Typical Asian deformed nose has many different types: concave nasal dorsum, low nasal dorsum, wide nasal dorsum, deviated nose, convex nasal dorsum, saddle nose, short-nose deformity, and deformities involving irreversible damage of skin/soft tissue envelop are the most representative ones. The key concept in Asian rhinoplasty is augmentation in all different forms of nasal deformities. Augmentation of the nose consists of framework, tip, and dorsal augmentation. Septal extension grafting and tip grafting are 2 maneuvers with profound importance in augmentation of lower two-thirds of the Asian nose. Dorsal augmentation is central concept in beautifying all different types of deformed noses, even the hump nose.
Key points
- •
Asian noses tend to have a weak and small cartilage framework and flat and thick nasal bone, thus resulting in a low radix and dorsal height. Hence, in most of rhinoplasty surgeries among Asians, augmentation is important.
- •
Augmentation of the nose should be achieved by framework augmentation and tip augmentation and dorsal augmentation.
- •
Typical Asian deformed nose has many different types: mildly concave nasal dorsum, severely concave or low nasal dorsum, wide nasal dorsum, deviated nose, convex nasal dorsum, saddle nose, short-nose deformity, and deformities involving irreversible damage of skin/soft tissue envelope and nasal skeleton are the most representative ones.
- •
Various kinds of techniques are needed to correct different types of deformities where a dorsal augmentation is a critically important concept to accomplish aesthetically pleasing surgical outcome.
Introduction
Despite the lack of general and scientific consensus on its definition, a deformed nose is characterized as one that has an obvious deviant shape. From a frontal view, a wide nasal dorsum and deviated nose can be considered as deformity. From a profile view, a hump or low-profile nose, saddle nose, upturned nose, long nose with ptotic tip, or a nose with columellar retraction can be problematic. This article aims to address the important points for successful correction of deformed noses of East Asian individuals. Although there is huge variation, the tip of the East Asian is usually low and the lower lateral cartilages are small and weak. The nasal bones are flat and thick, resulting in a low radix and dorsal height. Because the septal cartilage of some Asians is thin and small, the size and quantity of harvestable septal cartilage may be inadequate for complex rhinoplasty procedures, increasing the need to harvest grafts from other sites. Hence, in most of rhinoplasty surgeries among Asians, augmentation is important. Aesthetic perfection of the nose is determined by the height and shape of the nasal dorsum seen from the profile and frontal views, with its harmonious alignment with the nasal tip. The augmentation should be achieved by framework augmentation and tip augmentation and dorsal augmentation. In framework augmentation, spreader and septal extension grafts are added to the native septal cartilage, by which the surgeon can secure strong nasal bases that can withstand subsequent tip augmentation and dorsal augmentation. Tip augmentation is usually performed with grafting procedures such as onlay grafting, shield grafting, and multilayer tip grafting using autologous cartilages. Once the desired height and shape of the tip is acquired by aforementioned procedures, subsequent dorsal augmentation should be done using various materials. Dorsal augmentation is the most frequently performed procedure in Asian rhinoplasty; it is critically important not only in simple cosmetic rhinoplasty but also in all types of rhinoplasties to achieve aesthetic perfection. In this article, rhinoplasty procedures for different types of nasal deformities will be introduced.
Treatment strategies for various forms of deformed noses
Mildly Concave Nasal Dorsum
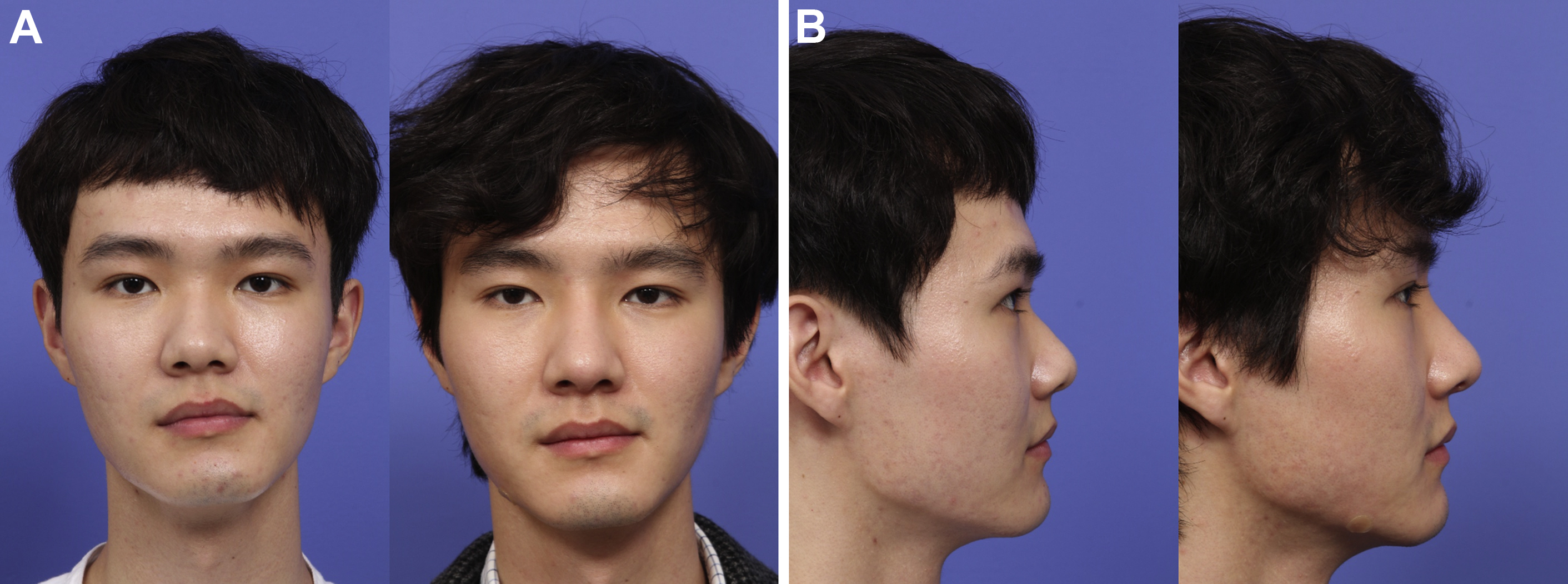
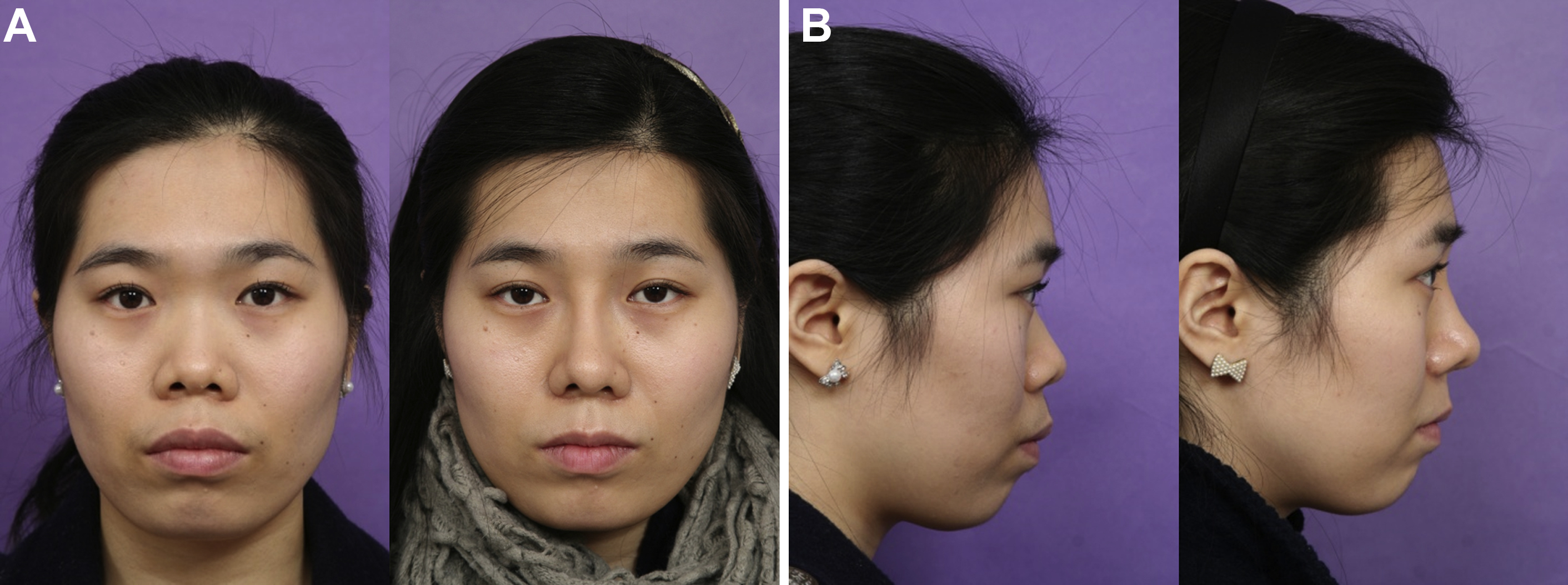
Although the female population generally favors this type of nasal profile, men with mildly concave nasal dorsum prefer a straighter dorsal line, thus seeking rhinoplasty. Various types of dorsal implants can be used to augment this type of nose. For example, alloplastic implants such as thin silicone and expanded polytetrafluoroethylene (ePTFE) may be suitable. In addition, autologous materials such as fascia-wrapped diced cartilage, free diced cartilage, and glued diced cartilage are also adequate material. The degree of augmentation desired by the patient must be determined by a thorough consultation. For example, patients desiring a slight augmentation may not require tip work, whereas patients desiring substantial augmentation should undergo tip augmentation before dorsal augmentation to create a harmonious tip–dorsum relationship ( Fig. 1 ).
Severely Concave or Low Nasal Dorsum Without an Upturned Tip
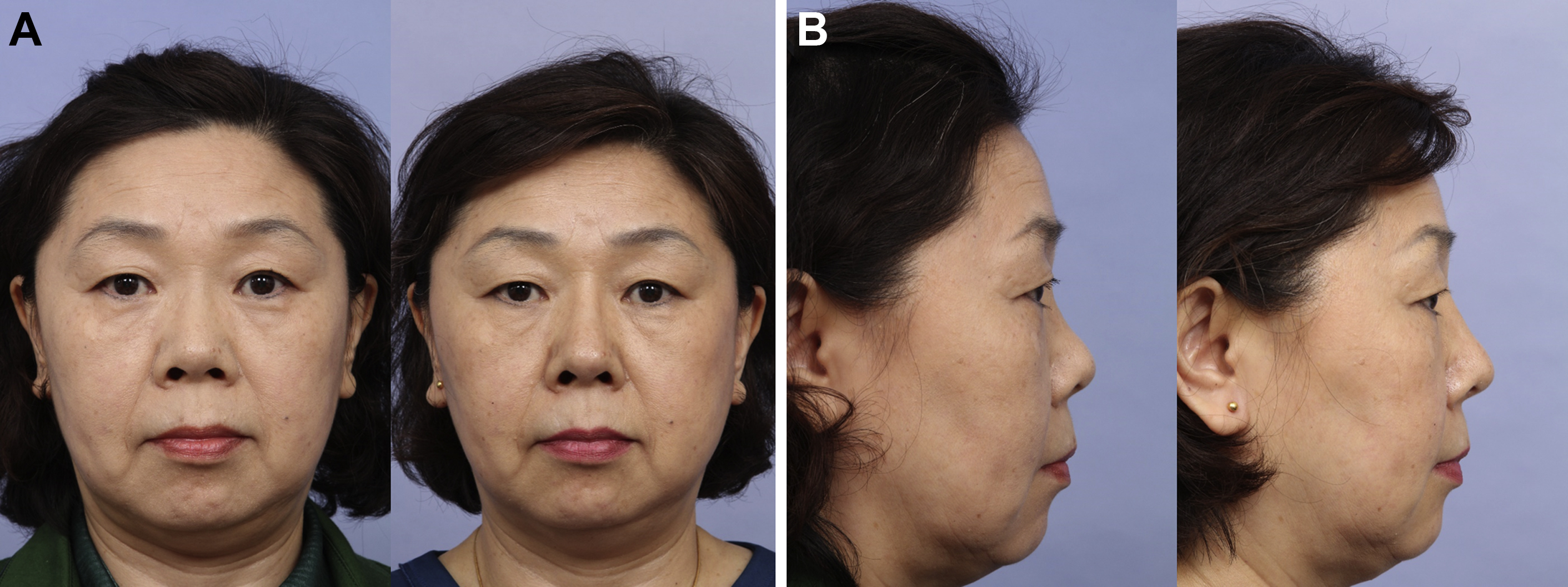
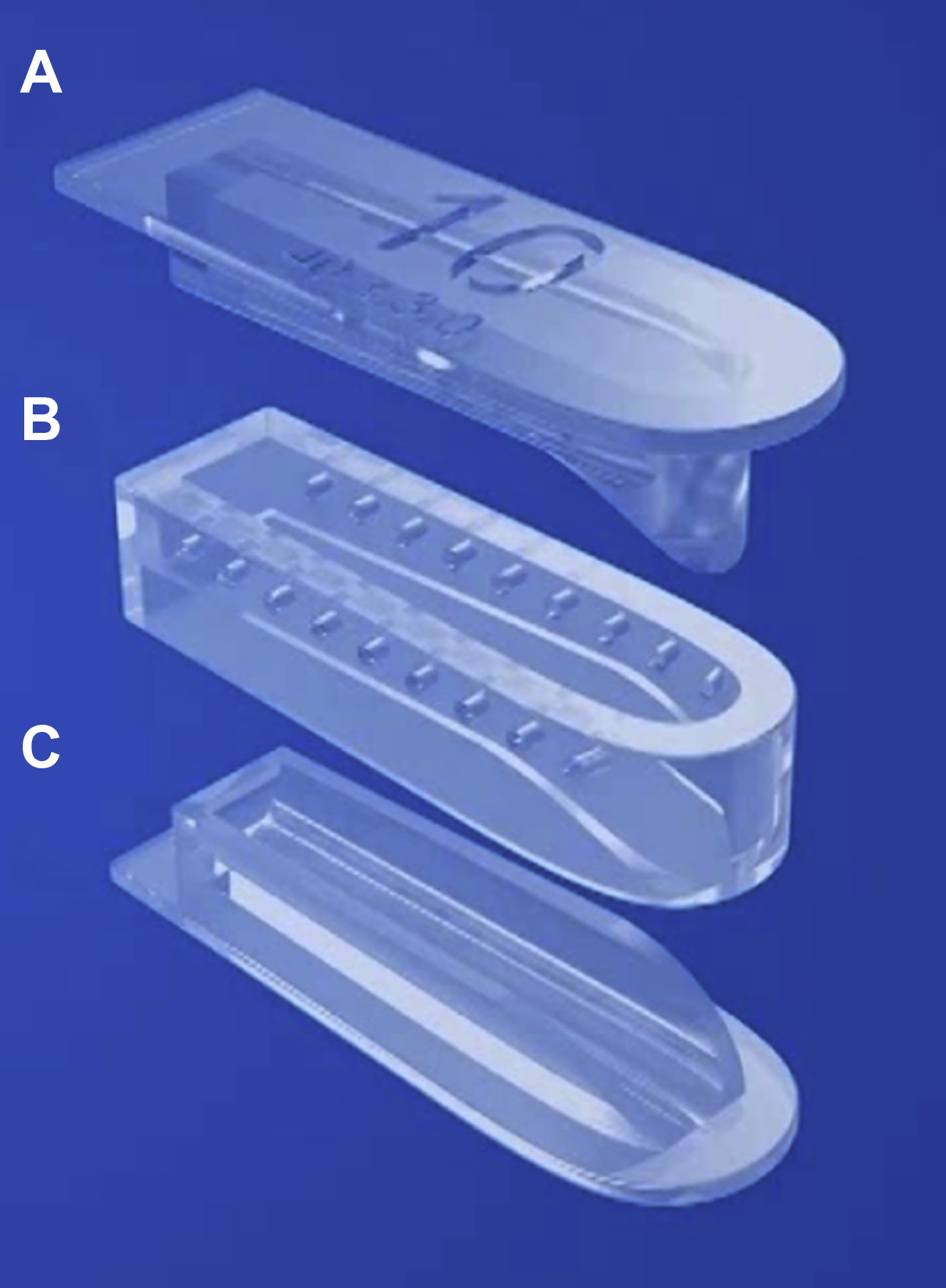
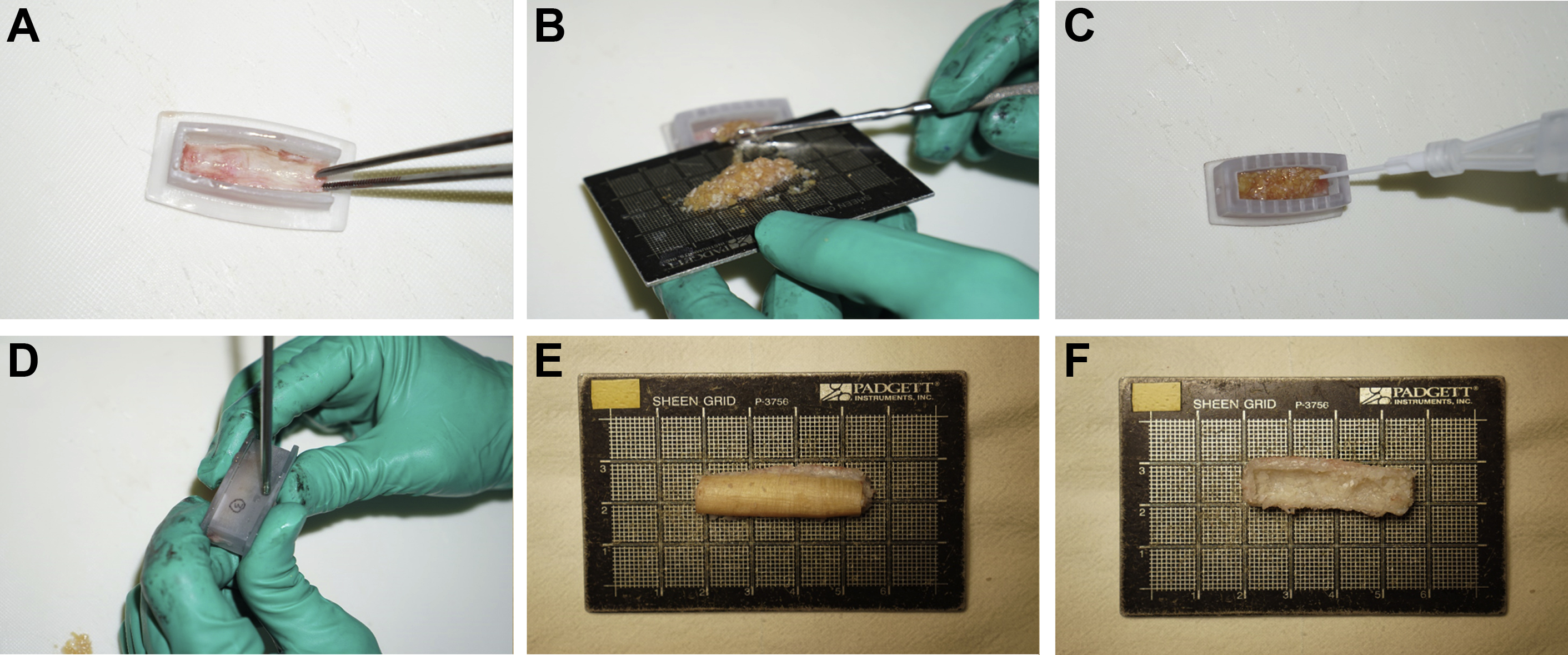
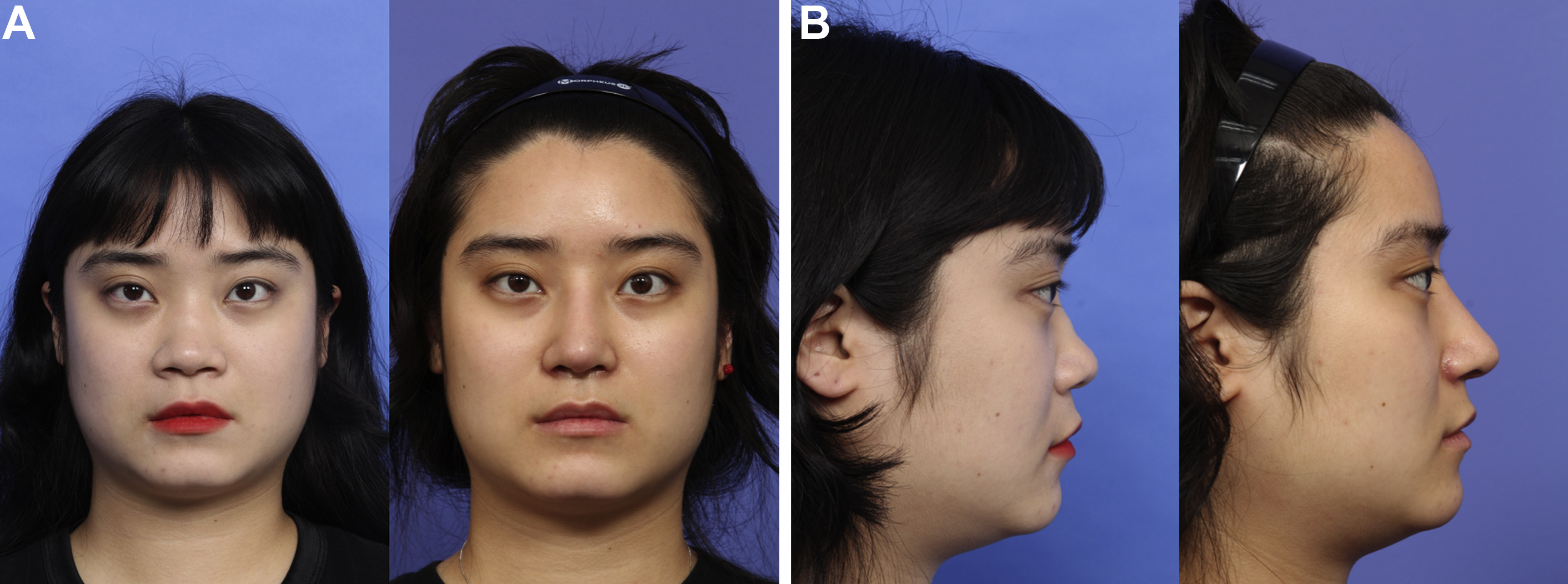
This deformity is relatively common in the East Asian population ( Fig. 2 ). The pathology underlying this deformity is a usually poorly developed cartilaginous dorsum and nasal bone. To beautify the profile line, this type of nose usually requires major septal reconstruction and tip augmentation before dorsum management. Augmentation of the nasal dorsum without reconstructing the poorly developed septal cartilage often causes the dorsum to sink under the weight of the dorsal implant. Because the correction of deformity highly demands a significant quantity of graft materials, costal cartilage is considered the most ideal graft source. Among the methods used to enhance septal support, the authors prefer to sandwich a caudal septal extension graft, placed end-to-end with the caudal septum, between 2 extended spreader grafts, slightly extended dorsally and caudally. If the increase in the tip height augmentation is insufficient, additional tip grafting is required. Subsequent dorsal augmentation should be done thereafter. This article recommends costal cartilage for dorsal augmentation material, as it is already harvested for framework augmentation. For dorsal augmentation, an autologous costal cartilage can be used in a solid mono-block form or in diced cartilage. Although augmentation using a mono-block carved implant may seem simple, carving is actually difficult and the graft can be bent or warped during the postoperative period. Furthermore, it is difficult to create a natural-looking smooth dorsal contour. To avoid problems inherent to the solid carved cartilage, augmentation with finely diced cartilage is becoming increasingly popular. Diced costal cartilage is used for dorsal augmentation as fascia-wrapped implant, glued graft, and free diced cartilage. , The authors prefer the technique of glued diced cartilage. In this technique, bonding diced cartilage with fibrin glue is performed instead of placing it in a fascia sleeve. Thus, this technique requires a mold to create the desired shape. Manually molded glued diced cartilage graft using a half-cut syringe has been reported to be useful. However, the false volume caused by fluid and glue around the diced cartilage is difficult to control with this method, and using a half-cut syringe makes this method cumbersome. Thus, the senior author developed a mold for the glued diced cartilage graft technique to get more refined control of the shape, thickness, and length of the diced cartilage implant for dorsal augmentation. The mold comprises the base template, guarding frame, and compressor ( Fig. 3 ). In this technique, harvested autologous fascia/perichondrium or homologous fascia lata can be used as a covering material at the convex side of the implant to prevent dorsal irregularities. Making the dorsal implant starts with applying 1 or 2 drops of the fibrin glue onto the covering material placed on the base template, and the guarding frame of the mold is assembled. Then, a thin layer of diced cartilage is placed on top of the fascia or perichondrium, a second layer of glue is painted, an additional layer of diced cartilage is laid on top, and glue is painted over the second layer of diced cartilage. Finally, the compressor of the mold is applied and manually pressed. Through the small holes of the sidewall, excessive glue and fluid around the diced cartilage are drained and suctioned out. After carefully disassembling the molds, the graft for dorsal augmentation is obtained. The implant has a convex outer surface with or without a soft-tissue cap, whereas the undersurface has a concave shape conforming to the convexity of the nasal dorsum ( Fig. 4 ). The graft is then placed onto the nasal dorsum usually in one piece but sometimes in a segmental fashion at the radix and supratip dorsum. Because molded diced cartilage graft with glue is in a semisolid state, it is important to handle it cautiously so as not to break the molded cartilage implant. The final shaping of the implant can be achieved by gentle manual molding over the skin-soft tissue envelope.
Wide Nasal Dorsum
In a Caucasian nose, a wide nasal dorsum is often attributed to the broad nasal bone and cartilaginous dorsum, which requires the dorsal-width narrowing by osteotomy. However, in Asians, this deformity is usually associated with a flat low-profile nose with a poorly developed nasal skeleton, which cannot create a distinct brow-tip aesthetic line, thus giving an impression of a wide nasal dorsum ( Fig. 5 ). In this case, osteotomy is not suitable to narrow the dorsum. Instead, dorsal augmentation is the mainstay for creating an aesthetically pleasing brow-tip aesthetic line. Furthermore, subjects with broad nasal dorsum usually have thick skin and poorly developed alar cartilages causing an underprojected and amorphously defined nasal tip. For the correction of the broad nasal dorsum, a significant tip projection using septal extension graft with or without tip grafting should be done, and subsequent dorsal augmentation is needed to create a well-balanced brow-tip aesthetic line.
Deviated Nose
Correction of a deviated nose is a complex issue that cannot be simplified, where dorsal augmentation is often the neglected procedure. Dorsal augmentation is one of the last steps in correcting deviated noses. To correct the deviation, procedures such as osteotomy or spreader graft are frequently used, but these maneuvers can cause dorsum irregularities in patients with thin skin. Moreover, surgical maneuvers to straighten cartilaginous dorsum and bony dorsum cannot perfectly correct the deviated appearance of the nose. As such, when the underlying nasal skeleton is not straight in the midline, rather tiled, dorsal augmentation can neutralize and mitigate the deviated nasal skeleton, so that the final shape of the nose looks straight. Subjects with deviated nose also show contraction of the tissue and the soft tissue where their deviation was originally located; appropriate dorsal augmentation and camouflage can correct the soft tissue deformities that cause deviation. Implant materials for augmentation should be small in volume and soft. Because the correction of deviation requires extensive dissection and may weaken the underlying structure due to osteotomy and septal correction, dorsal augmentation with solid materials such as silicone or costal cartilage can easily be displaced or deform the underlying nasal skeleton by its weight. It is therefore recommended to use soft implant materials such as ePTFE, fascia, conchal cartilage, crushed septal cartilage, diced cartilage, and fascia-wrapped diced cartilage for dorsal augmentation ( Fig. 6 ).