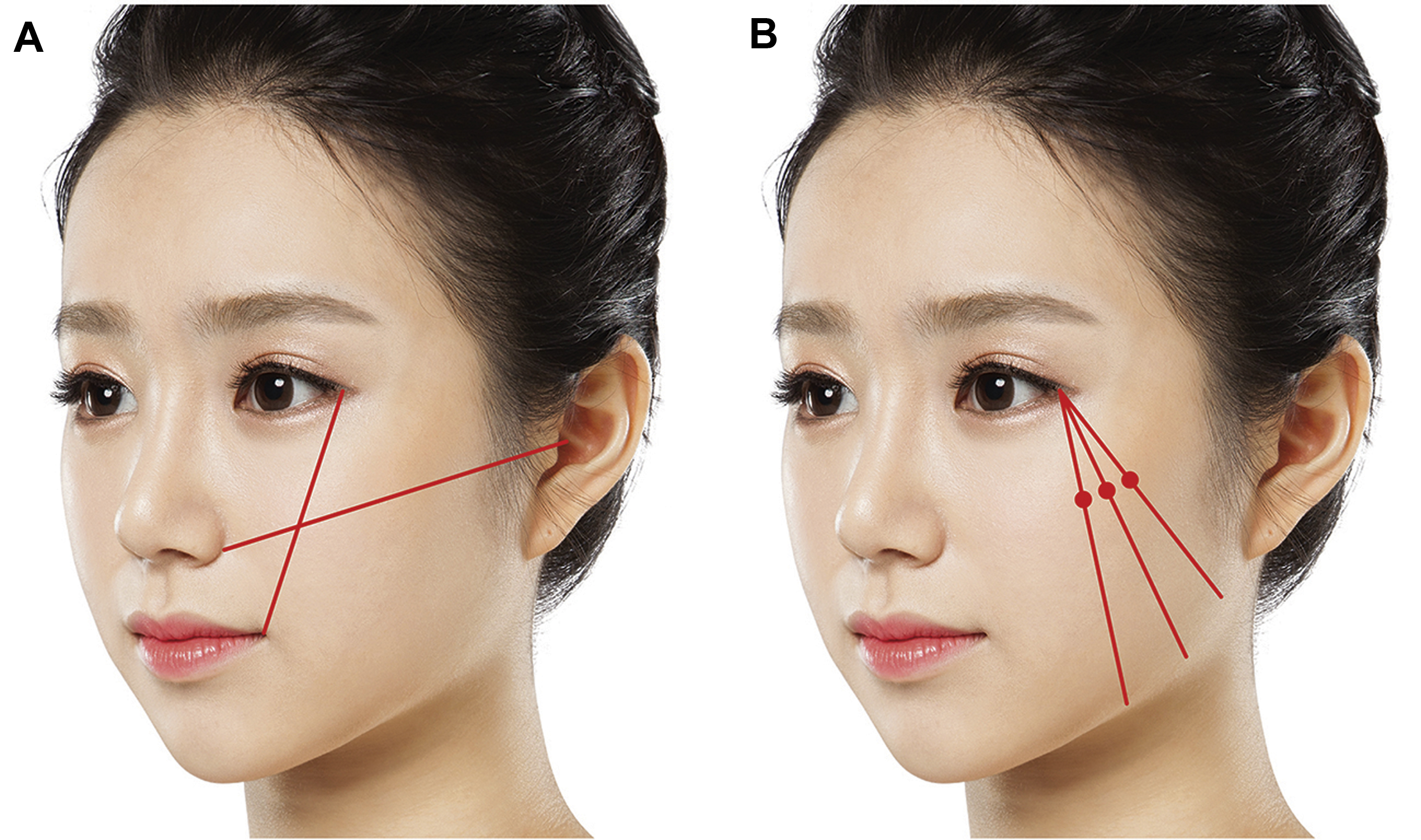
The zygomatic body is most clearly appreciated in the three-quarter oblique view, exposing the shape of zygoma as well as the degree and location of zygomatic body protrusion. Severity of zygomatic protrusion is usually determined with the point of maximal malar projection (MMP). The MMP is the most protruded portion of the outer contour of the zygomatic complex in the three-quarter views. Shape and position vary among patients, thus altering the projection, and position of the MMP point placed precisely in the patient’s aesthetically ideal position, is the key to a successful postoperative result.
The ideal MMP point may vary among different ethnicities and patients’ needs; however, patients who desire zygoma reduction want the MMP to be medial to the lateral canthus in the horizontal dimension, and not too high or too close to the lateral canthus in the vertical dimension , ( Fig. 4 ).
Lateral Evaluation
The gonial angle and the mandibular plane should be identified using the lateral cephalogram. If the gonial angle is less than 100°, the facial shape looks square. If the gonial angle is located too low or the mandibular plane is too flat (<30°), the lateral face also looks square ( Fig. 5 ).

Facial profile should be evaluated and understood in lateral evaluation. In class III profile, mandible surgery should be done cautiously in order to not exacerbate the prognathic look. In contrast, in class II profile patients, zygomatic reduction should be done cautiously to exacerbate a long face.
Basal Evaluation
When viewed from below, the degree of projection in the suborbital area and protruding zygomatic arch can be evaluated. This view helps in evaluating symmetry and facilitates evaluation of the zygomatic arch.
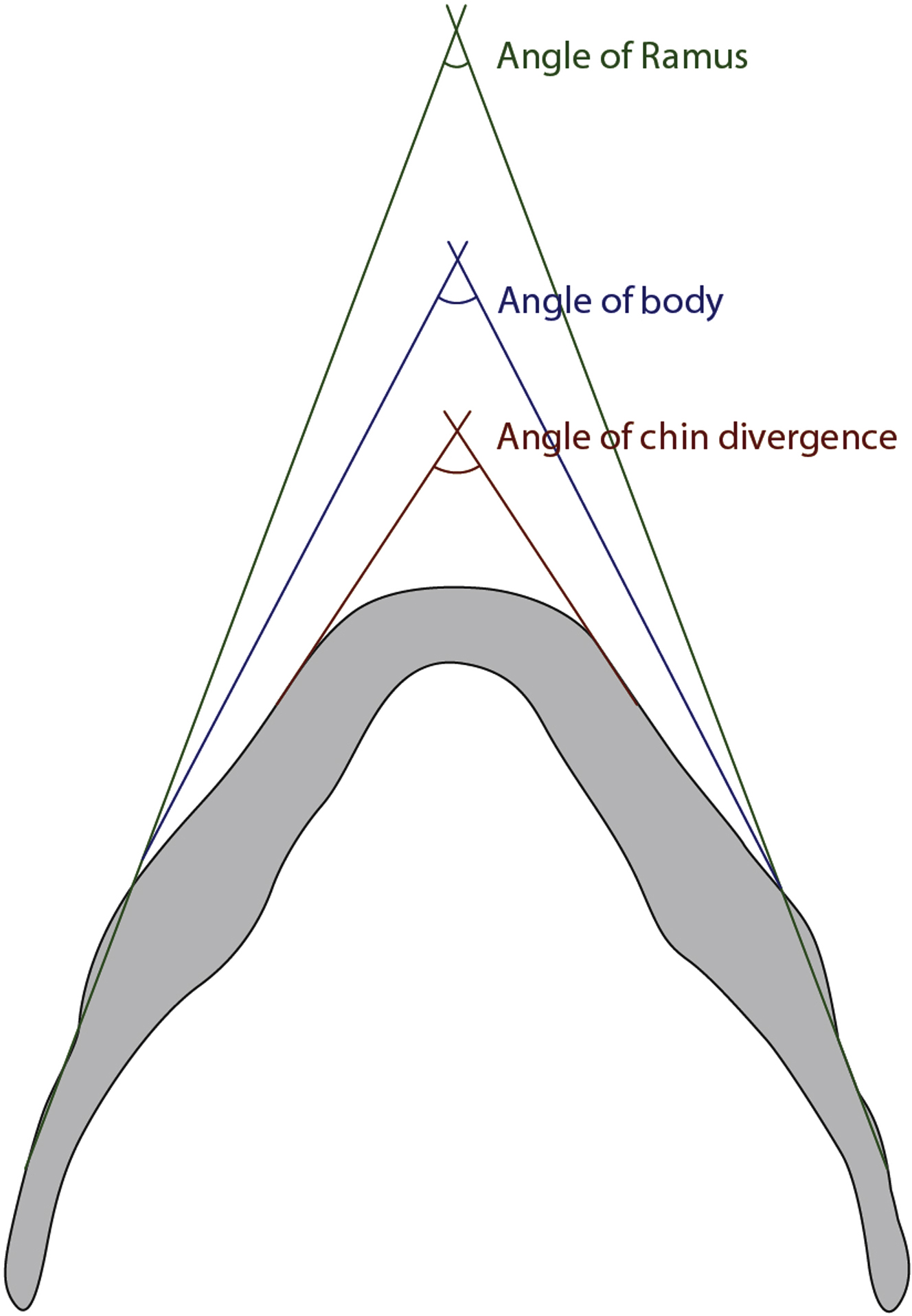
Transverse shape of the mandible can also be evaluated ( Fig. 6 ). The angle of divergence and convexity of the mandible are observed. In patients with an inward curled angle with convex transverse shape, sagittal resection at the body helps to reduce the width of the mandible more effectively.
Soft Tissue Evaluation
Because facial soft tissue is also an important component in zygoma reduction, it should be given due consideration to achieve a satisfactory aesthetic result. If the patient has thin skin with minimal soft cheek tissue, changes following zygoma reduction will be obvious with minimal prospect of soft tissue drooping. Such patients are ideal candidates for zygoma reduction.
In contrast, the risk of cheek drooping increases if the patient has abundant soft tissues or thick skin. Surgeons should discuss the possibility of cheek drooping with the patient during the informed consent process and contemplate appropriate additional procedures, such as liposuction or lifting, to counter this possibility.
Surgical techniques
Zygomatic Reduction
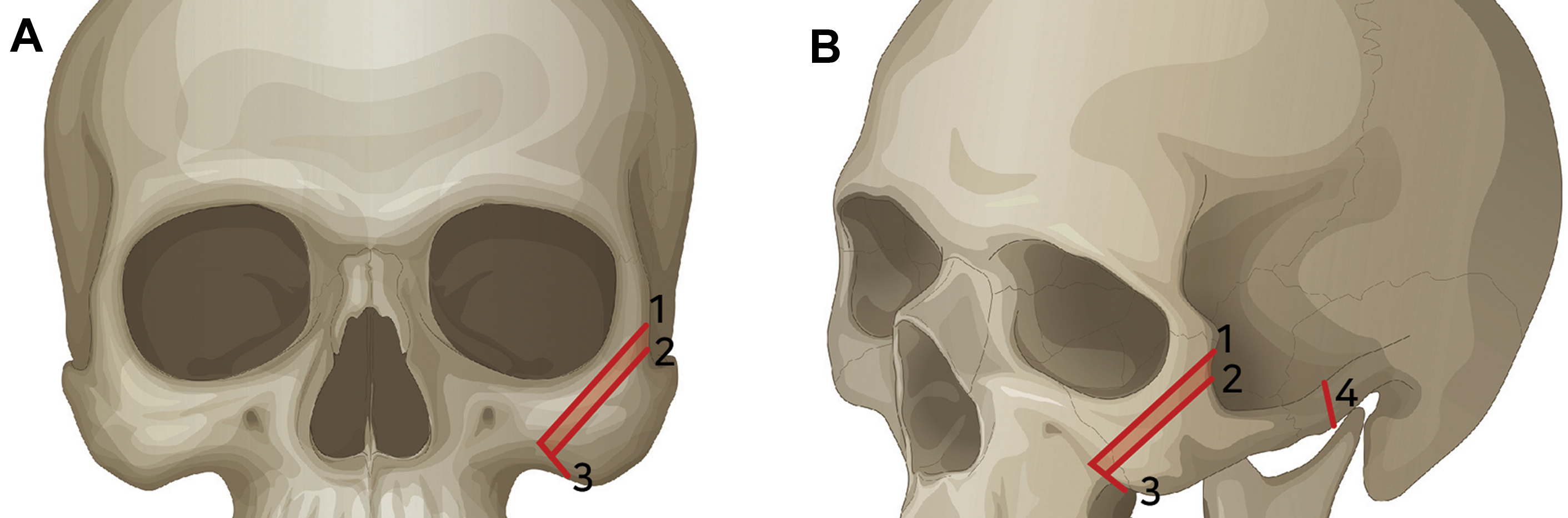
An L-shaped osteotomy of the zygomatic body is the preferred method for patients with moderate to severe malar protrusion caused by wide zygomatic arch and prominent body. An L-shaped osteotomy is made in the anterior part of the zygomatic body and a separate osteotomy is made in the posterior part of the zygomatic arch. The L-shaped osteotomy technique can change both the zygomatic body and arch; it also has the advantage of controlling the degree of reduction as well as the shape after reduction.
General anesthesia is recommended for all zygoma reduction surgeries. Either nasotracheal or endotracheal intubation can be used.
For the zygomatic approach, a standard upper labiobuccal vestibular incision is made on each side of the maxilla. The soft tissues are elevated superiorly and laterally. Dissection is done subperiosteally to the area of the zygomatic body, the anterior wall of the maxillary sinus, and the lateral and inferior orbital rim. As the dissection extends superolaterally over the malar eminence, a portion of the origin of the zygomatic major and zygomatic-cutaneous ligaments may be partially divided from the bony surface.
The course of the frontal branch of the facial nerve and the zygomatic arch is marked on the facial skin. About a 1-cm vertical incision is made within the sideburn, 2 to 3 cm anterior to the tragus. , This incision should lie posterior to the course of the facial nerve. The arch is identified after the dissection of the periosteum, and fine elevators are passed over the top and behind the arch and as far posteriorly as possible to ensure that the osteotomy is still anterior to the temporomandibular joint.
An L-shaped osteotomy line is marked over the malar eminence ( Fig. 7 ). This line generally extends medially from the lateral border of the orbital rim to just below the infraorbital foramen. The surgeon should be careful not to start the osteotomy too low from where the arch changes from a vertical to a horizontal direction, because this may result in insufficient volume reduction at the zygomatic body. The short limb of the osteotomy then turns at about a 90° angle toward the zygomaticomaxillary buttress. Great attention must be paid to avoid injury to the orbital contents or infraorbital nerve. A second, parallel line is drawn lateral to the first line to represent the strip of bone to be resected, allowing inset of the fragment. The distance of the second line from the first line depends on the patient’s preference and the width of the zygomatic body (see Fig. 7 ). A wider parallel osteotomy can be made for greater reduction; however, the usual width of the strip is 3 to 5 mm. A double-blade reciprocating saw with a distance of 2, 3, 4, 5, 6, or 7 mm between the 2 blades ( Fig. 8 ) was designed at our clinic and has proved to be very useful in achieving this goal. A simple osteotomy and repositioning of the zygomatic body alone usually cannot successfully reduce the size of the zygoma, which necessitates ostectomy and removal of bone. , Careful dissection is required in the zygomatic-pterygoid space to prevent injury to vessels, which may lead to profuse bleeding and postoperative bruising.