History
The signature operation of facial rejuvenation is the rhytidectomy. Of all the procedures designed to remedy the effects of aging, the rhytidectomy has the most profound ability to improve the patient’s appearance. The first recorded efforts to surgically rejuvenate the face appeared early in the 20th century . The first 50 years of the 20th century saw little advance; burdened by the risks of anesthesia and the lack of medications, such as antibiotics, surgeons were forced to move forward with great trepidation. As technologic advances erupted in the latter half of the 20th century, surgical advances soon followed. In the last 30 years of the century, these technologic advances enabled surgeons to provide excellent surgical results to their patients and the popularity of facial rejuvenation has since exploded. Facial rejuvenation surgery has never been more popular, as adjunctive modalities such as dermal fillers and Botox have brought interest in cosmetic improvements to an all-time high. Today, an attractive outward appearance is a sign of strength and health instead of vanity .
The original techniques employed short skin flaps and minimal, if any, manipulation of the underlying soft tissues for fear of damaging the facial nerve. With greater anatomic understanding, the techniques progressed deeper into the ptotic tissues of the aging face. The skin flaps gradually became longer and the manipulations of the underlying soft tissue, the superficial musculoaponeurotic system (SMAS), became more aggressive. With these advances, new frontiers were crossed and new complications arose. In addition, physicians working in this field have now gained a much greater knowledge and appreciation for other factors that historically had been neglected, especially in regard to lifestyle choices, such as smoking and alcohol intake, and in medications, such as antiplatelet agents.
The field has undergone a fascinating 40-year evolution since the groundbreaking work of Dr. Skoog in the 1970s . Skoog was the first to perform what can be called the deep plane technique. Hamra advanced the concept to include the soft tissues of the midface with his deep plane and composite techniques . Today, there is great controversy as to the appropriate technique and plane of dissection for optimal rejuvenation . With the advent of the deep plane facelift technique, rhytidectomy took a quantum leap forward. For decades, rhytidectomy provided the patient with a benefit that often pleased the patient but left the surgeon wanting more. This exciting technique enabled the surgeon to provide a more lasting, natural result. We propose our techniques described herein not as an answer to these dilemmas but as a proven method to safe, excellent, reproducible results in facial rejuvenation.
Personal Philosophy
The evolution of our technique is based on several criteria. First, the result with the deep plane technique was superior to that of the SMAS lift plication and imbrication techniques. With a more thorough undermining of the ptotic soft tissues of the face, a better postoperative result soon followed, as would be expected. Although the SMAS procedure is excellent for short-term gains in reducing skin laxity and mild improvement of soft tissue ptosis, the majority of the ptotic soft tissue remains fallen. We agree with the previously published viewpoint that “minilifts” or subcutaneous facelift procedures have only dealt with laxity of the skin and do not completely address the ptotic soft tissues of the face .
Second, once experience was gained with this technique, the long-term results became evident. In addition, the occurrence of the “pulled” or “operated look” decreased rapidly with the increased use of this technique. We also believe that with the shorter skin flap and superior blood supply of the deep plane technique, the catastrophic issues of skin loss and poor scar appearance are greatly diminished. With its strict adherence to physiologically sound principles, the effect of the deep plane technique is maintained for a longer period than that of the skin flap techniques. This is due to the composite flap maintaining the viscoelastic properties of the SMAS . Though others have not agreed with these opinions, we maintain our results have improved greatly since the transformation of techniques .
Much excitement has been generated over the “weekend” or “mini-facelifts.” With the promise of smaller incisions and less downtime, these procedures have received significant attention over the last several years as the popularity of plastic surgery has flourished. These techniques are similar to standard SMAS facelifts and thus are an option for certain patients.
Generally speaking, patients for whom these procedures are devised suffer from lax skin, especially in the lower face. When a patient considers facial cosmetic surgery, we feel the first operation should be the definitive procedure. If the patient has had a “less invasive” procedure in the past, the tissue planes are forever altered, thus making further surgery, when the aging process has come to fruition, much more difficult. This is obviously a matter of personal preference, and some patients will persist in having certain procedures performed regardless of the surgeon’s preferences. This is a matter for each individual practice. For ours, all primary facelifts are done via the deep plane techniques.
A variety of midfacial approaches have been proposed over the last 20 years. The point of origin for most of these procedures is from the work of Tessier . Several variations of this approach have been proposed . We favor the deep plane technique over the subperiosteal midface approach for several reasons. The first is the direct nature in which the deep plane technique addresses the fallen tissue. The focus of midfacial rejuvenation is the suspension of the soft tissues of the midface that have fallen with time. In the deep plane technique, the surgeon may directly manipulate this tissue to the desired location. To state the issue directly, deep plane surgery “works at the level at which mobility and aging laxity are occurring” . The tissue to be repositioned in the midface is the cheek fat that rests on the zygomaticus musculature. With elevating the soft tissues off the zygomatic musculature, the surgeon may now address the nasolabial fold and the descent of the soft tissues in a manner not possible before. A SMAS correction is inherently more effective than a subperiosteal approach in the midcheek because it is closer to the tissue to be repositioned .
In addition, the nerves that innervate the facial musculature enter from below. Thus, it stands to reason that dissection techniques that leave the nervous structures between the plane of dissection and the target tissue leave the nerves at risk from either direct trauma through inadvertent movements of the dissector or, more commonly, through traction neuropraxia. The subperiosteal technique has been reported to have a high rate of facial nerve injuries, implying a steep learning curve .
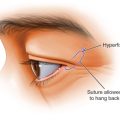
Edema from periosteal manipulations is significant, and for it to persist for weeks, if not months, is not uncommon . To patients who are expecting a “minimally invasive” procedure, this may prove to be a difficult issue. In the subperiosteal approach, the zygomaticus musculature is repositioned to a place it never was before, the intermalar distance is necessarily increased, and frequently manipulation of the lateral canthus is required . Not only is the lateral canthus often altered, but the resetting of the zygomaticus musculature may also lead to an unwanted alteration of the patient’s appearance . One must be concerned about the potential for distortion of the palpebral fissure with many of these procedures . When an open lower lid blepharoplasty approach is incorporated into the subperiosteal midfacial techniques, the lower lid malposition rate has been reported to be as high as 50% .
An argument can be made for addressing the midfacial region via volume rather than surgical manipulation. Whether it be autologous fat injection or dermal fillers, volume replenishment is almost always employed as an adjunct to surgical elevation to create the optimized outcome. The surgeon, to attain the desired result, must be fully versed in not just surgical handling of ptotic tissues but also in the key role that volume plays in facial rejuvenation .
Our approach to facelifting, as with our overall practice approach, is the attainment of a natural, lasting result via conservative means. We seek to provide the patient with rejuvenation where the observer cannot detect that an operation has occurred. The deep plane technique may not be considered conservative in some quarters, but with the technique performed as described herein, we feel it to be exceedingly safe and well tolerated by the patient.
Anatomy
The facelift surgeon must be fully versed in the complex anatomy of the face. A complete discussion of the anatomic relationships is beyond the scope of this chapter and the reader is advised to refer to excellent published reports on this challenging territory . There are several anatomic keys to the aging face, and specific areas of concern are discussed. As we age, some of the most profound effects are noted in the midface. A key to the deep plane technique is the anatomy of the midcheek and malar region.
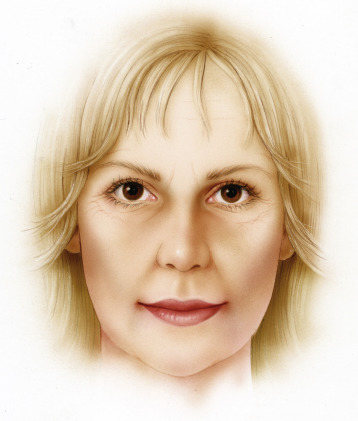
The cheek mass descends with age and causes a deepened nasolabial fold inferiorly while creating a depression at the infraorbital rim ( Fig. 16.1 ) . The malar fat pad atrophies and descends with age, leading to a cresent-shaped hollowness at the lid-cheek interface and nasojugal groove, and lack of cheek prominence, giving a sunken, tired appearance . The effects of gravity are more pronounced on superficial tissues .


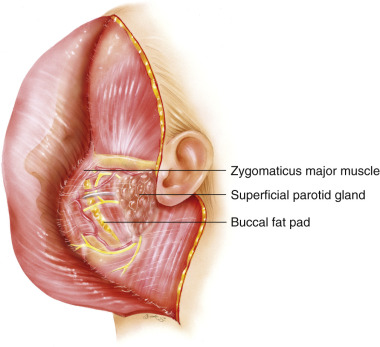
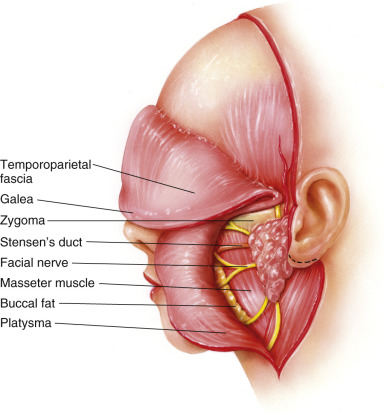
Another feature of midfacial aging is the buccal fat pad. It provides fullness to the cheek in youth and diminishes, relatively, in size as the patient ages . This fat pad has four major components, with the buccal being the largest. On the lateral aspect of the masseter lies this parotid-masseteric fascia, a key structure in the deep plane technique. This fascia layer is found between the overlying SMAS and the underlying branches of the facial nerve ( Figs. 16.2 and 16.3 ). Fortunately, this fascia binds the branches of the facial nerve down, a key factor when placing extreme traction on the SMAS to expose the deep plane. As this fascia continues anteriorly, it shifts superiorly to envelop the buccal fat pad, parotid duct, and buccal branches of the facial nerve .
Another important area of the midface is the nasolabial fold . The nasolabial fold is a true anatomic boundary between the fatty cheek above and the upper lip below . As the tissues of the midface become ptotic with age, the nasolabial fold deepens and becomes of greater concern to the patient.
The lower aspect of the face is dominated by jowling and submental fat. The jowling that so troubles the aging population results from the descent of the platysma muscle in the neck and face with the associated fat and skin along the mandibular line. The platysma has been described as having a graded aging process . The history of submental fat resection is often attributed to the work of Millard and others .
The SMAS merits specific discussion. First described by Mitz and Peyronie, the SMAS layer and manipulations thereof have intrigued facial plastic surgeons for 40 years . This layer has been seen as an extension of the platysma into the face (see Figs. 16.2 and 16.3 ). The SMAS is considered to be a fibromuscular structure that lies in continuity with the platysma and has no bony attachments . The layer consists of connective tissue and muscle. It has fibrous extensions that connect it to the skin . The SMAS is thicker in its lateral aspect over the parotid and tapers as it travels medially . Our experience concurs with these reports. There has also been controversy over the relationship of the SMAS to the parotid fascia as to whether they are separate layers or one and the same . Whether they are one and the same or distinct layers means little to the surgeon. The key point is that there is a fascia layer to be raised in this region and its thickness varies from patient to patient.
The SMAS is noted to be muscular in its inferior component where the platysma rises into the face and more fibrous as the surgeon goes further cephalad as the platysma tapers. In the more muscular, inferior portion of the SMAS, facial nerve branches are commonly seen traversing the masseter muscle on the floor of the dissection as the deep plane is raised (see Figs. 16.2 and 16.3 ).
Also of note during our dissection technique are the retaining ligaments of the face. The key ligaments for our procedure are the zygomatic ligament and the masseteric ligaments . The zygomatic ligament may be released as the dissection proceeds to the origin of the zygomaticus major at the anterior aspect of the zygomatic arch. Care should be taken in this area, as it is closely associated with the facial nerve. On occasion, the releasing of these ligaments is performed in the subcutaneous plane instead of underneath the fascia when augmentation of the zygomatic arch is desired. The masseteric ligaments pose a challenge for the surgeon in that they closely resemble peripheral branches of the facial nerve. When dissecting in the correct plane these ligaments may be safely released.
The vascularity of the deep plane technique is an important concept. Schuster and associates described three concentric vascular arcades . The most lateral arcade is drawn from the zygomatico-orbital and transverse facial arteries. The middle arcade consists of the infraorbital and facial artery connected by the middle and posterior jugal branches, and the medial arcade contains the angular artery, superior and inferior labial arteries, and a branch of the ophthalmic artery. When raising a skin flap in the SMAS or skin-only facelift, this outermost arcade is traumatized as a random flap is created. As this flap is developed, blood must pass through a choke zone as it traverses one arcade to another. The further medial this dissection is carried, the more tenuous the blood supply becomes as the blood must now pass through two choke zones. The deep plane technique avoids this vascular compromise.
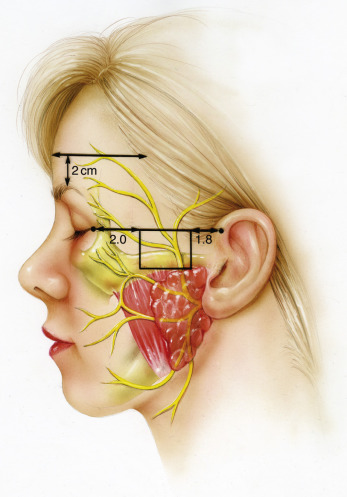
There is also great concern for the temporal branch and the marginal mandibular branch, due to their respective lack of anastomotic connections, during deep plane rhytidectomy . There are usually four rami of the nerve that cross the zygomatic arch, though this number varies, of course. The most anterior ramus is an average of 2.0 cm posterior to the anterior end of the zygomatic arch. The danger zone is located in a region overlying the zygomatic arch approximately 2.0 cm anterior to the superior attachment of the auricle and 2.0 cm posterior to the bony orbital rim. It is in this area that the nerve is just beneath the subcutaneous fat and directly overlying the bony prominence of the zygoma . When employing the deep plane technique, the surgeon must also be cognizant of the marginal mandibular branch anatomy. As the surgeon aggressively attempts to rid the patient of jowling with an anterior dissection in the lower face, he or she must note that the marginal branch is located deep to the platysma until approximately 2.0 cm lateral to the corner of the mouth. At this point, the nerve takes a more superficial trajectory along the undersurface of the facial mimetic muscles. The facial artery can also be used as a guide. Posterior to the vessels the nerve is generally not in the dissection; however, anterior to the vessels the surgeon must proceed with caution . The most commonly injured nerve in rhytidectomy is the greater auricular. This structure is located approximately 6.5 cm inferior to the bony auditory canal .
Preoperative Assessment
Prior to the analysis of the patient’s cosmetic desires and possibilities, a thorough history and physical examination must be performed. This is especially true for aesthetic surgery. As an elective procedure, there can be no excuse for an overlooked medical issue that can compromise the outcome. General issues that should be investigated include previous surgeries, medications, smoking, and alcohol intake, and any coexisting medical conditions. Specific issues to facial rejuvenation surgery such as the use of aspirin and other nonsteroidal anti-inflammatory medications, hypertension, and smoking history should be thoroughly explored and explained to the patient. In addition, there are several medical diseases the facial plastic surgeon must respect. Obviously, any blood dyscrasia must be evaluated with a hematologist. Also, several connective tissue disorders, such as Ehlers-Danlos syndrome, may compromise the result of an otherwise good operation.
Perhaps of equal importance in the preoperative assessment is the evaluation of the patient’s psyche by the surgeon. We make a point to ascertain the patient’s motivation for the proposed procedure(s). This is a highly individualized approach that each surgeon must discover for himself or herself. We cannot stress enough the importance of this evaluation and opportunity to educate the patient on realistic expectations. No matter what the technique nor how well it is executed, a psychologically impaired patient will not be pleased.
The surgeon should then evaluate the nature of the skin. Sun damage, smoking history, and Fitzpatrick type are but a few of the skin features that must be assessed during the preoperative consultation process. Fair skin with a moderate amount of sun damage usually heals best; darker skin types necessitate more caution on the part of the surgeon. The patient should be questioned as to his or her healing history and any preexisting medical conditions or medications that might hinder the healing process.
After the initial examination of the skin, we prefer to examine the overall appearance of the face. The patient’s ethnicity, body habitus, and age all play a role in this initial assessment. The general proportions of the face should be considered. The face is generally broken down into fifths vertically, based on the width of an eye; and thirds horizontally, as measured from the hairline to the glabella, from the glabella to the subnasale, and from the subnasale to the menton. Any facial asymmetries should be noted at this time. All faces have some level of asymmetry. This is normal and should be conveyed to the patient, preoperatively.
The surgeon should then proceed to examine the patient’s bony infrastructure. This is the scaffolding on which the soft tissues of the face are suspended. The malar prominence, mandible, and hyoid positions are all examined and palpated. A strong bony structure to the face is obviously the favorable situation.
The soft tissue components of the face are the final facet of the examination. Jowling, buccal fat, the sagging midface and nasolabial fold, infraorbital hollowness, and the aging neck are the focal points of the soft tissue examination. In the majority of cases the lifting of the surgical procedure is complemented by augmenting the soft tissues via autologous fat or commercially prepared fillers. The scope of this chapter is not to elaborate on these modalities, as they are described elsewhere in the book.
Surgical Technique
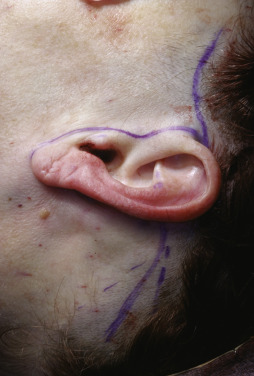
Nearly all of our deep plane facelifts are performed under intravenous sedation. Usually, these procedures are combined with a series of other facial rejuvenation procedures. After administration of the anesthetic, the patient is prepped. The first step in our preparation is a minor shaving of hair in the preauricular and postauricular areas. The preauricular area is shaved to enable the “bird’s beak” incision, which extends horizontally to the temporal hair tuft through the sideburn . The postauricular shaving is performed by noting the superior aspect of the conchal bowl and drawing a straight line in an inferoposterior vector from this point ( Fig. 16.4 ).
A thorough injection of local anesthetic (an equal mixture of 0.5% lidocaine with 1 : 200,000 epinephrine and 0.5% bupivacaine with 1 : 200,000 epinephrine) is then performed in the subdermal planes of dissection bilaterally. The surgeon should note the character of the skin and dermis during the injection, especially in revision procedures. When performed in conjunction with other procedures, the facelift is always performed last to ensure that a compressive dressing may be placed at the termination of the case. The face and neck are then prepped and draped in standard surgical fashion and the head is wrapped with a sterile towel and clamped.
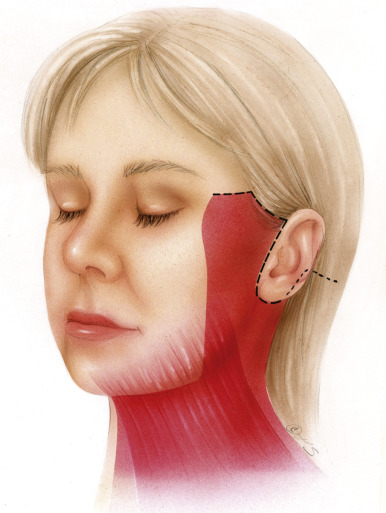
Our incision placement is dictated by the desire to preserve hair and create the optimal vectors for lifting the tissue in a natural manner. Thus, we choose to bring the anterior and superior aspect of the incision forward, through the sideburn hair with a gentle curve as it progresses anteriorly ( Fig. 16.5 ). Care is taken to maintain an adequate amount of sideburn hair that will grow over and thus mask the scar. In order to maintain a normal hair pattern, the preauricular tuft must not be advanced over the level of the supraauricular sulcus . By employing a frontotemporal hairline incision, the surgeon may place the vector of lift more superiorly than lateral. It is not a pure vector but we feel it minimizes untoward sequelae . We agree with others that the classic incision beginning at the superior attachment of the auricle and tracing superior and posterior inherently shifts the hair in an unnatural fashion and can be a stigma of facelift surgery .

The postauricular incision is marked by bisecting the superior aspect of the shaved hair, as noted from the superior conchal bowl vector, to the inferior aspect of the native hairline. The preauricular incision is marked horizontally from the temporal hair tuft, through the sideburn, now shaved, to the bird’s beak above the ear. The incision then traverses inferiorly in a native preauricular crease until the tragus is encountered. The selection of a pretragal or retrotragal incision is based on the patient’s desire and anatomy. Either approach when carefully planned and executed results in an excellent result. For the retrotragal incision, a sharp demarcation is made into the external auditory canal and behind the tragus. Emerging from the inferior aspect of the tragus, the incision now emerges at a near 90-degree angle to the tragus until a natural preauricular crease is encountered, where the incision will make another 90-degree turn inferiorly as it tracks along the preauricular crease. The incision then gradually wraps around the lobular attachment and slightly onto the posterior aspect of the conchal bowl as it rises to reach the posterior take off near the superior aspect of the conchal bowl ( Fig. 16.6 ). Occasionally the anterior aspect of the incision must be extended into the temple region when the surgeon anticipates that a significant amount of skin will be removed . This extension is commonly used in revision procedures and in older patients who have extremely lax skin with multiple fine rhytids.

The lengths of the anterior and posterior components of the incisions are dictated by the anticipated amount of skin mobilization and resection. The function of these incisions is primarily to manage the dog-ears that occur with the advancement of the flap. The lift is basically a posterior and anterior rotation flap with a central advancement component .
All incisions are made with a No. 10 blade, except the retrotragal aspect. We prefer the use of these larger blades because with their increased surface area the knife stays sharper for longer periods, an important factor when performing extensive incisions. The incision begins at the anterior/superior aspect and traverses the retrotragal portion, around the lobule, and onto the postauricular portion, where it terminates in the hairline. The initial portion of the incision, through the sideburn, should be performed with a beveled blade parallel to the follicles to ensure masking hair growth during the recovery period. The incision is beveled in accordance with accepted hair-saving principles . Further extension of this incision superiorly, along the hairline in patients with excess skin, should be performed without beveling as this will yield a better postoperative scar. Once the incisions have been performed, the skin is then elevated. The bird’s beak area is grasped with an Adson forceps and, using sharp, fine scissors, the skin elevation is begun. We prefer to use a transillumination technique to ensure proper depth of dissection. The plane of dissection is subdermal, just inferior to the hair follicles. With the transillumination technique, the assistant places the overhead lights onto the skin while the operative field has no direct light ( Fig. 16.7 ). This is in direct opposition to the commonly used technique of bright illumination from behind the surgeon’s head and onto the field. Once adequate skin has been raised, several different instruments can be used to retract the skin. A thimble with a double prong, a variety of rake retractors, and our preference, the Anderson bear claw, are all acceptable retractors. The skin elevation, as with almost all our dissection maneuvers, requires an excellent assistant to provide countertraction. Other technical aspects worthy of mention include the dissection over the sternocleidomastoid musculature. The fascia in this area can be very adherent, leading to injury of the great auricular nerve if care is not taken ( Fig. 16.8 ) . After discerning the plane, we change scissors from sharp tipped to dull. Many surgeons will perform a blunt dissection of the subdermal plane, which is definitely acceptable, but in this day and age of minimal downtimes and the need for expedient recoveries, we have found our technique to be less traumatic to the tissues and thus our postoperative edema is considerably less than if we employed the blunt dissection techniques.


The subdermal elevation is continued for approximately 4 to 5 cm from the incision points ( Figs. 16.9 and 16.10 ). This dissection may be carried slightly more anterior in the region of the malar eminence, where the dissection turns deeper as the deep plane is raised.

In the inferior aspect of the dissection, the subdermal plane is raised until the surgeon reaches the angle of the mandible. At this point, a lighted retractor is used to dissect the posterolateral portion of the platysma ( Fig. 16.11 ). The overhead lights used for transillumination are now removed from the field. The subdermal dissection should be relatively bloodless as long as adequate local anesthetic has been injected and sufficient time has transpired.
Once the edge of the platysma has been identified, the plane can be rapidly developed with broad spreading movements of the dissecting scissors. The preplatysma dissection may require the use of extra-long scissors to dissect to the midline. We try to lift all of the subdermal fat off the muscle, leaving a clean plane of muscle at the floor of the dissection.
We infrequently perform liposuction of the neck, though it is a viable option in select cases. We prefer direct excision of fat. We concur with other authors that liposuction can lead to several postoperative issues that are exceedingly difficult to remedy. As with many other issues in plastic surgery, it is best to underdo this portion of the procedure than to try to attain the “perfect” result, which can lead to drastic, difficult postoperative issues .
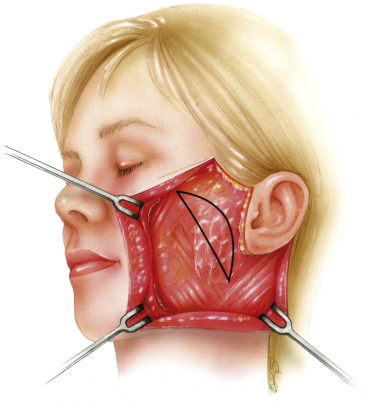
After completely elevating the skin and subcutaneous tissue from the platysma, the surgeon pays attention to the deep plane. We prefer to enter this plane 2 to 3 cm anterior and slightly superior to the angle of the mandible inferiorly ( Figs. 16.12 and 16.13 ). A line may be marked for the incision into the deep plane from just above the angle of the mandible to the junction of the zygomatic arch and body. This incision, as with all others in the deep plane technique, is performed with the No. 10 blade. The incision into the deep plane is generally placed near the anterior aspect of the parotid gland. By placing the incision this far forward with a curve at the superior aspect, the frontal branch of the facial nerve is avoided in the dissection because it is posterior and superior to the incision into the deep plane ( Fig. 16.14 ).
The lighted retractor, preferably with nonlacerating teeth, is used to gain a purchase of the SMAS and the surgeon’s wrist is turned to place the SMAS under extreme tension. The assistant provides countertraction similar to that provided when raising the skin flap. This can be awkward for the surgeon and assistant until the move is learned. Patience is encouraged in attaining the proper balance of retraction between surgeon and assistant.
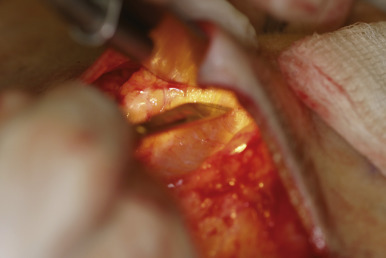
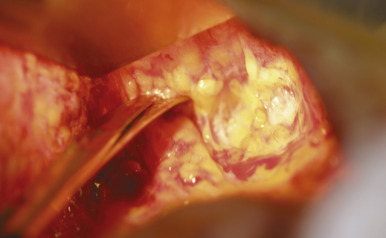
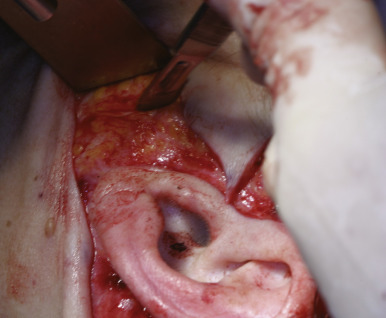
With the SMAS held taut by the lighted retractor and the countertraction provided by the assistant, the plane is incised with the No. 10 blade ( Fig. 16.15 ). Almost immediately after opening this plane, the surgeon will note the SMAS lifted up with the retractor at the roof of the dissection while the masseteric fascia falls to the floor, broadly displaying the deep plane ( Figs. 16.16 and 16.17 ). Occasionally facial nerve branches can be seen traversing this fascia ( Fig. 16.18 ). The surgeon can take great comfort in that as long as the masseteric fascia is seen, the facial nerve branches are intact. Once opened, the plane can be developed with either scissors in a spreading fashion or with the No. 15 blade in a pushing motion. We prefer to use the No. 10 blade to push down the connective tissue attachments from the undersurface of the flap ( Fig. 16.19 ). The muscle fibers of the platysma are usually seen on the undersurface of the flap and are used as guide for the dissection. The blade should be positioned so as to peel fibers from the undersurface as opposed to using the knife from the floor of the dissection and pushing the fibers up to the undersurface of the platysma. The surgeon must be mindful of the position of the mandible as the dissection continues anteriorly and inferiorly so as not to risk injury to the marginal mandibular nerve.