History
The brow has historically been overlooked in the rejuvenation of the aging face. The focal procedure of facial rejuvenation has always been the rhytidectomy. Surgical forehead rejuvenation began at the turn of the 20th century . Passot has been generally recognized as a pioneer in the field. Several other surgeons described their work over the subsequent years . The interest in these procedures waned, as the effects were often found to be transitory. However, as with most plastic surgery procedures, interest in brow rejuvenation was renewed in the latter half of the 20th century, when new techniques evolved and results improved .
There has been, and continues to be, significant controversy as to the “correct” technique to rejuvenate the brow; for example, whether to use an open versus an endoscopic approach, and currently, in some quarters, whether the brow can be adequately elevated with nonsurgical techniques such as Botox and fillers. The contention that one operation is superior to the other has left many surgeons unsure of the appropriate approach. This confusion has contributed to the subjugation of the browlift to the less controversial rhytidectomy and blepharoplasty procedures, and thus avoidance of addressing the aging brow in lieu of correcting the aging face and periorbital regions.
Historically all brow rejuvenation procedures were performed via the open technique. Although this procedure has excellent long-term results, patients and surgeons were often hesitant to undergo such an involved procedure with extensive incisions and recovery time. With the advent of the endoscopic techniques in the early 1990s, surgical rejuvenation of the upper third of the face became increasingly popular . This trend, coupled with the advent of noninvasive paralytic agents, brought brow rejuvenation to the forefront of facial rejuvenation.
Personal Philosophy
Comprehensive facial rejuvenation merits an appraisal of all components of the face. This is especially pertinent for the upper third of the face. This is the focal region of the face during communication with others. The importance of the periorbital area is seen in everyday life. Indeed, it is so common in our observations of others that it is often overlooked. When speaking to or meeting someone for the first time, attention is immediately brought to the periorbital area, much more so than the jowls or the neck that so bother the aging patient. Patients with brow ptosis subconsciously raise their brows when viewing themselves in the mirror. This cannot be done on the ptotic, sagging tissue of the middle and lower thirds of the face. Thus the patient masks an issue that others see at all times. Although simple, this is an often-overlooked point that must be discussed with the patient.
The importance of brow rejuvenation is vital to facial rejuvenation. In our practice, this procedure is often seen as the primary operation to rejuvenate the face. In addition, if middle- and lower-third rejuvenation is performed without addressing the brow, the patient may be left with an overall disharmonious appearance .
The primary reason for brow rejuvenation in our practice is to address the patient’s concern about looking heavy, tired, or angry, especially in the glabellar area. The goals of any browlifting procedure are to eradicate the depressing effect of the musculature of the glabellar region and to raise the lateral aspects of the brow. A key benefit of the open approach is the excellent exposure, which allows for precise handling of these problems. There is no need for overcorrection with the open approach because the surgeon can be confident that the results will be long lasting. This is owing to excision, rather than suspension, of the ptotic tissues.
There have been concerns over the side effect profile of open browlift techniques. Likewise, endoscopic techniques are being questioned as to the quality and longevity of the results. Despite the variety of methods to surgically, or nonsurgically, address this area, it often remains neglected.
The endoscopic techniques have done a tremendous amount to reinvigorate interest in the aging upper third of the face. Surgeons have noted the advantages of smaller incisions: less downtime; reduced scarring, numbness, and alopecia; and minimizing the loss of blood . However, endoscopic techniques do have selected disadvantages. For example, there is still no method of fixation that is clearly superior to others . The technique has a limited ability to correct severe eyebrow ptosis and must be utilized only in certain patients . In addition, the endoscopic record is not yet defined . Reports in the literature have confirmed many surgeons’ trepidations about this technique. Only 50% of plastic surgeons surveyed felt that their results were satisfactory more than 2 years after the operation .
In addition to the longevity concerns regarding endoscopic browlifts, there have also been questions regarding its impact on the contour of the brow . It has been found that the greatest impact of the endoscopic browlift is medially not laterally, thus contributing to the dreaded “surprised look” and not affecting the lateral brow where the lift is generally desired . This highlights another advantage of the open browlift technique. The open approach allows for more control of the brow contour by way of its differential scalp incision . Although emphasis has been on endoscopic and less invasive methods such as the use of botulinum toxin A and various fillers, the open browlift has a proven record of providing excellent, lasting results with minimal side effects. The open browlift maximizes the optimal removal of the corrugators and excess skin that accumulates with time . In addition to the traditional coronal and tricophytic approaches, the temporal, or lateral, browlift is a modification of the open approach by focusing the incision placement in a vector that optimizes the aesthetic ideal of lateral brow elevation with no raising of the medial aspect of the brow . This approach is also quite useful when coupling the procedure with a vertical facelift in that it allows for removal of the troubling redundancy of tissue incurred at the superior, anterior aspect of the facelift incision.
In our opinion, the main role for the endoscopic approach is in young patients with a minimal amount of ptosis. In our practice, however, we often suggest deferring the procedure in younger patients until the concerns have truly manifested themselves, at which point we perform what we believe to be the procedure of choice, the open browlift. We feel the open browlift is the optimal operation in patients with severe ptosis of the brows, deep glabellar or midforehead wrinkles, or a preexisting high forehead, when a trichophytic lift is selected. The results achieved with this forehead lift are predictable, natural appearing, long lasting, and aesthetically pleasing with minimal morbidity .
Other surgeons have also reported that the open technique is more effective in achieving the three main goals of brow surgery: brow elevation, reduction of transverse lines, and reduction of glabellar lines . We would add to this the enhanced ability to contour an asymmetric brow and the aforementioned elimination of excess tissue in the temple region that is often found after a vertical facelift. Even those who favor the endoscopic technique state that some patients will benefit from the open approach .
The negative side effects of open browlift techniques seem to have been unduly emphasized in the literature. In an unpublished report on the significance of the side effects of the open browlift techniques, the authors found an overwhelming percentage of patients who would recommend the procedure to a friend or relative. Studies have also thrown light on various vague detractions of the open technique. The difference in the rate of alopecia between the two techniques is small, and sensory loss has been noted to be higher with endoscopic techniques . In summary, the open browlift technique has a similar complication rate, a comparable rate of sensory loss, and a higher patient satisfaction rate compared with endoscopic techniques .
The other issue commonly mentioned when discussing the open approach to forehead rejuvenation is the extent of the incision. We feel that this is predominantly a matter of proper patient education and surgical technique. In our practices it is rare for patients to opt out of this approach after a thorough conversation on the benefits of the procedure. Certainly, if patients feel that they are going to be “scalped,” they will not consent to the procedure .
The coronal incision can be completely camouflaged with the patient’s hair. In the case of the trichophytic incision, only the anterior aspect is exposed, and this component of the incision can also be masked with hair when the patient wears her bangs combed forward. In both instances the incision generally heals imperceptibly when proper beveling is employed during the incision and meticulous technique is applied during the closure. The patient must be counseled as to the amount of time it requires for the wound to heal completely. If the patient does not wish to have an open procedure because of the incision, the endoscopic approach should be explored with the patient.
The open technique via the pretrichial route enables the surgeon to manipulate certain situations in unique ways. For example, the pretrichial lift allows for shortening of an elongated forehead. A long forehead disrupts the harmony of the face and adds to the patient’s age . The forehead-shortening capabilities of the trichophytic browlift are unobtainable with the endoscopic technique . Detractors argue that the incision placement prohibits the use of this technique, but many feel that with proper planning, technique, and execution this approach yields an excellent aesthetic result . This is not to say that this procedure may be used in all patients with an elongated forehead. If the patient is overly self-conscious of scarring or has a hairstyle that positions the hair posteriorly, the surgeon would be wise to avoid this technique.
The decision-making process for the coronal versus the pretrichial approach has been reported in the literature . We generally agree with these parameters but do make exceptions in certain cases to the 5-cm rule.
The purpose of this chapter is not to determine which technique is superior. That is a decision to be made during the consultation. The open browlift technique should be familiar to all plastic surgeons rejuvenating the upper third of the face. Endoscopic and open techniques should be discussed with all patients. Finally, endoscopic and open browlift techniques do not address volume changes that occur in the brow and temple regions because of bony remodeling and fat atrophy. Volume loss has to be addressed with fillers or autologous fat grafting and will be discussed elsewhere in this book.
Anatomy
To appropriately rejuvenate the brow, the surgeon must be knowledgeable of its anatomy. The position and movement of the brow are determined by several factors. First among these are the paired frontalis muscles. The frontalis is the sole elevator of the brow. These paired muscles have a definitive midline separation ( Fig. 7.1 ) . Each of these muscles originates from the galea aponeurotica. This fascia also encases the muscles, and inserts into the orbicularis oculi muscles, which then insert into the eyebrow dermis. Only the lower 20% of the frontalis muscle is mobile .
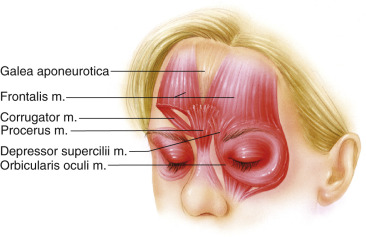
The brow has four depressor muscles: the procerus, corrugator, depressor supercilii, and the orbital portion of the orbicularis oculi (see Fig. 7.1 ). The depressor supercilii is located on the medial arc of the orbicularis and is considered by some to be part of the orbicularis . This muscle aids the corrugator in depressing the medial head of the brow. The corrugator musculature originates from the frontal bone near the superomedial orbital rim and inserts into the dermis of the forehead skin behind and immediately superior to the middle third of the brow . Contraction of the corrugator complex results in depression of the brow and deep vertical glabellar rhytids. The procerus originates from the nasal bone and inserts into the lower medial skin of the forehead. Its contraction leads to the most inferior horizontal rhytid over the radix of the nose .
The galea is contiguous with the superficial temporalis fascia laterally. The periosteum of the frontal bone is contiguous with the temporalis fascia. These respective fascia layers converge just medial to the temporal fusion line of the skull.
The sensory innervation to the scalp is relatively straightforward. The two major nerves are the supraorbital and supratrochlear, with the supraorbital nerve supplying the majority of the scalp. The supraorbital nerve has two main divisions, superficial (medial) and deep (lateral) . The deep division of the supraorbital nerve runs under the deep galeal plane and over the periosteum toward the superior temporal line before taking a turn superficially through the galeal fat pad on its way to the skin of the frontoparietal scalp . The superficial division courses from the orbital rim and over the frontalis muscle, and terminates in the anterior scalp . The superficial branch supplies the sensation to the forehead skin and anterior scalp. The superficial branches of the supraorbital nerve and the supratrochlear nerve both travel over the superficial surface of the frontalis muscle. The frontal branch of the facial nerve runs within the superficial temporalis fascia on its way to innervate the frontalis muscle.
Preoperative Assessment
Numerous studies have considered the ideal appearance of the female eyebrow . A variety of factors determine the aesthetically pleasing brow. An individual’s ethnicity, age, sex, culture, and adjacent structures all influence the perceived beauty of the brow. Although opinions differ on certain facets of the brow, certain desirable traits commonly recur: (1) the medial brow should lie at, or below, the level of the supraorbital rim; (2) the brow should have an apex lateral slant; (3) the medial brow should begin in the vertical plane of the inner canthus and lateral extent of the ala; (4) the brow should end laterally in line with a tangent drawn from the lateral ala through the lateral canthus; (5) the brow should be full and supple with minimal show of the orbital bone architecture and atrophy of the temple; and (6) the apex of the brow should lie above either the lateral limbus or lateral canthus . Another key feature of brow beauty is the relationship to the dorsal line of the nose ( Fig. 7.2 ). When the brow continues this gentle slope (brow-tip aesthetic line), it adds to the inherent attractiveness of the face .

The decision of trichophytic, temporal (lateral) versus coronal incision will be discussed with the patient during the preoperative assessment. This decision process begins with the patient’s desired appearance. This equation must take into consideration any inherent asymmetries as well as the patient’s desired contour. Again, this stresses the flexibility of the open approach. This judgment is based on the position of the hairline, low versus high, and the manner in which the patient wears his or her hair . Of course, the personal preferences of the patient must also be taken into account.
The key to an accurate preoperative assessment is the relaxation, manual if necessary, of the brow. It is in repose that the patient must objectively view the resting position of the brow. As mentioned earlier, the patient reflexively raises his or her brow when placed in front of a mirror or when a photo is taken. The surgeon can manually position the brow as it appears at rest with the patient’s eyes closed and then instruct her to open her eyes slowly. This maneuver enlightens the patient as to the issues at hand and furthers confidence in the surgeon as an expert who truly sees the face in a different manner from the layman. In addition, if the procedure is being coupled with a facelift the surgeon should note that the brow elevation may be necessary to “complete” the rejuvenation. In today’s aesthetic field the “natural” look is sought by nearly all of our patients. In addition, although it may seem counterintuitive to the patient, adding another procedure will actually assist in attaining the natural look by keeping the face harmonious.
Technique
The sequence of procedures for facial rejuvenation usually begins with the forehead lift. We rarely perform a solitary procedure on the brow. Most often it is in conjunction with an upper and lower lid blepharoplasty and deep plane facelift. We choose to do the brow first because it allows for a more conservative, and accurate, upper lid blepharoplasty. In select cases, such as patients with deep-set eyes, previous blepharoplasty, or limited redundancy of upper lid skin, the browlift is all that is needed for upper-third facial rejuvenation.
Marking and shaving of hair can be performed prior to or after the administration of the anesthetic. Patients are often very anxious during this time, and the marking and shaving of hair amplifies these feelings. We prefer to do these tasks after the administration of intravenous anesthesia.
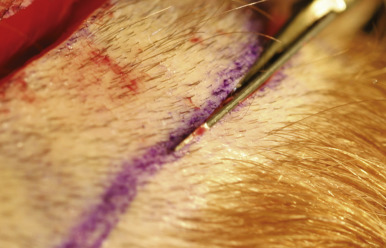
When a coronal approach has been chosen, a fusiform segment of tissue is shaved and marked for excision ( Fig. 7.3 ). The patient is evaluated in the preoperative area while sitting upright. Measurements are made of the brow elevation at three points: medial, central and lateral brow. It is common to elevate the lateral brow to a much higher extent than the medial brow. These measurements will be used as a guide in the operating room as to the exact amount of tissue to be excised. The surgeon should add anywhere from 3 to 5 mm of measured elevation to the amount to be excised when accounting for the patient’s own tissue mobility and exact location of the planned incision. The markings for the excision should lie 4 to 5 cm posterior to the anterior hairline. The lateral extent of the incision should terminate approximately 1 to 2 cm above the superior insertion of the auricle to the skull in an attempt to incorporate the superficial temporal vessel within the flap ( Fig. 7.4 ). If this vessel is compromised, however, the blood supply to this flap is substantial. The surgeon should ensure that an adequate amount of temporal hair is left behind. This is particularly important when this procedure is being performed in conjunction with a facelift in which a portion of the sideburn is shaved as well. The incision should parallel the anterior hairline tapering to a point at the lateral aspects. We prefer to mark and excise the amount of tissue to be removed at the beginning of the case rather than making one incision, anterior or posterior, mobilizing the scalp, and then deciding on the appropriate amount to excise. We have found we can reliably gauge the amount to be resected by assessing the mobility of the scalp and its associated effect on brow position prior to incision. It is acceptable to decide on the exact amount of skin to be excised after raising the flap. However, we have found that precise incising of this thick tissue, as is mandated when trying to preserve as many hair follicles as possible, is very challenging after it has been mobilized. With adequate experience the surgeon is highly successful in anticipating the total skin excision prior to the initial incision. Generally speaking, the amount of skin lies between 1 and 2 cm. If the surgeon discovers that he or she has miscalculated and resected too much tissue, the posterior scalp elevation can be performed to aid in the closure. Obviously it is better to err on the side of caution and remove less excess skin if the surgeon is uncertain as to the exact amount to be removed.


The trichophytic incision is more difficult to plan and perform but yields a tremendous result when attention is paid to the details. The marking begins with a trimming, with scissors, of the first two to three rows of hair in the anterior aspect of the hairline. Laterally the hair is shaved as an elongated, curved triangle with its apex above the superior insertion of the auricle to the scalp ( Fig. 7.5 ). This area is generally 4 to 5 cm in length and should not be placed too inferiorly to avoid encroaching on the temporal hairline. This termination point varies from patient to patient depending on the position of the hairline and the contour of the patient’s skull. Once the incision is created a flap must be mobilized to allow access to the glabellar musculature. This procedure often requires folding the flap upon itself, and thus an adequate rotation point must be chosen laterally. In the midline, the incision has gentle undulations closely following the hairline. This undulation allows improved camouflage of the incision over a simple straight line. The posterior aspect of the incision should be placed in the transition zone between the thick posterior hair of the scalp and the fine hairs that constitute the anterior hairline (see Fig. 7.5 ).

The hair is secured with rubber bands anteriorly. In the trichophytic browlift the only hair that is secured with rubber bands is the lateral temporal hair. The hair is shaved in the fusiform ellipse in the coronal approach and as described in the previous paragraph for the tricophytic approach. The temporal, or lateral, browlift is a modification of the tricophytic lift. The incision mimics this approach laterally while omitting the medial, and more visible, aspects of the incision. This approach is highly individualized and the amount of tissue marked is uniquely dependent on the patient’s specific desires and anatomy. Figure 7.6 is a more aggressive application of this technique.

The incisions are re-marked and injected with local anesthetic. We prefer a mixture of equal parts of 0.5% lidocaine with 1 : 200,000 epinephrine and 0.5% bupivacaine with 1 : 200,000 epinephrine. The injection should be in the galeal plane where most of the vessels run their course. Local anesthetic should also be injected into the subgaleal plane. Bilateral supraorbital and supratrochlear blocks are administered. Lastly, the corrugator and procerus muscles are directly injected to aid in pain management as well as for vasoconstrictive purposes. The patient is then prepped and draped in the standard fashion. We prefer to staple a sterile towel around the head in a parallel course to the planned incisions, being mindful not to place the towel too tightly.
The incisions are then performed with a No. 10 blade. We prefer this blade for its increased surface area, which reduces the need to change blades frequently. Excessive use of smaller blades leads to increased cost and operating time. The forehead skin is thick and will quickly dull smaller blades. The blade must be sharp and the surgeon should not hesitate to use several blades in making these incisions. A dull blade will cut imprecisely, which should never occur in cosmetic surgery. Proper beveling of both the pretrichial and coronal incisions is vital to attaining maximal hair regrowth and scar camouflage. In the coronal incision the bevel parallels the follicles throughout the length of the incision ( Fig. 7.7 ). The entire amount of shaved hair is removed, leaving a hair-to-hair closure. Thus the patient may be reassured preoperatively that he or she will not have a noticeable region of alopecia postoperatively. The coronal incision traces further laterally than the pretrichial incision, and the orientation of hair at the end point of the incision is almost perpendicular to the skin; the blade must mimic this orientation.