The goal of Asian blepharoplasty is to create a lid crease configuration that resembles the natural-appearing crease found in other Asians. Because the Asian upper eyelid contains more prominent preseptal fat resulting in greater lid fullness, soft tissue work in blepharoplasty of the Asian eye is even more diverse and essential than that of whites in order for there to be the sustainability of the eyelid crease. Hence, Asian blepharoplasty should be performed specifically following the orbital anatomy of Asians. This article details the incisional method of blepharoplasty to create natural-appearing creases for Asians with single eyelids.
Key points
- •
Soft tissue work in blepharoplasty is even more critical in Asians than in whites, for long-term sustainability of the eyelid crease.
- •
During the evaluation, always check the position of the eyebrows. When compensated brow ptosis is anticipated, a preoperative explanation of the relationship between eyebrow change and the double eyelid should be given.
- •
Orbital fat manipulation is an important consideration in double eyelid surgery, because the shape and height of double eyelids change according to the amount of orbital fat.
Introduction
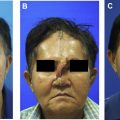
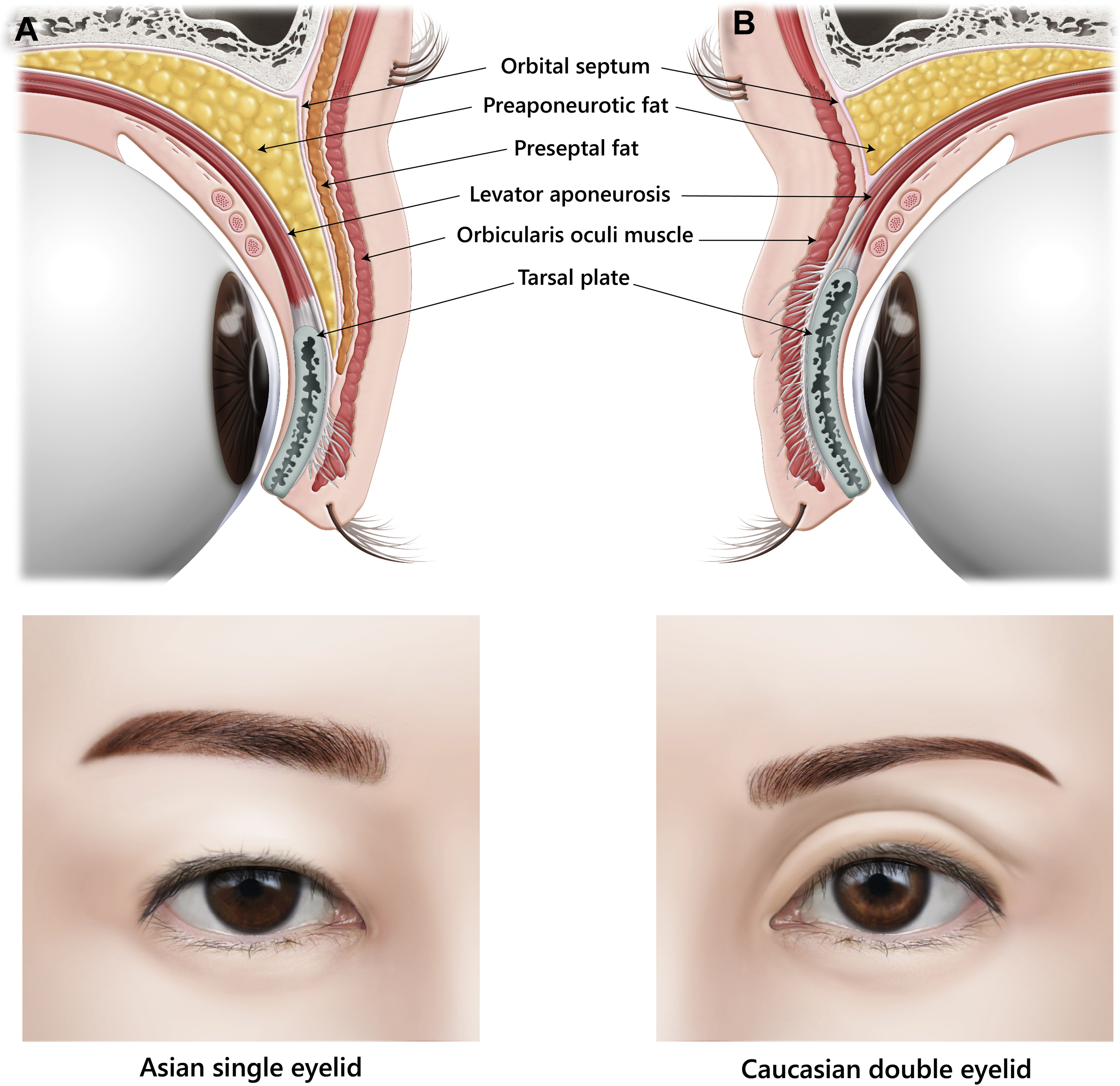
Asian blepharoplasty (double eyelid surgery, supratarsal crease [STC] surgery) refers to the surgical creation of a STC in Asians and should be distinguished from the traditional upper blepharoplasty for persons of Western descent. The most obvious characteristic of the Asian eyelid is the absent or very low lid crease and fuller upper eyelid. White eyelids typically have a double eyelid; however, Asian eyelids can be categorized into 3 types: single eyelid, low eyelid crease, and double eyelid. The presence, position, and depth of the STC are highly variable in Asians (usually lower than that of whites, in the range of 2–5 mm from the eyelid margin), and it is absent in approximately 50% of Asians. Most single eyelid eyes look swollen and heavy because of the prominent fat pads and the thick skin of the upper eyelid, and the pupils are less exposed, making the eye appear less fresh ( Fig. 1 A).
The anatomic difference from whites eyelid
Less Cantilevered Orbital Bone/Transition Area
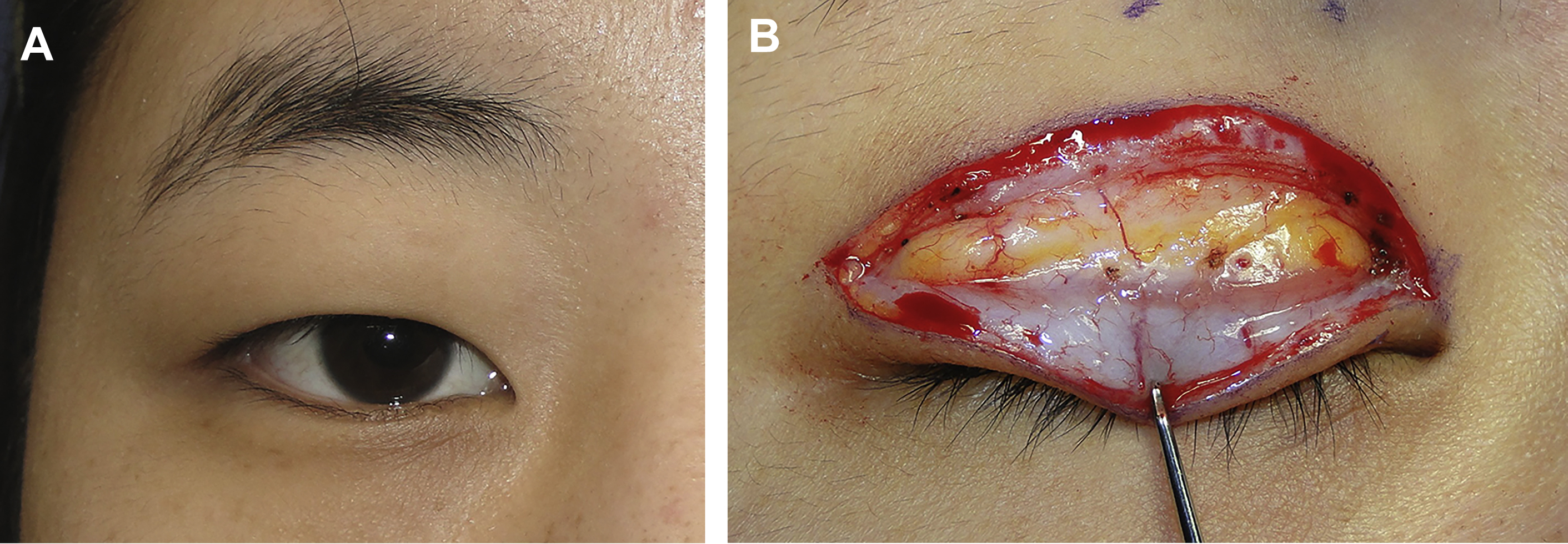
The most important anatomic differences between the eyes of whites versus Asians are that the former possess cantilevered orbital rims with deeper set globes, which results in the formation of an eyelid crease. In contrast, Asian eyes typically have shallow orbits and supraorbital ridges with minimal to no cantilevering, resulting in there being a transition area between the orbital rim and STC, a characteristic that is absent in non-Asians , ( Fig. 2 A). The white upper lid crease coincides with the orbital rim, whereas the Asian crease typically arises a fair distance below the orbital rim, owing to the flat supraorbital ridge. If a double eyelid is made without a transition area in Asians, it becomes a very unnatural and awkward double eyelid, not a Westernized eye (see Fig. 2 B, C).
Epicanthal Fold
Although the epicanthal fold can manifest across a range of ethnicities, it is a major anatomic feature of the Asian upper eyelid, occurring at frequencies of 60% to 90%. The epicanthus represents a remnant fibromuscular volume on the upper medial canthal region, that often obscures the medial canthus and is characterized by vertical skin shortage and tension that causes difficulty in horizontal skin folding. , It acts as a major hindrance to double eyelid formation in Asian blepharoplasty.
Although the standards of the beauty of the East and the West differ, even in the East there is a preference for large eyes with narrow interepicanthal distance. Because the epicanthal fold can cause telecanthus, epicanthoplasty is often used to make a larger horizontal palpebral fissure.
In patients with severe epicanthal fold, surgery results are often poor if double eyelid surgery alone is performed without also addressing the epicanthus. Severe epicanthal folds are a common cause of STC loss after blepharoplasty ( Fig. 3 ), as the preexisting vertical skin tension caused by the epicanthal fold acts as tensional stress on the newly formed surgical crease. In such cases, medial epicanthoplasty is necessary in order to remove this vertical tension, so that the newly created STC cannot be easily undone.

Orbital Fat Pads
The amount of orbital fat (OF) varies according to race and gender. There may also be variability between an individuals’ left and right eye ( Fig. 4 ). OF manipulation is very important because the shape and height of the double eyelids will change according to the amount of OF present. In Asians, OF protrudes downward to the front of the tarsal plate in an apronlike configuration, resulting in a somewhat puffy upper eyelid. The OF sac is a very delicate structure, and numbness of the upper eyelid following blepharoplasty may represent injury to the terminal branches of the ophthalmic division of the trigeminal nerve, which pass superiorly and superomedially to the fat in the upper OF compartments. To prevent this complication, the OF sac should not be removed along with the fat. Instead, the OF sac must be opened to remove the fat. As the OF pad is a critical structure that forms the glide zone between the levator aponeurosis (LA) and the septum, one should be very conservative with its removal. , Excessive fat removal is not recommended in Asian blepharoplasty, as it may result in unsightly deep folds, extra creases, or a sunken appearance.

Fibrous Structures on the Levator Aponeurosis
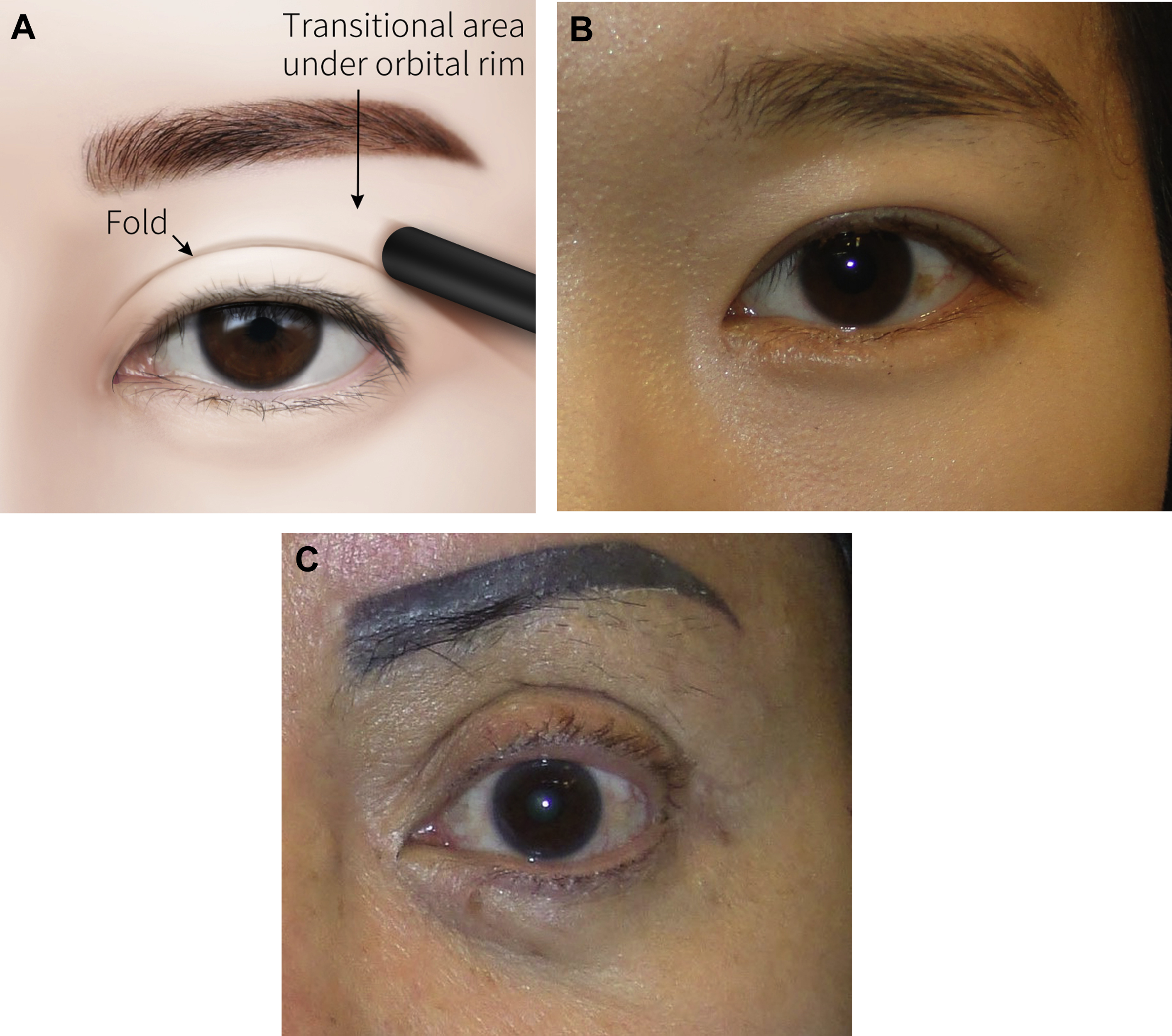
When the orbital septum is incised, the OF pads that herniate outwards are retracted to reveal within the lower aspect of the preaponeurotic fat space a transverse fibrous structure, that differs from the higher positioned Whitnall ligament, called the lower-positioned transverse ligament (LPTL) ( Fig. 5 A). This loose yet inelastic structure spans superomedially to inferolaterally and can be identified in almost every upper eyelid. Although Whitnall ligament is located on the levator muscle, the LPTL is located just above the fusional line between the orbital septum and the LA. , Within the preaponeurotic space, the superficial expansion of the LA turns up around the LPTL to become the orbital septum. Hence, contraction of the levator muscle leads to retraction of the preaponeurotic fat against the LPTL. The LPTL is thought to determine the low position of the preaponeurotic fat and can restrict the vertical width of the palpebral fissure. ,
In addition, on the upper aspect of the smooth, fascia-like surface of the LA, fatty tissue as well as tough fibrous web bands are commonly encountered (see Fig. 5 B). These fibrous web bands between the LA and OF can limit movement of the LA, which is a cause of eye-opening limitation. Subclinical and mild blepharoptosis can be corrected by releasing these fibrous bands without manipulating the LA or the Müller muscle. ,
The anatomical principles of the double eyelid
Although the exact mechanism remains controversial, , the STC is thought to be an anatomic invagination of the eyelid skin along the superior tarsal border. There exists a superficial fascia beneath the orbicularis oculi muscle (OOM), which fuses with the LA at the lid fold level. Below the fold, these fasciae remain fused or “conjoined.” Thus, the external fold in the upper eyelid reflects this internal fascial union (conjoined fascia) and is not simply a result of the LA inserting into the skin.
The STC is formed at the fused height of the orbital septum and LA. This fusion can be as low as the lower anterior portion of the tarsus near the lid margin. In the Asian single eyelid, the point of fusion of the orbital septum to the LA is typically below the superior tarsal border, while fusion occurs above the superior tarsal border in whites (see Fig. 4 ). , A pretarsal fat pad is also identified in the Asian single eyelid. Because of these anatomic differences, in the Asian eye the STC is smaller or is entirely absent and creates an impression of a fuller and thicker eyelid.
The eyelid consists of 5 main layers (superficial to deep). , In order to surgically create an STC, a component of the anterior lamella (skin and OOM) must be fixated to an element of the posterior lamella (LA). , Asian double eyelid surgery removes the factors (descending preaponeurotic fat pad, pretarsal fat) that prevent the bonding between the 2 lamellas, as well as creates adhesion between them , ( Fig. 6 ).
Preoperative consultation for blepharoplasty
The preoperative consultation begins with a thorough assessment and documentation of the patient’s eye condition, including whether
- •
The eyes and eyebrows are left to right symmetric
- •
The eyes are of equal size
- •
The power to open the eyes the same
- •
One eye is more protruded than the other
- •
There is a difference in the degree of skin sagging
The most common sources of lid asymmetry include the following :
- •
A difference in brow position
- •
Inequality of globe exposure
- •
Orbital position posture
- •
Lateral canthus posture
- •
Lower lid posture
Brow and eyelid asymmetry is common in patients being evaluated for upper eyelid blepharoplasty. Because there is a high likelihood that asymmetric eyes will have asymmetric STC after blepharoplasty, the patient should be made aware of the preexisting eye and facial asymmetry beforehand. Preoperative counseling includes discussions about the anatomic limitations imposed by their periorbital tissues and expected surgical results.
The next step is to determine the patient’s desired height for the double eyelid crease. The level and shape of the planned eyelid fold should be individualized and discussed with each patient. Teenage patients usually request a lower, more subtle double eyelid crease. As they get older, they generally want a larger double eyelid.
The peak level of growth in the vertical dimension of the palpebral fissure is reached between ages 10 and 13 years, that of the intercanthal distance between ages 14 and 16 years, and that of the horizontal dimension of the palpebral fissure between ages 17 and 19 years. Therefore, for teenage patients, a nonincisional method is recommended first, reserving the option of having a higher crease created with the incisional method later, if desired. If a patient’s skin is thick, the eye-to-eyebrow distance is close, or the eye size is small, a small crease looks more natural than a high crease. However, if the patient’s skin is thin and the eye size is large, the STC height can be tailored to the patient’s desire. In the case of single eyelids, oftentimes the eyes will have a swollen appearance. Whether this is due to the fat or the thickness of the skin itself, or a combination, should be identified.
The importance of eyebrow position in Asian upper blepharoplasty
It is extremely important to check the brow position during the initial evaluation. Postoperative crease asymmetry is a common source of dissatisfaction after double eyelid surgery, occurring in 13% to 35% of Asian blepharoplasties. Eyebrow asymmetry is one of the common causes. It is not unusual for even youthful East Asians to experience a sudden drop in their eyebrow position after upper blepharoplasty, owing to a phenomenon known as compensated brow ptosis. Compensated brow ptosis is a prevalent condition whereby, preoperatively, the patient’s eyebrow resting level is so ptotic and low that it interferes with forward vision, especially laterally. To compensate, the patient subconsciously forces their frontalis muscles into constant contraction, to alleviate the obstructed view. , Following double eyelid surgery, the forehead muscles are no longer required to maintain their contraction to aid with vision, and consequently, the eyebrows drop. In such cases, the distance between the eyes and the eyebrows reduces, and the eyes may not look fresh after surgery. , Therefore, when compensated brow ptosis is recognized during a consultation, the relationship between eyebrow change and double eyelid should be explained to the patient.
If there is eyebrow asymmetry, an endoscopic brow lift is recommended first. If not performed together, the double eyelid incision line must be designed a little higher, or additional skin and OOM should be excised, in order to prevent double eyelid asymmetry following surgery.
In young Asians, an endoscopic brow lift is performed for natural double eyelids, not for antiaging purposes. It is very beneficial to those with profoundly low resting eyebrow levels with significant frontalis activated compensated brow ptosis. If the distance between the eyes and eyebrows is narrow, the creation of double eyelids will appear unnatural. However, if the eye-to-eyebrow distance is increased by performing an endoscopic brow lift, it is then possible to create a fresher and more pleasing STC. To evaluate for this preoperatively, lift the eyebrows by hand. If by doing so the hidden double eyelids are exposed and their size and shape are also good, an endoscopic brow lift alone may be sufficient without the need for double eyelid surgery ( Fig. 7 ).