Over the past 27 years, the endoscopic foreheadplasty has evolved into the procedure of choice for aesthetic surgeons with a goal of rejuvenating the brow-forehead complex. Harmony between brow position, symmetry, and improvement of forehead and glabella wrinkles can be achieved if the surgeon possesses a thorough understanding of the endoscopic techniques, regional neurovascular, muscular, and soft tissue anatomy. Since first introduced in 1985, endoscopic foreheadplasty has been refined by more precise methods of dissection, allowing natural long-term results. Herein we discuss the basic surgical technique of endoscopic foreheadplasty and highlight important details necessary for surgical success.
History
Correction of brow asymmetry and softening of forehead rhytids has been attempted for nearly 100 years. The first known description of what is now known as foreheadplasty was done by Passot in 1919 . This description involved various horizontal skin excisions on the higher portion of the forehead in hopes of improving horizontal rhytids. Soon thereafter, Passot’s work was expanded by Hunt in 1926 and Claoue in 1933, both describing variations to the original technique. All the original accounts revolved around soft tissue excision in hopes of correcting wrinkling. In 1964, Castanares expanded traditional techniques of simple soft tissue excisions and recommended modification of the frontalis muscles and transection of the frontal branch of the facial nerve in an attempt to improve aesthetic outcome. For the next 30 years, various surgeons expanded upon this technique, giving rise to the biplanar approach and modification of the procerus and depressor supercilii muscles. In 1989, Keller introduced minimally invasive endoscopic laser procedures for brow, midface, and neck procedures . In 1992, Isse introduced a minimally invasive instrumental technique for foreheadplasty utilizing endoscopic equipment . Since that time, the endoscopic method of rejuvenation has evolved into the procedure of choice for many aesthetic surgeons.
Personal Philosophy
The soft tissues of the brow-forehead complex are constantly molded by the downward forces of gravity and depressor muscles along with the opposing action of the elevator muscle units. With time, this opposition results in volume loss, weakening of ligamentous structures, and general descent of tissues. For this reason, it is no longer sufficient to perform a “simple blepharoplasty,” but instead to rejuvenate the entire periocular area. As one can expect, every aspect of foreheadplasty cannot be covered in a single chapter, or even a single textbook. However, in the following pages an outline of endoscopic foreheadplasty will be presented along with important details with respect to patient care, endoscopic equipment, and surgical anatomy.
Anatomy
Understanding the anatomy of the forehead and brow is essential to performing an endoscopic foreheadplasty. The eyebrow can be divided into three parts: medial, central, and lateral. The medial aspect of the eyebrow lies medial to the supraorbital nerve. Naturally, the medial limit of the central eyebrow is the supraorbital nerve; the lateral limit is the superior temporal crest. Lastly, the lateral third of the eyebrow is found lateral to the superior temporal crest. All subunits of the eyebrow are controlled by a delicate interaction between depressor and elevator muscle activity. These two muscle groups, along with the corrugators, make up all human facial expression around the brow.
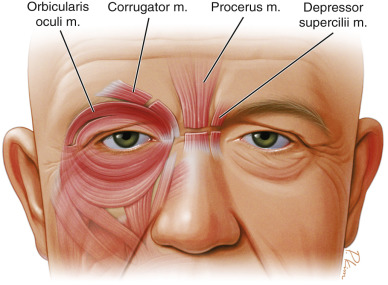
The frontalis muscle is the main elevator of the eyebrow. Its interaction with associated depressor muscle activity is responsible for the horizontal rhytids seen on the forehead. The orbital portion of the orbicularis oculi muscle is the main depressor of the eyebrow and responsible for horizontal lines adjacent to the orbit. The depressor supercilii and procerus muscles depress the head of the medial brow and produce the “reverse parenthesis” and horizontal rhytids at the root of the nose. Finally, the corrugator supercilii muscle produces both an elevation of the medial brow along with depression of the lateral brow ( Fig. 8.1 ). In 1852, Duchenne described an agonist/antagonist relationship of the muscles acting on the brow with the orbicularis, corrugator, procerus, and depressor muscles functioning to depress the brow and the frontalis muscle functioning to elevate the brow. This complex muscle action is responsible for flattening of the glabellar area and forehead wrinkles . With appropriate understanding of eyebrow anatomy, endoscopic foreheadplasty has the ability to modify all of these muscles as needed.
Preoperative Assessment
Endoscopic foreheadplasty is indicated when improvement of the brow position and shape is desired, or when the rhytids of the forehead, glabella, and periorbital areas need to be softened. Generally, patients must be well adjusted with a desire to restore a more youthful appearance rather than achieve a “perfect” look. The following conditions are indications for an endoscopic foreheadplasty and should be considered during the preoperative evaluation:
- •
Brow ptosis and malposition
- •
Glabellar rhytids (frown lines)
- •
Tissue sagging (root of nose)
- •
Pseudoptosis of upper eyelids
- •
Mild to moderate dermatochalasia (upper eyelids)
- •
Minimal ptosis of the upper eyelids
- •
Downward slanting of the lateral canthus
- •
Periorbital wrinkles (crow’s feet)
Instrumentation
Aside from a complete set of endoscopic equipment (including a medical video camera, camera control unit, light source, and fiber optic cable), very little specialized equipment is required to perform endoscopic foreheadplasty. One curved periosteal elevator, a straight elevator, scissors (curved and straight), and a 30-degree endoscope with open dissection sheath is the extent of necessary equipment. While there is some variability in endoscope and camera quality, the overall ability to perform the surgery does not depend on these variables. Suction-Bovie cautery and plasma knife instruments can offer some benefit to dissection and when obtaining hemostasis.
Surgical Technique
A combination of intravenous sedation and local anesthesia is adequate, although general anesthesia can be used. Local anesthesia is performed using 1.0% lidocaine with epinephrine (1 : 100,000) for the forehead, temporal area, eyelids, and scalp infiltration.
The following standard surgical steps are performed during an endoscopic foreheadplasty:
- •
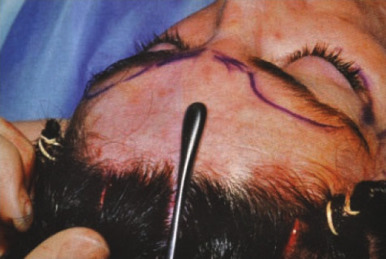
Preoperative marking
- •
Incisions
- •
Creation of an optical cavity
- •
Dissection of the forehead and temporal areas
- •
Release of tissue attachment to bone and deep fascia
- •
Tissue modifications
- •
Fixation
The Incisions
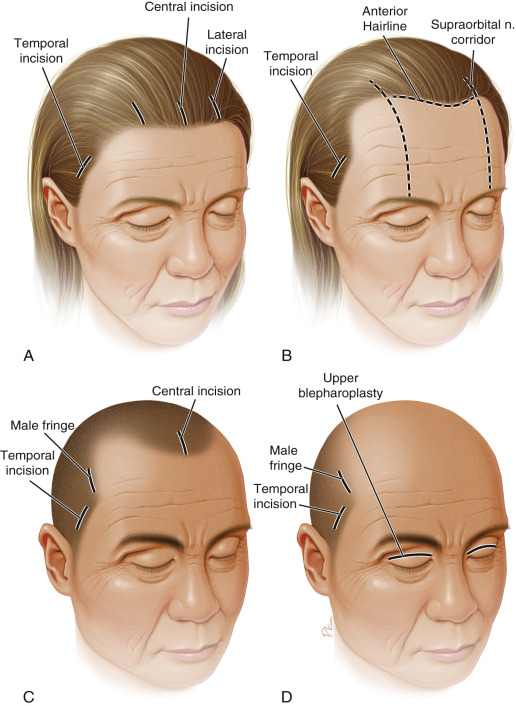
Following a rigid template for incision placement is not possible for endoscopic foreheadplasty. The placement of incisions must reflect surgical goals. Once the aesthetic outcome of the operation is clear, incision placement can be easily detailed. A vertical midline incision placed immediately behind the hairline and taken through the frontalis and periosteum is used in most patients. Vertical incisions are then placed approximately 5 cm on either side of the midline incisions, the aptly named paramedian incisions. These incisions are carried down to, but not through, the fascia overlying the frontalis muscle. The paramedian incisions should be performed with care. The deep division of the supraorbital nerve passes close to these, below the orbicularis . Traditional incision length was limited to 1 to 2 cm. However, a longer incision allows for improved visualization and reduces hair loss in the immediate vicinity of the incision. For these reasons, incisions up to 3 cm in length are now regularly used.
Male patients offer unique challenges to incision placement. Hair loss following the Norwood I to III classifications can be navigated quite well with the median incision in the midfrontal area with temporal incisions placed either in the midtemporal area or at the temporal fringe. For more severe balding (Norwood IV–V), most work can be accomplished through low lateral incisions made on the temporal fringe . At times, a midline blepharoplasty incision can be used for retrograde dissection ( Fig. 8.2 ).
Creation of the Frontal Cavity
In order to utilize endoscopic techniques for foreheadplasty, an optical cavity must first be created. These cavities can be created in a subcutaneous, subgaleal, or subperiosteal plane. Of the listed techniques for frontal brow dissection, most aesthetic surgeons employ a subperiosteal plane, which will be the only technique discussed here in detail. After incisions have been placed, a 2-cm arc of blunt dissection is drawn over along the entire length of the brow. Blind dissection is avoided beyond this area in order to avoid injuring nerves emerging from the neural foramina near the orbital rim. The initial dissection is blind and easily accomplished with a curved endoscopic elevator ( Fig. 8.3 ). This initial dissection is paramount for protection of the supraorbital nerve and lateral supraorbital nerve branches emerging from the bony orbital rim. Once the optical cavity is created, the endoscope can be advanced through the incisions and will provide a magnified view of the dissection cavity. With the help of the endoscope, midline dissection is carried to the origin of the corrugators. At this point the surgeon will then enter a midline subgaleal plane over the nose, successfully preserving the attachments of the midline corrugators and associated ligaments. Lateral dissection is taken to, but not beyond, the level of the arcus marginalis.