The principles of facial reconstruction are well established and some unique modifications apply to the non-White population. Anatomic and physiologic distinctions to this group give rise to alterations in design and surgical planning. Different ethnic groups have different skin anatomy and physiology and that should be taken into consideration. Healing differs among the different ethnic groups, affecting the final result regardless of method chosen. Variations in aesthetic units can lead to different flap selection and design. These should be considered for this population to maximize aesthetic outcomes and patient satisfaction.
Key points
- •
Ethnic distinctives should be identified before consideration of reconstructive options.
- •
Non-White skin is different in terms of anatomy and physiology from White skin.
- •
For nasal reconstruction, the subunit principle is often modified from the White model.
- •
The skin soft tissue envelope (SSTE) is usually thicker and more inelastic compared with White patients. Wider undermining may be required to achieve tension-free closure.
- •
Nonanatomic cartilage grafting of the nose is used extensively but primarily to prevent alar notching rather than lateral wall collapse.
Introduction
Facial cutaneous defects with subsequent reconstructions form a large part of a typical facial plastic surgical practice. Facial defects are usually a result of either resection of a tumor or trauma. Although the incidence of skin malignancies is higher in the White population, they also occur in other ethnic groups and present an equally challenging repair. Hispanic, Asian, and African American individuals account for 4% to 5%, 2% to 4%, and 1% to 2% of skin cancer cases, respectively. Because of the scarcity of skin cancers in non-Whites, there is less experience and literature on this topic.
It is imperative to realize that there are nuances when performing facial reconstruction in the non-White group of patients. As globalization occurs, the idea of beauty takes on a broader and more universal view. Despite this, there are ethnic distinctives that should be respected.
Discussion
Ethnic Differences
Before delving into the differences in reconstruction, the basic structural and physiologic difference in skin should be examined.
Skin structure
Contrary to common belief, there are no racial differences in the number of melanocytes. Differences in skin color are attributed to variations in melanosomes, which are the melanin-containing organelles in melanocytes and keratinocytes. The skin’s response to UV irradiation is dependent on the epidermal content of melanin and distribution of melanosomes. Because of the increased melanin in Asians, Hispanics, and African Americans, the classic signs of photodamage often manifest later in life. However, this increase in melanin also predispose other darker-skinned ethnic groups to postinflammatory hyperpigmentation (PIH). This may have a significant role when considering the normal course of healing with darker-skinned individuals, especially as it pertains to incision planning, scar revision, dermabrasion, and cosmetic facial surgery.
Skin phototype
The system of categorizing skin phototype was developed by Fitzpatrick. This differentiates the skin type based on color and response to sunlight and UV radiation. This classification allows clear and consistent communication when classifying patients across different ethnic groups. It also helps alert the physician to be aware that patients with higher Fitzpatrick skin types are more prone to developing PIH.
Skin healing
During the healing phase, PIH results from overproduction of melanin or an irregular dispersion of pigment after cutaneous inflammation. The intensity of the PIH may correlate with high skin phenotypes.
The incidence of keloids is variable and patients with darker skin tend to have a higher prevalence compared with lighter-skin individuals. It is the most common skin disease among ethnic Chinese in Asia and the fifth most common disease among Africans in the United Kingdom. ,
Facial proportion
When performing reconstruction, aesthetics and form should be a substantial consideration. There is some ethnic deviation of what is considered to be attractive. Asian women tend to prefer a small and less angular face, whereas Whites tend to accept a more defined mandible and protruding cheeks. In a study looking at facial anthropometric differences among workers in the United States, they found that African Americans have larger features than Whites with larger faces. Hispanics also have faces larger than Whites but have shorter nasal protrusion. Comparing North American Whites and Asians, there were significantly smaller mouth widths, greater intercanthal widths, shorter palpebral fissures and wider noses among the Asian population. These ethnic distinctions are real and should be considered before embarking on facial reconstruction. It is important to recognize that only rarely does a person of one ethnicity actually desire to look like another race.
Aging
A dynamic process, such as aging, can affect races differently for several reasons, including variations in fibroelastic fibers, sebaceous glands, skin thickness, and environmental exposures. A comparison between Chinese and European populations has shown that Chinese women are affected by wrinkles later than French women. As expected, both races have pigmented lesions as they get older; however, when Chinese women acquire these lesions they tend to have a greater number than French women. The knowledge of the differences in aging can play a role in surgical planning.
Cultural significance/sensitivities
In many Asian countries, elderly individuals often prefer a less extensive approach to repair of their cutaneous defects as compared with other ethnicities. The ultimate choice of reconstruction option obviously lies with the patient but the surgeon–patient interaction can have a significant impact and influence decision making. There are cultural beliefs and social values toward facial proportions that may affect the patient’s choice of reconstruction. The shape of the nose, mouth, lips, and forehead are said to influence one’s life and wealth. This could have a role in selecting the appropriate reconstruction option, especially if the surgery involves narrowing the nose and lips. A thick fleshy nose is believed to indicate wealth and prosperity, whereas thicker lips are said to reflect such positive traits as enthusiasm and kindness. Surgeons should have an honest, open discussion with patients about procedures that can potentially change the shapes of their nose and lips.
Treatment of Nasal Defects
Nasal anatomy
Studies have shown that African Americans have shorter, wider, and shallower noses. Ethnic variations of nasal morphology have been categorized to three general forms:
- •
Leptorrhine (“tall and thin”) nose, which is associated with White or Indo-European descent.
- •
Platyrrhine (“broad and flat”) nose associated with African descent. It is characterized with thick skin, low radix, bulbous and lower projected tip, short dorsum, and flared nostrils.
- •
Mesorrhine (“intermediate”) nose that is associated with Asian or Latino nose. It is characterized by a low radix, rounded and less projected tip, variable anterior dorsal projection, and rounded nostrils.
These ethnic variations are only meant as a guide and categorizing all non-White noses to be just “ethnic” is overly simplistic.
Skin thickness plays a major role when planning for reconstruction. This is most apparent in the nose, where skin thickness differs depending on the location. The nasal skin is thinner in the upper portion and becomes tighter and more adherent in the lower portion. Patients with thinner skin soft tissue envelope (SSTE) often have a higher risk of postoperative atrophy and possible discoloration from vascular congestion, whereas patients with thicker SSTE are more likely to have increased postoperative edema. The edema may impact scar healing and camouflage and refinement of the nasal tip and fullness to the supratip.
Asians and African Americans tend to have thicker and less extensible skin with more abundant subcutaneous soft tissue than noses of Whites. Eggerstedt and colleagues have demonstrated that African American patients have significantly thicker SSTE at the supratip than all other races. Asian Americans also demonstrate thicker SSTE at the supratip than occidental patients.
Nasal subunits
Generally, in the White population, reconstruction using the subunit principle has yielded good results. These subunits were not as appropriate for Asian patients. The soft tissue triangle is not distinct; the distinction between other subunits is not as sharp as with Whites. This is mainly caused by the thick skin and weaker underlying cartilages. When considering the resultant scars for a nasal reconstruction, these ethnic differences must be considered at the forefront. Generally speaking, the softer and more rounded nature of the non-White nose leads to less defined aesthetic units and thus they have a more minor role in flap selection and design.
Functional difference
The internal nasal valve is defined as the area between the caudal border of the upper lateral cartilages and the dorsal cartilaginous septum. In White noses, this angle is said to be 10° to 15°. In African American and Asian noses, this angle of more obtuse, making them less susceptible to internal nasal valve collapse and nasal obstruction. Knowledge about the internal nasal valve is crucial in the White and non-White population because there are maneuvers that could potentially cause narrowing and collapse.
Management of specific nasal defect
Primary closure is considered if the nasal defect is small and there is minimal distortion of the nose. In non-White noses, where the skin is less extensible, this technique may not be used as much.
Skin grafting is an easy technique and useful in closure of various defects. However, for most defects of the nose, it is not an ideal choice because of the difficulty in matching texture and color. This is especially true in non-White noses where the SSTE is thicker.
Local flaps tend to be the reconstructive option of choice for many nasal defects. Local flaps are often robust and provide good texture and color match. Because of the thicker and less extensible nature of the SSTE in non-White patients, wider undermining is usually required to achieve the stretch required for tensionless defect closure. Additionally, the Asian nose tends to be smaller in size and local flaps are more limited in versatility. Many tables and algorithms found in the medical literature reference the White nose in terms of overall size. This is misleading.
Case study 1
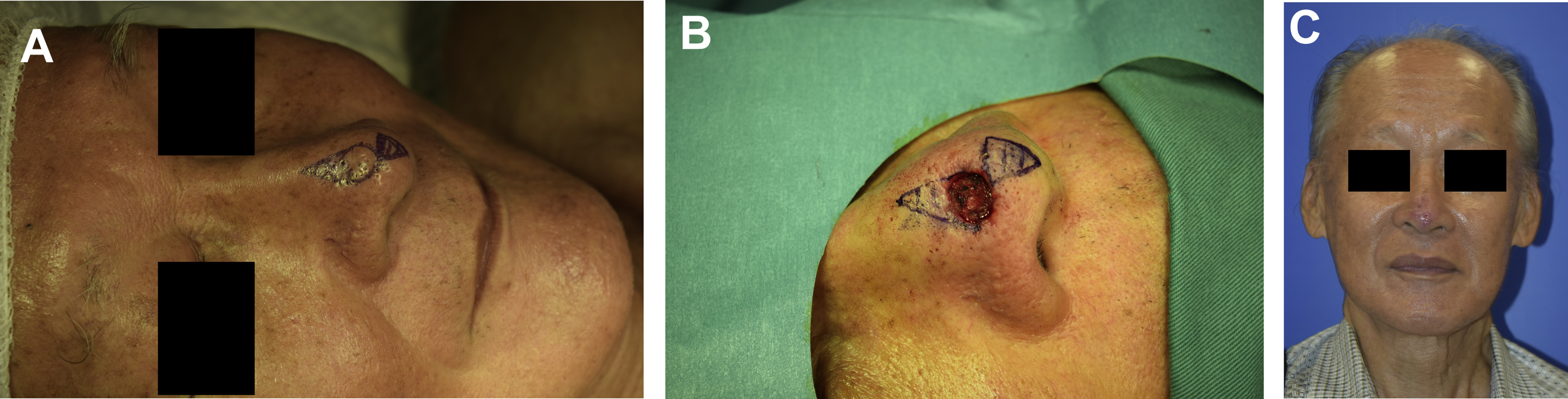
Fig. 1 shows a middle-aged Korean man with basal cell carcinoma. After Mohs surgery, he had a small nasal defect at the nasal tip. The nasal tip skin is more sebaceous especially in Asian subjects. Bilateral advancement flap was designed for closure of the defect, with standing cutaneous defects immediately above and below the defect. The resultant scar is in the midline with minimal distortion of alar rims.

Case study 2
Fig. 2 shows an elderly Chinese man with basal cell carcinoma and 8-mm defect of the nasal tip after excision. While planning for reconstruction, note the SSTE of the nasal tip is thick and sebaceous. In planning the East-West flap, the inferior standing cutaneous deformity was moved to the midline infratip lobule segment. Wide undermining is generally required because of the relative inelasticity of the sebaceous skin.
Similar to White nasal defects, nonanatomic cartilage grafting is used extensively. However, according to Jin and colleagues, nasal grafting is often used to prevent alar notching rather than for functional purposes and lateral wall collapse.
Choice of local flaps used depends on mainly the site, size, and depth of the defect. For many alar defects, the flap of choice is an interpolated melolabial flap. For larger defects, forehead flap should be considered.
In the design of forehead flaps, there are subtle modifications as suggested by Hsiao and colleagues for reconstruction of Asian noses. The Asian SSTE is generally thicker with more fibrofatty tissue at the nasal tip. For this reason, flap thinning is less imperative and performed in a more conservative manner. They found that framework reinforcement was necessary in patients because of the unpredictable flap contracture. Therefore, it was recommended to thin the flap conservatively to match the skin thickness and to strengthen and overbuild the structural framework to counter the contractile forces of a healing forehead flap.
Case study 3
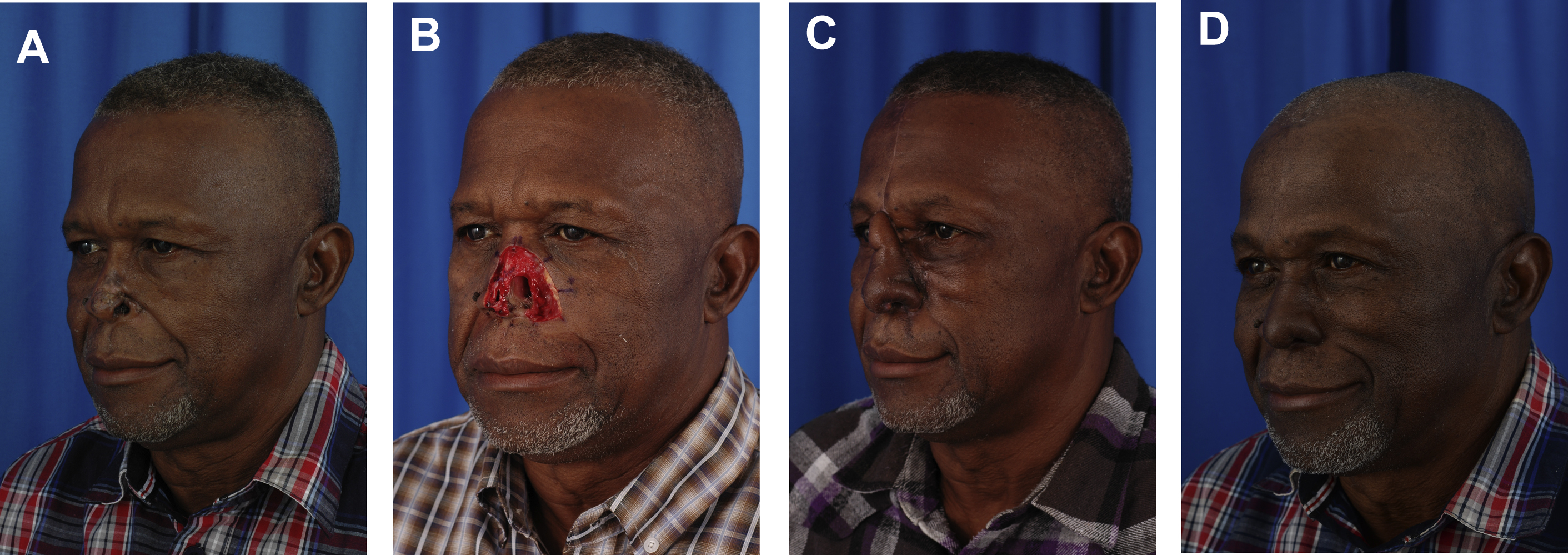
Fig. 3 shows a middle-aged African American man with extensive basal cell carcinoma involving the nasal tip, dorsum, and the alar. After Mohs excision, the patient had a large, full-thickness nasal defect involving the nasal dorsum, nasal tip, left nasal sidewall, and left nasal alar. He underwent multiple staged reconstruction with forehead flap as skin coverage, full-thickness skin graft for nasal lining, costal cartilage for framework support, and composite concha grafts for support and lining. Left cheek advancement flap was also performed. Costal cartilage was used to reconstruct the dorsal strut. Composite concha graft was harvested from the right ear and used to reconstruct the lining and the left alar rim.
Case study 4
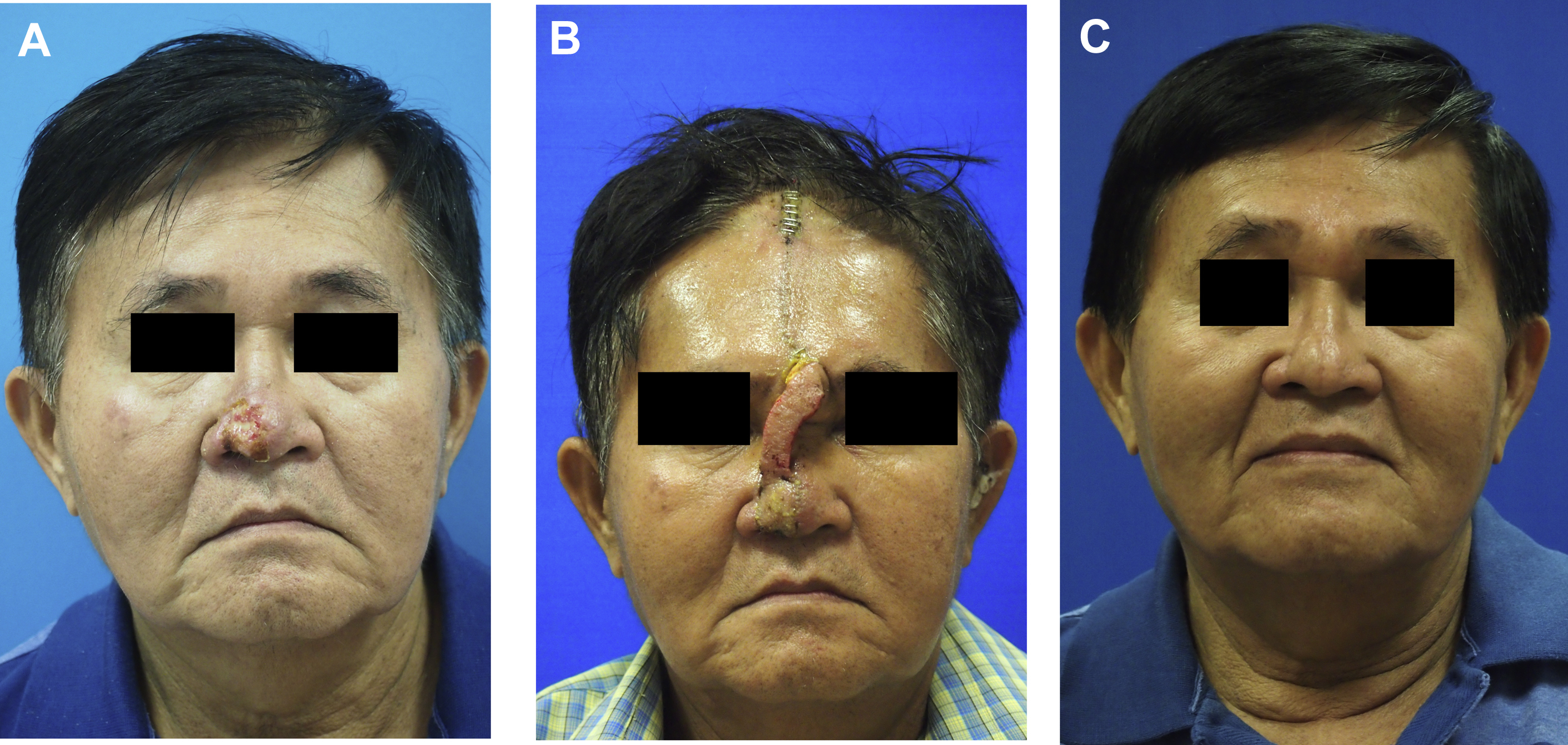
Fig. 4 shows a middle-aged Chinese man with right nasal basal cell carcinoma involving the nasal tip, the right nasal alar, with a resultant large nasal defect after excision involving the nasal tip and alar. Forehead flap was planned for skin coverage and concha cartilage nonanatomic grafting to support the nasal alar. Cartilage graft was mainly used to prevent alar notching. During the harvest of forehead flap, it is important to match the skin thickness of the surrounding skin.
Treatment of Periorbital Defects
Periorbital anatomy
It is well known that there are many differences between the Asian and White eyelid. There is generally more prominent subcutaneous, suborbicularis, and pretarsal fat tissue in the Asian upper eyelid. This pretarsal fat is considered to be a spacer that prevents levator aponeurosis from extending to the subdermal tissue in single eyelid crease people. In Asians, the preaponeurotic fat is much lower than that in Whites. Epicanthi are folds of skin in the medial canthal area and Asians tend to have this fold of skin that hides the caruncle.
Globe protrusion and interpupillary distance in African American patients tend to be greater compared with White patients. ,
Whites also have more prominent supraorbital bones, whereas Asians have low supraorbital bones.
Management of specific periorbital defects
Local skin flaps are the preferred reconstructive option of choice in anterior lamellar defects. Skin grafts usually do not have appropriate color and texture match. The color mismatch maybe more apparent in other ethnic groups because of the PIH. Common flap designs are rhombic flaps and V-Y and Y-V advancement flaps. For superior eyelid defects, the absence of supratarsal creases in the Asian population can lead to increased difficulty in hiding the resultant scar.
Generally, second intent healing is not acceptable in upper eyelid defects. The exception is the medial canthal region where defects less than 1 cm can heal well with second intent. However, in the Asian population with prominent epicanthal folds, the scarring is difficult to predict and this may result in asymmetry, which can be jarringly obvious, especially if the epicanthal fold is disrupted unilaterally. Medial canthal symmetry in the Asian patient is especially challenging to correct and requires a more elaborate and thoughtful repair from the onset.
Treatment of Cheek Defects
Cheek anatomy
The surface anatomy and contour of the face depends on the underlying bony structures and on the overlying soft tissues. The facial skeleton, which forms the foundation of the face, is obviously different depending on the ethnicities. There are also differing physical characteristics of the skin and the soft tissue between the ethnic groups. The Asian skeleton generally has a wide and flat midface, with prominent zygomas, small nasal bones, and wide mandible angles. The African American skeleton tends to have a bimaxillary protrusion, orbital proptosis, with increased facial convexity. The Latino and Hispanic face generally has increased bizygomatic distance, bimaxillary protrusion, with more receded chin.
Different authors have sought to describe and define the aesthetic subunits of the face. According to Gonzalez-Ulloa and coworkers, the cheek is divided into three aesthetic subunits: zone I includes the suborbital region, zone II involves the preauricular region, and zone III encompasses the bucomandibular region. Bradley and Murakami have divided the cheek into medial, lateral (mandibular), zygomatic, and buccal divisions. It is generally agreed that the primary goal during reconstruction is to restore skin color and texture, which are more obvious than contour and subunit outline variations.
Reconstruction of specific defects
Generally, the same principles apply in White and non-White patients. Reconstruction should be tailored accordingly in each patient, taking note of their defect size and their location. Immobile landmarks should be respected and care must be taken to avoid any shift or distortion. Resultant scars are always considered but different across ethnicities.
Direct closure in general should be considered as the first line for closure of cheek defects if there is no distortion of adjacent tissue. If direct closure is not possible, the next option is a local flap. When planning for cheek flaps, the mobility and laxity of the skin surrounding the defect should be assessed. The resultant scars should ideally lie at the border of aesthetic units, the nasofacial sulcus, alar-facial sulcus, melolabial crease, or along relaxed skin tension lines (RSTL) to best camouflage them. This may be difficult to achieve in patients with taut and wrinkle-free skin. In Kim and coworkers’ study on cheek defects, they avoided the use of bilobed flaps because of unsatisfactory scarring in Asians. They opted instead for either V-Y advancement flap or rhombic flap.
For cheek defects adjacent to the nasal ala, lateral nasal wall, and inferior orbital rims, usually large cervicofacial flaps or rotational flaps are required. In younger patients or patients with better orbicularis oculi tone, the scar is camouflaged in the subciliary line. However, care has to be taken to avoid ectropion and inferior lid retraction, especially in individuals with lax lower lids.
With larger defects, the cervicofacial flap remains the reconstructive option of choice. With a large flap and visible scar, the concept of healing in the non-White population becomes pertinent. Meticulous tension-free skin closure with good wound care form the foundation to achieving good results.
Summary
There are a few key principles in facial reconstruction that should be observed regardless of ethnicity. The principles of restoring facial harmony and symmetry should be foremost in any reconstructive surgeon’s mind. With different ethnicities, however, there are nuances to consider that include facial anatomy, skin physiology, and cultural norms and expectations. Integrating these variables improves outcomes and patient satisfaction.
Clinics care points
- •
Ethnic distinctions are part of the consideration of reconstructive planning.
- •
Different ethnic groups have different skin anatomy and physiology and that should be taken into consideration. Variations in aesthetic units can lead to different flap selection and design.
- •
Healing differs among the different ethnic groups, affecting the final result regardless of method chosen.
- •
For reconstruction of nasal defects, the SSTE difference between the ethnic groups has to be considered before choosing an appropriate reconstructive option.
- •
The principles of symmetry and harmony remain as the central pilar when performing facial reconstruction with the goal of allowing the repair to appear as inconspicuous as possible.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


