Anatomy and standards of beauty are different between Asians and Westerners. Unlike Westerners, Asians have a wide and prominent jaw shape but prefer a slim and soft face shape. To achieve this goal, maxillary setback and/or posterior impaction surgeries are popular among upper jaw surgery, and various adjuvant surgeries are performed simultaneously on the mandible to obtain the so-called oval shape or V-line face. In addition, according to the development of virtual surgery software and orthodontic treatment techniques, the surgery-first approach is now accepted as a reliable option for orthognathic surgery if it is indicated.
Key points
- •
Asian women prefer to have slimmer and softer faces compared with white women.
- •
The Le Fort I and bilateral sagittal split osteotomy short lingual techniques are the most popular surgical techniques.
- •
Diverse adjuvant jaw surgeries, such as malarplasty, lateral corticotomy, mandibular angle reduction, and genioplasty, are performed commonly during orthognathic surgery.
- •
The surgery-first approach is now accepted (recognized) as a reliable option for orthognathic surgery.
- •
The use of cutting-edge technologies has become popular for more precise and safer orthognathic surgery.
Introduction
Orthognathic surgery (OGS) for jaw deformities has seen a leap since Hullien first introduced jaw deformity surgeries back in 1849 and has recently become a safe and effective surgical method that improves the functional and esthetic aspects of the patient. Over the last century, the technical developments in jaw deformity surgery could be categorized into the development of various effective mandible and maxillary surgery methods, the development of orthodontic treatment methods before and after surgery, and the development of surgical materials and devices. In this article, the latest trends in OGS currently being performed in Asia, especially in Korea, are detailed, with a focus on the unique features that differ among Western patients.
Different factors of Asian and westerners for orthognathic surgery
The standards of beauty are quite subjective and are influenced greatly by culture. In general, Western women think that an angular and distinct jaw shape is attractive, whereas Asian women prefer a small, slim, and soft face shape, which is more feminine. In addition, the shape of the jaw itself differs between Westerners and Asians. Westerners have characteristics such as a narrow and long face, a high nose, a prominent tip of the chin, and relatively less protrusion of the maxilla and cheekbones. In contrast, Asians have a relatively wide face, a low nose, and a more protrusive maxilla and cheekbone. One of the main purposes of jaw-correction surgery is to improve esthetics that the patients prefer. Therefore, to achieve this goal, the surgical plan and surgical method selected differ significantly from those in the West.
Characteristics of surgery planning in Asians
In general, Asian women prefer a slim and smooth mandibular angle and jawline. With respect to the maxilla, they prefer it not to be too protrusive, an approximately 90° nasolabial angle, so that a low nose could be compensated. Regarding the chin, the preferences are that it should not be too big, but somewhat prominent. Overall, they wish to have the so-called oval or V-shaped face. Therefore, during OGS in Asia, additional jaw plastic surgeries, such as mandibular contouring surgery, malarplasty (of the cheekbone), mandibular angle reduction, and various types of genioplasty, are often conducted simultaneously.
However, repositioning the jawbone only for esthetic purposes can cause serious jaw dysfunctions, such as difficulties in chewing and opening the mouth, sensory loss, relapse of jaw deformities, and even fatal side effects, so functional aspects of the jaw after OGS should be considered during surgical planning. To this end, the role of preoperative orthodontic treatment is important, and the ideal surgical planning of OGS is to consult (collaborate) with an orthodontist and a surgeon from the beginning to establish an adequate preoperative orthodontic treatment plan considering the final location of the jawbones.
Diagnosis
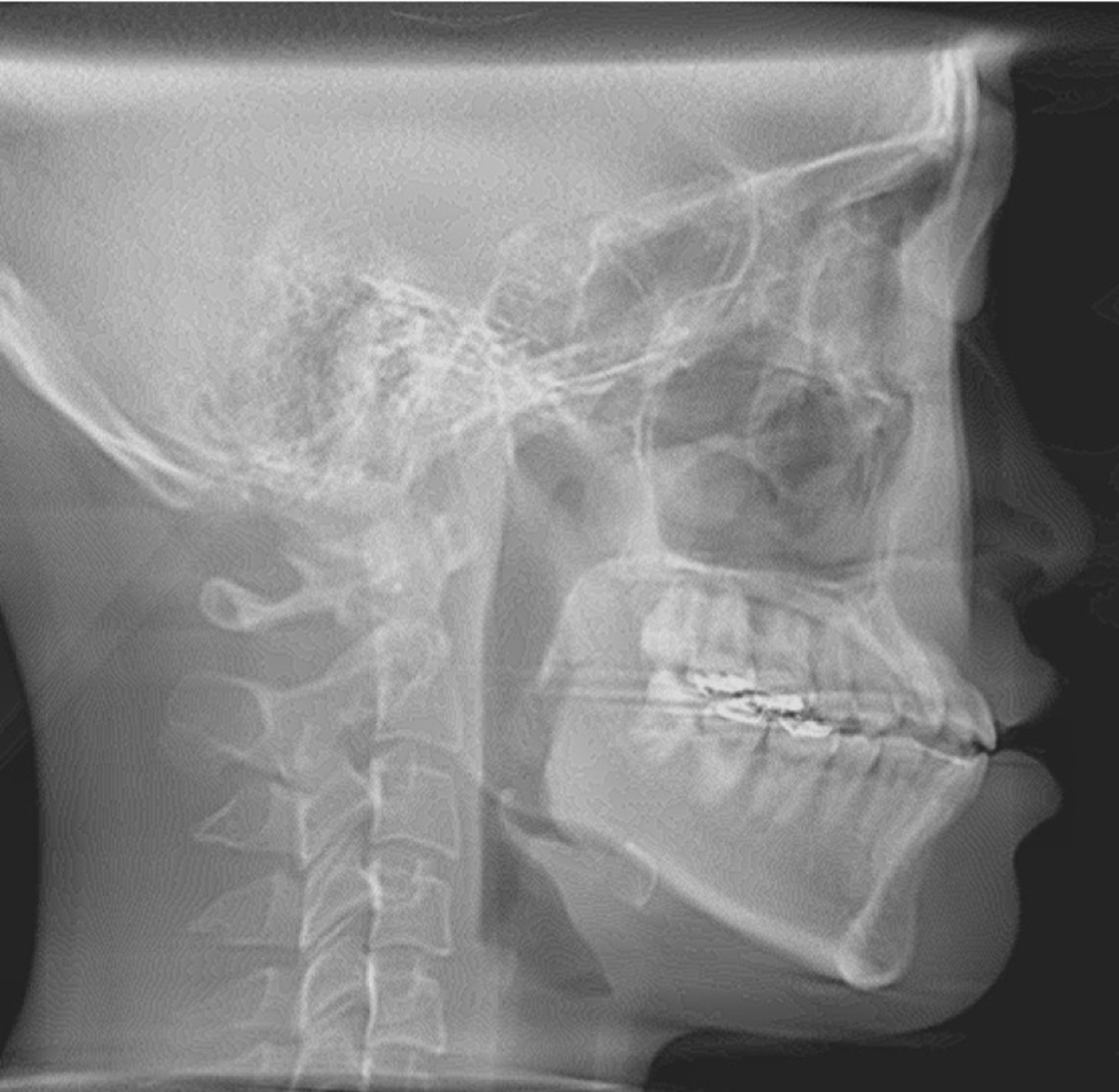
The lateral cephalogram is the method used most commonly to analyze the malocclusion. Anatomic landmarks are identified, and linear and angular measurements are used to analyze the patient’s malocclusion ( Fig. 1 ). The measurement values are compared with the norm, and the amount of deviation for each variable identifies the type of malocclusion. A list of commonly used skeletal, dental, and soft tissue lateral cephalometric variables and the Korean norm are shown in Table 1 . In patients with facial asymmetry, a posteroanterior cephalogram or computed tomography (CT) is recommended to analyze the asymmetry.
| Variable | Definition | Norm |
|---|---|---|
| SNA (°) | Angle formed by sella, nasion, and point A | 82.4 |
| SNB (°) | Angle formed by sella, nasion, and point B | 77 |
| ANB difference (°) | Difference between SNA and SNB | 3 |
| A to N-Perp (mm) | Distance from Nasion-perpendicular line to point A | 0 |
| Pog to N-Perp (mm) | Distance from Nasion-perpendicular line to pogonion | −5 |
| Wits (mm) | Distance between the points drawn from point A and point B perpendicular to the occlusal plane | −1.3 |
| APDI (°) | Anteroposterior dysplasia indicator | 81.4 |
| SN-GoGn (°) | Angle formed by the sella-nasion plane and the mandibular plane | 32.5 |
| Occlusal plane (°) | Angle formed by the FH plane and the occlusal plane | 10 |
| ODI (°) | Overbite depth indicator | 70 |
| U1-FH (°) | Angle formed by the maxillary incisor long axis and the FH plane | 116 |
| IMPA (°) | Angle formed by the mandibular incisor long axis and the mandibular plane | 95 |
| Upper lip to E-line (mm) | Distance from the outermost point of the upper lip to the E-line (pronasal to soft tissue pogonion) | 1.8 |
| Lower lip to E-line (mm) | Distance from the outermost point of the lower lip to the E-line | 3.6 |
Case
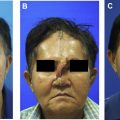
A 19-year-old female patient presented with the chief complaint of jaw protrusion and facial asymmetry. On a clinical examination, a midface deficiency with chin protrusion was observed ( Fig. 2 ). According to the intraoral photographs, an edge-to-edge bite with anterior open bite tendency was observed ( Fig. 3 ). Both the left and the right first molars showed a class III relationship, and the lower dental midline was deviated 2.5 mm to the right from the facial midline. In her smile photograph, a flat smile arc was observed.


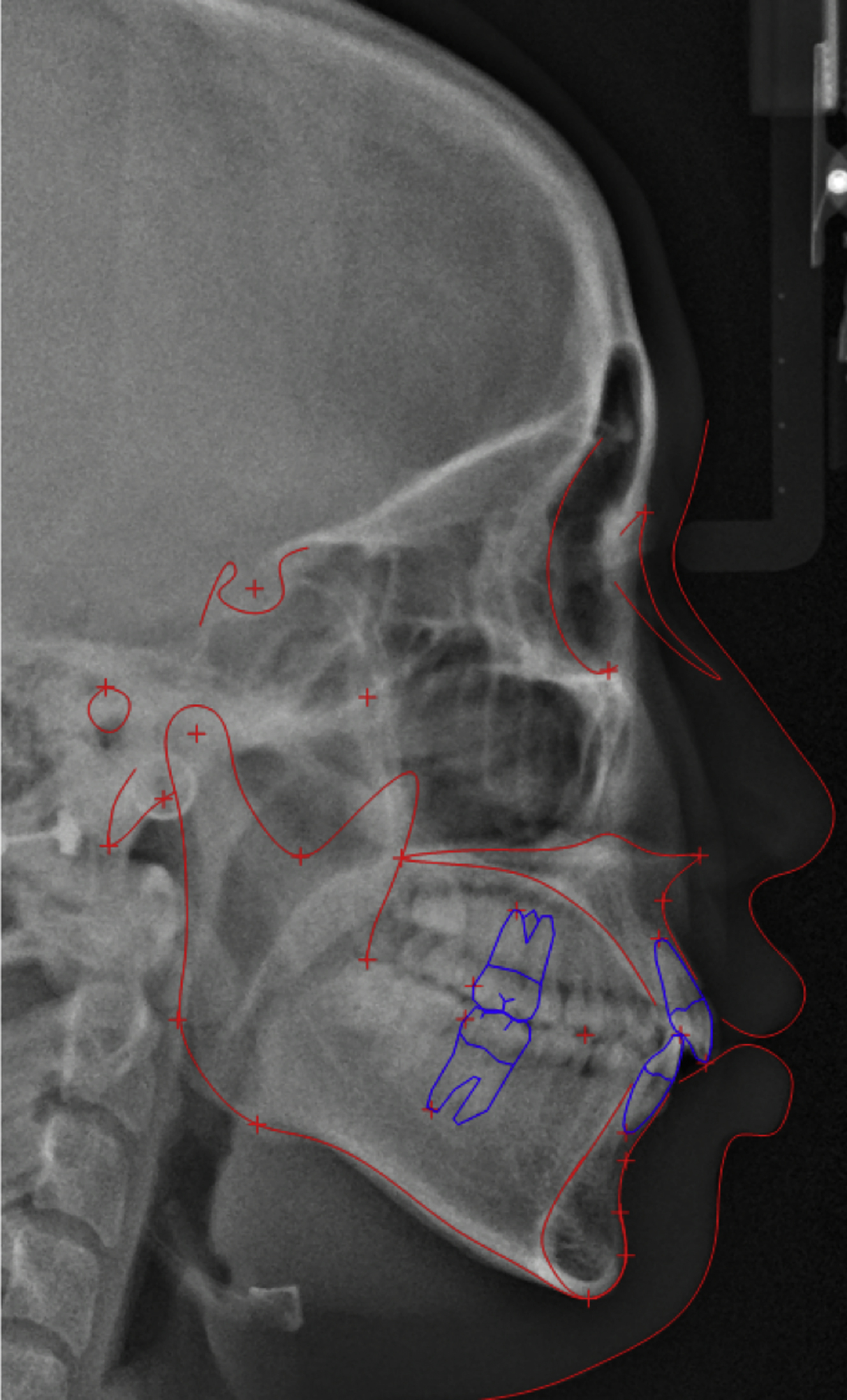
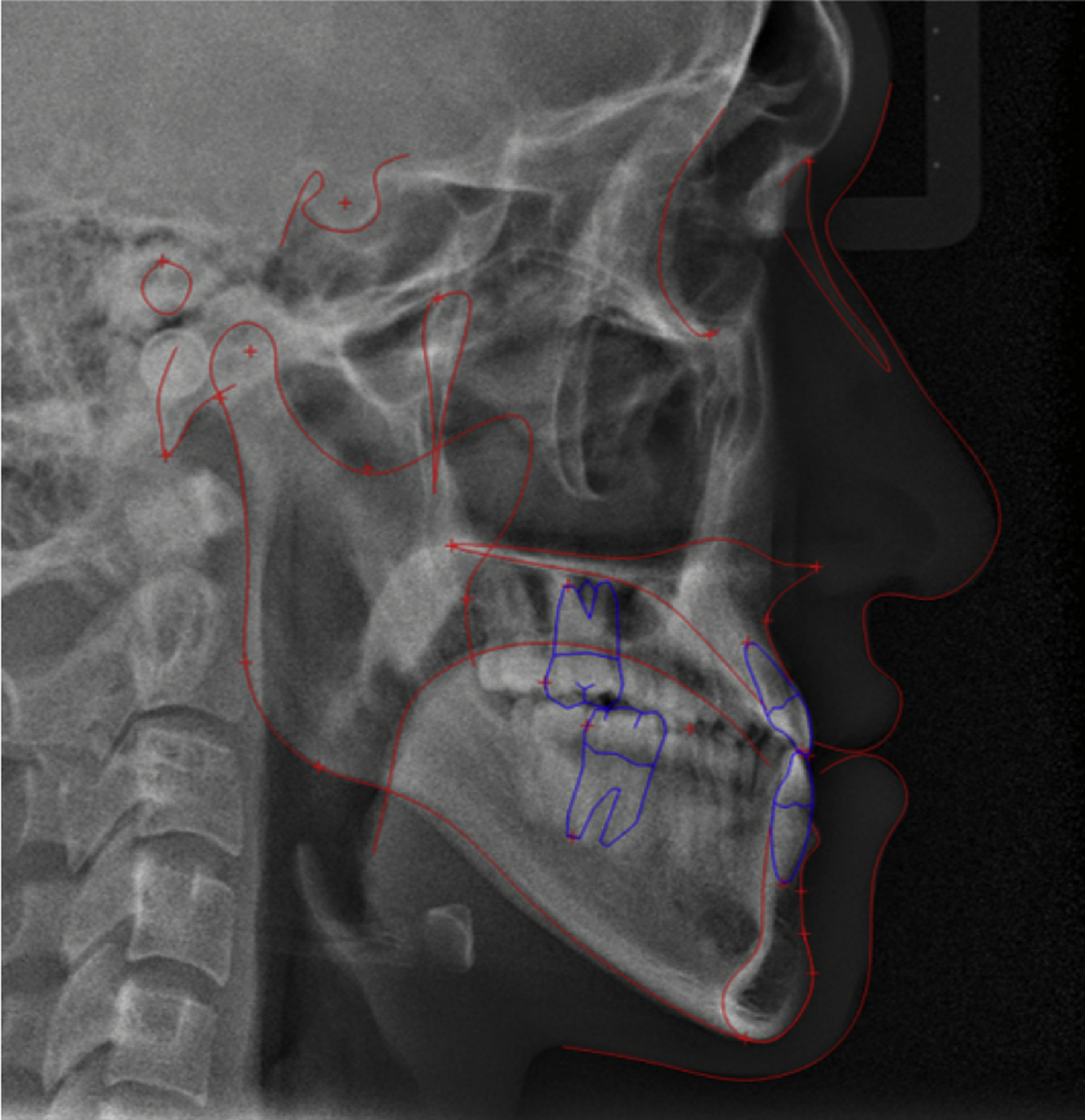
The lateral cephalometric analysis revealed a class III skeletal pattern with an point A-nasion-point B angle of −2.7°, and Wits appraisal of −7.7 mm. mandibular plane angle (angle between sella-nasion and gonion-gnathion) was 42.7°, indicating a long face. The upper incisors were proclined with a upper incisor inclination (U1-FH) of 132.4°. The lower incisor inclination was 92.4°, measured relative to the mandibular plane ( Fig. 4 , Table 2 ).
| Measurements | Norm | Initial |
|---|---|---|
| SNA (°) | 82.4 | 78.3 |
| SNB (°) | 77 | 81.1 |
| ANB (°) | 3 | −2.7 |
| A to N-Perp (mm) | 0 | 0.4 |
| Pog to N-Perp (mm) | −5 | 4.8 |
| Wits (mm) | −1.3 | −7.7 |
| APDI | 81.4 | 90.9 |
| SN-GoGn (°) | 32.5 | 42.7 |
| Occlusal plane (°) | 10 | 3.7 |
| ODI | 70 | 46.5 |
| U1-FH (°) | 116 | 132.4 |
| IMPA (°) | 95 | 92.4 |
| Upper lip to E-line (mm) | 1.8 | −2.0 |
| Lower lip to E-line (mm) | 3.6 | 2.8 |
According to the cone beam computed tomography (CBCT) images, a maxillary transverse deficiency was observed.
Treatment goal
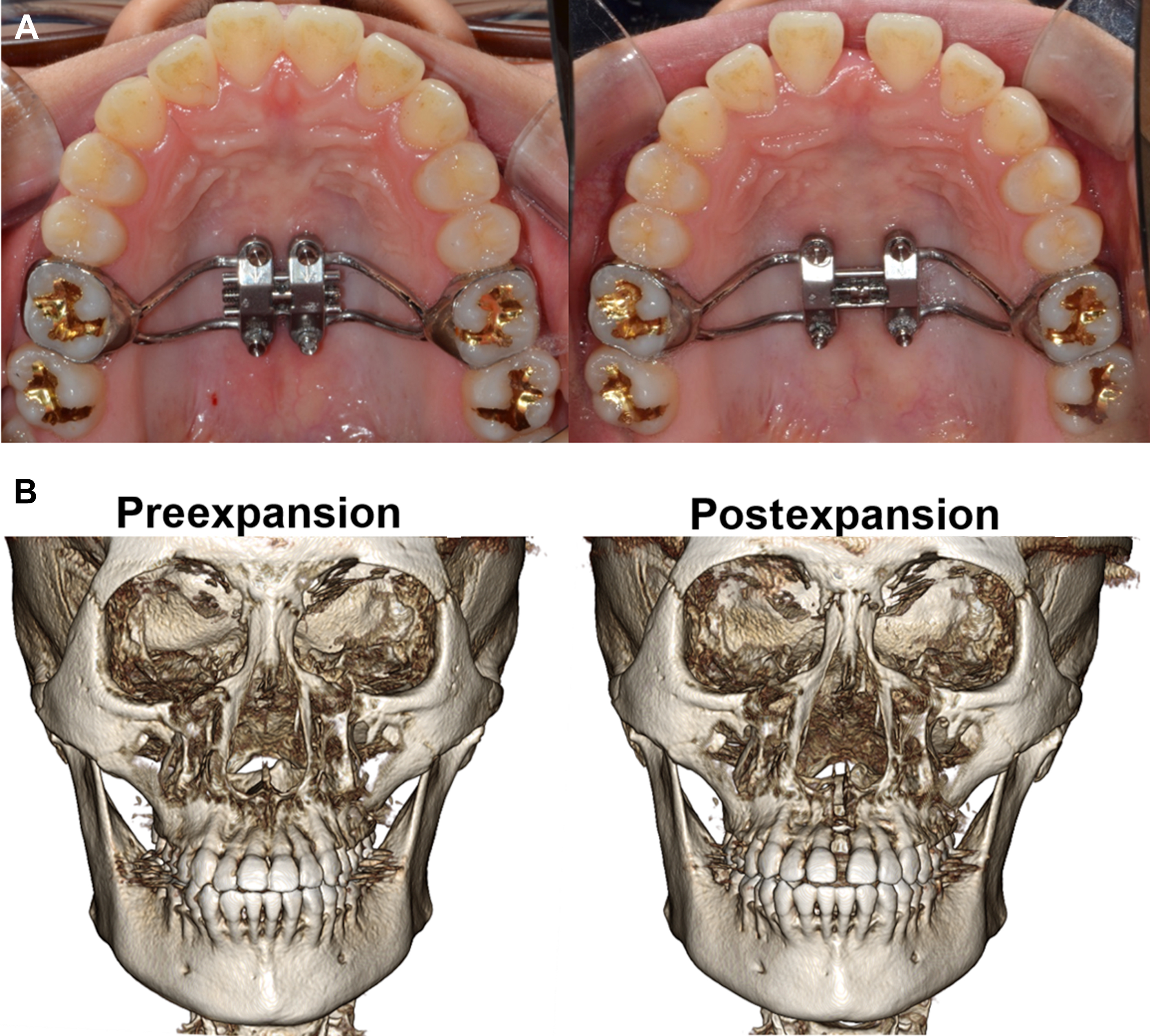
The treatment goal was to correct the facial asymmetry and mandibular protrusion and obtain normal occlusion. Maxillary transverse deficiency is often observed in patients with skeletal class III malocclusion. In adult patients, maxillary skeletal expansion can be performed by surgically assisted rapid palatal expansion (SARPE) or miniscrew-assisted rapid palatal expansion (MARPE). In SARPE, corticotomy of the maxilla along the Le Fort I osteotomy line is performed, followed by maxillary expansion using an expansion screw. MARPE uses temporary anchorage devices or miniscrews that are anchored to the midpalatal suture, and then the maxilla is expanded using an expansion screw ( Fig. 5 ). Maxillary expansion is an unstable procedure because of the thick keratinized palatal mucosa; therefore, overcorrection and long-term retention are required.
Treatment plan
Before the surgery, usually presurgical orthodontics is performed. As the teeth are often compensated to the patients’ skeletal pattern, a process of decompensation is done to accommodate the postsurgical occlusion. In the case of class III malocclusion, upper and lower incisors often exhibit proclination and retroclination, respectively, to compensate for the skeletal discrepancy ( Fig. 6 ). In patients who have severe crowding with upper incisor protrusion, the upper bicuspids could be extracted to relieve crowding and retract the incisors. Lately, the surgery-first approach (SFA) has increased because of advantages, such as the immediate improvement of facial esthetics, patients’ psychosocial status, shorter treatment time, and physiologic tooth movement. Despite the advantages of the SFA, care should be taken owing to the unstable occlusion after surgery. There are greater vertical and sagittal changes in the occlusion during postsurgical orthodontics, making it less predictable for the final skeletal relationship. In addition, premature contact in the postsurgical occlusion might lead to surgical relapse, and possibly to TMD because of condylar displacement. Therefore, to obtain predictable results in the SFA, accurate diagnosis and treatment planning, accurate laboratory procedures, and much clinical experience are required.
Surgical planning
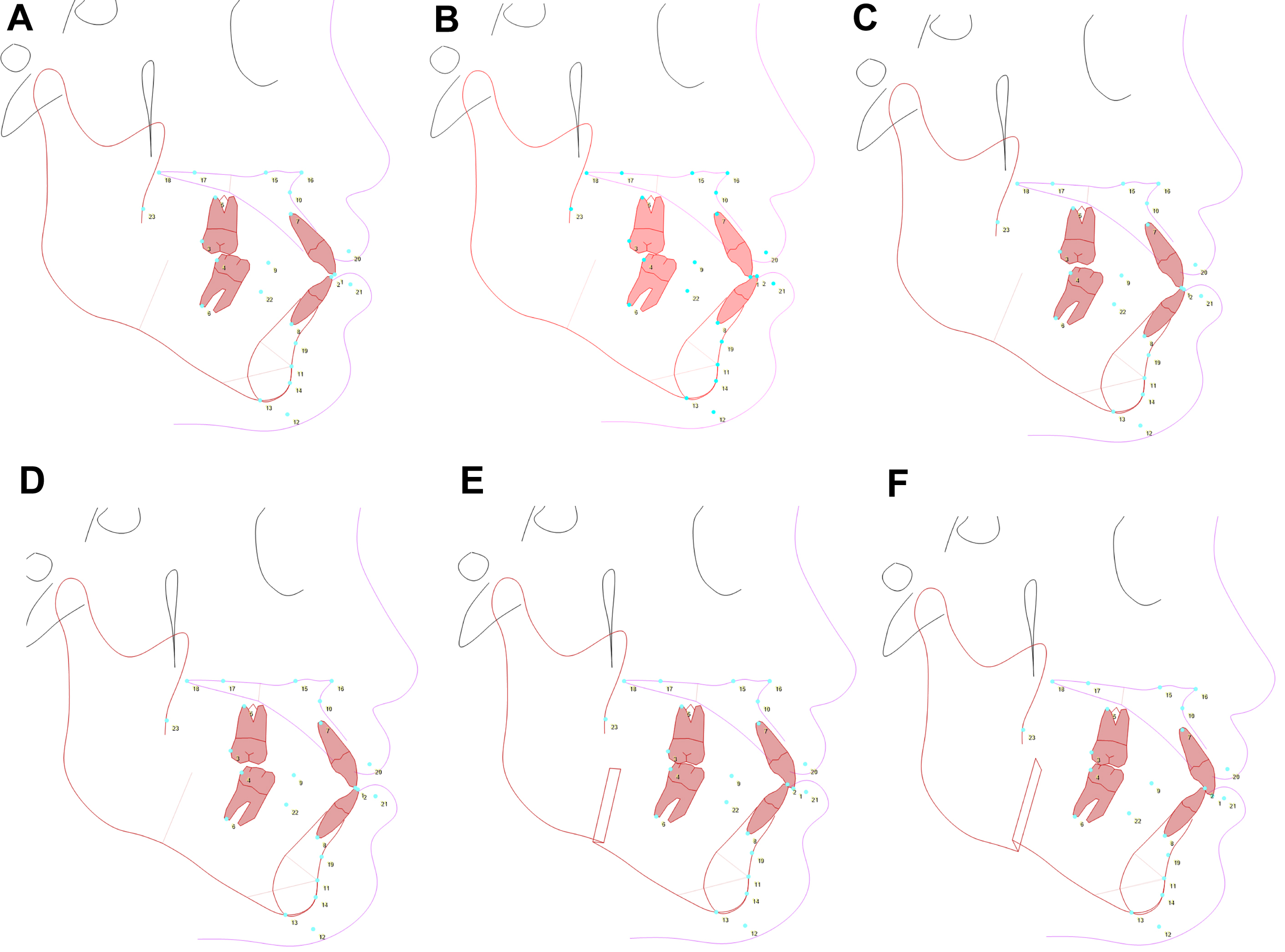
Patients expect an esthetic outcome in addition to the correction of their malocclusion. Therefore, the treatment plan should be based on a careful assessment of the facial soft tissues in addition to analyzing the skeletal and dental anomalies. Arnett and colleagues suggested 7 steps for OGS planning using lateral cephalograms, as follows ( Fig. 7 ):
- 1.
Correct the torque of the maxillary incisors (see Fig. 7 A and B).
The patient had proclined upper incisors; therefore, the upper incisor torque was corrected.
- 2.
Correct the torque of the mandibular incisors.
The patient had lower incisor torque within normal ranges; therefore, no changes in the lower incisors were planned.
- 3.
Position the maxillary incisor (Le Fort I).
The maxilla was moved up and forward (see Fig. 7 C).
- 4.
Autorotate the mandible to 3 mm of overbite.
After maxillary repositioning, the mandible was autorotated to occlude with the upper teeth (see Fig. 7 D).
- 5.
Move the mandible to 3 mm of overjet.
The mandible was set back to obtain a normal incisor overjet (see Fig. 7 E).
- 6.
Set the maxillary occlusal plane.
The patient had a flat occlusal plane; therefore, posterior impaction was performed, resulting in the clockwise rotation of the maxillomandibular complex. This resolves the mandibular protrusion (see Fig. 7 F).
- 7.
Assess chin projection and height.
The patient shows normal chin projection with an improved facial profile.