Keywords
Facial anatomy, Facial aging, SMAS, Facial retaining ligaments, Facial fat compartments
Introduction
The anatomy of the face is fairly constant. Variant anatomy is seen in the thickness of the soft tissue layers, and in the size and orientation of cartilaginous structures such as the nasal cartilages (nose), tarsal plates (eyelids), and facial bones (maxilla, mandible, zygoma, etc.). The relationships of nerves, vessels, and muscles of the face are fairly uniform. The facial anatomy combines to give the face form and function.
Plastic surgical procedures can significantly affect facial form and function. The vast array of surgical and injectable procedures have expanded in recent years as the want and need to improve facial function and appearance has increased. To successfully perform these procedures, a thorough knowledge of the variant facial anatomy is required.
This chapter will discuss the common anatomical relationship of the face. The layered anatomy of the face will be outlined, as will the typical position of muscles and neurovascular structures. Applied anatomy as related to surgical and injectable procedures will be highlighted.
Layers of the Face
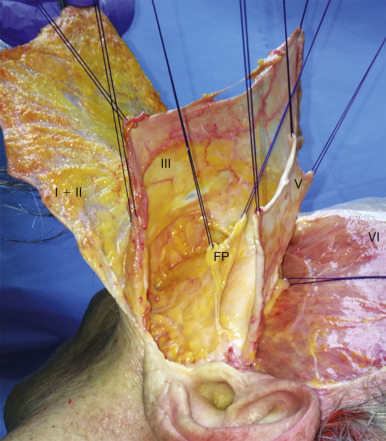
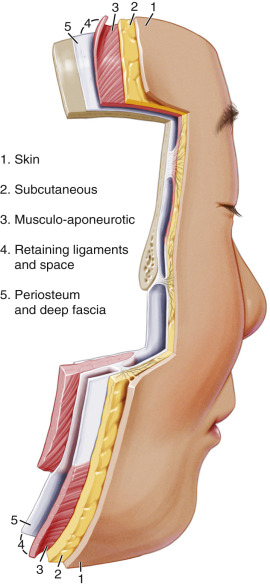
Although a few exceptions exist, the skin, subcutaneous tissues, and superficial and deep fascial layers of the face are consistent in their relationships and can be designated with a common numbering system. These layers can be numbered I to V ( Figs. 2.1 – 2.2 ). Although the names of the individual layers differ from various regions of the forehead, temple, face, and neck, the relative relationships of these layers remains constant. The muscles, nerves, and vascular structures, however, vary in their position and relationship to the layers.
The layering system of the facial levels can be seen in Table 2.1 . The various names of each layer within a given facial region are described throughout the chapter, making note of the designated numbering system.
| I | Skin |
| II | Subcutaneous tissue/superficial areolar tissue |
| III | Superficial fascia |
| IV | Loose areolar tissue |
| V | Deep fascia |
Layer I: Skin
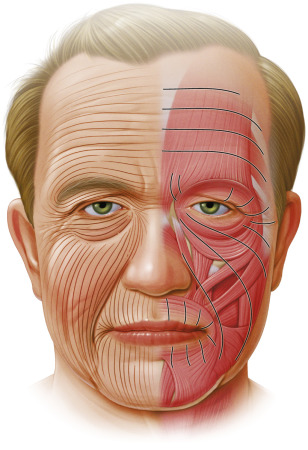
The skin varies in thickness, pigmentation, dermal appendages, and adherence to the subcutaneous tissues between different areas of the face . The skin is thickest over the mentum and in the region of the forehead and eyebrows, and is thinnest over the eyelids. In the infraorbital region and medial to the midpupillary line, the skin is thin and usually contains no subcutaneous fat. The skin is firmly attached to the underlying muscles of the oral commissure and in the region of the nasal tip, while it is loosely adherent to the underlying soft tissue in the eyelids and at the root of the nose. As the dermis of the skin thins with age, the underlying muscles cause rhytids, which generally are perpendicular to the direction of facial muscle contraction ( Fig. 2.3 ). The amount of skin wrinkling is variable, and relates to the skin thickness and elasticity.
Layer II: Subcutaneous Tissue
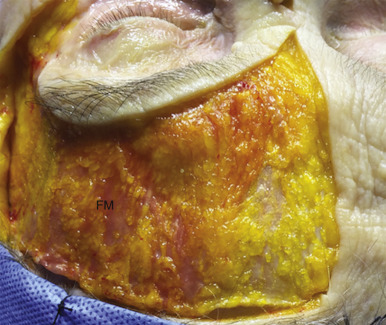
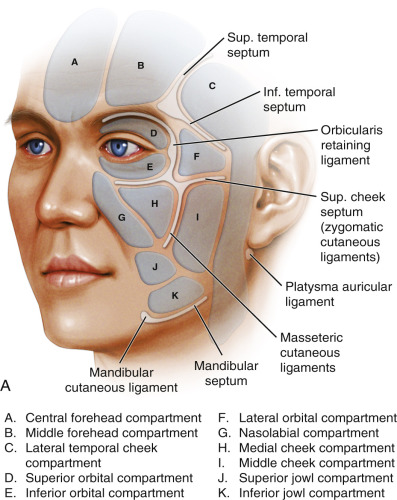
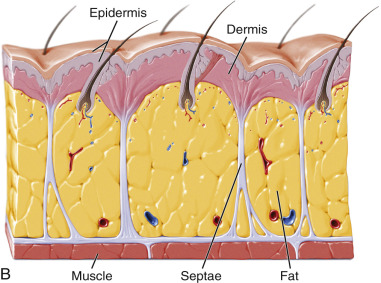
The subcutaneous tissue varies in amount in relation to the patient’s genetics, ethnicity, and body weight . In a given individual, the thickness of the subcutaneous tissue is different based on the facial region. In the forehead and over the mentum, the fat layer is thick and the overlying skin is densely adherent. However, in the eyelids, the fat layer is almost nonexistent and the skin is loosely adherent. In the midface, the subcutaneous fat is highly vascularized and compartmentalized by various fibrous septae ( Fig. 2.4 ).
Layer III: Superficial Fascia
The superficial fascia of the face is fairly adherent to the overlying skin and subcutaneous tissues of the face in most regions, and therefore must be dissected sharply from the skin in order to surgically separate these tissue planes. This is in contradistinction with the relationship of the superficial fascia with the underlying deep fascia . In most regions, the superficial fascia is loosely attached to the underlying deep fascia. Surgical dissection between the superficial and deep fascia is therefore usually blunt and easily performed.
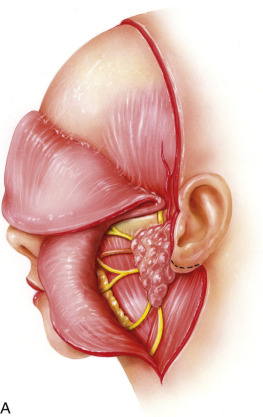
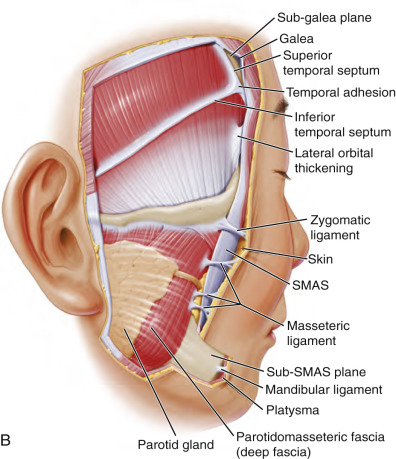
The superficial fascia has different designations in different regions of the scalp, temple, face, and neck. In the forehead, the superficial fascia is called the galea aponeurosis. This layer envelopes the frontalis muscle in the forehead, and splits to encompass the occipitalis muscle at the posterior aspect of the scalp. In the temple, the superficial fascial layer is termed the temporoparietal fascia (TPF; see Fig. 2.1 ). This layer is a thin, pliable, and vascular layer that is well suited for facial and auricular reconstruction. In the midface, the superficial fascia is the superficial muscular aponeurotic system (SMAS). The SMAS and TPF are contiguous structures, but are discontinuous at the level of the zygomatic arch. In the neck, the superficial fascia provides a fascial sleeve for the platysma muscle ( Fig. 2.5 ).
Layer IV: Deep Areolar Layer
In all regions of the head and neck, the superficial fascia (III) is connected to the deep fascia (V) by a loose areolar layer. This connection is variable and differs by age, genetics, and body weight. The attachments are typically comprised of loose connective tissue, and surgical dissection of this plane is therefore usually blunt . The specific structures that traverse this layer vary by region, and are covered later.
Layer V: Deep Fascia
The deep, or investing, fascia is a dense connective tissue that is usually immobile. It is connected to the overlying mobile superficial fascia (III) by loose connective tissue (IV). The deep fascia of the forehead is the frontal bone periosteum. The periosteum is densely adherent to the frontal bone, and becomes continuous at the superior orbital rim with the septum orbitale. The thickening at the orbital rim is termed the arcus marginale. The deep fascia of the temple is designated deep temporal fascia (DTF) or temporalis muscle fascia. This fascia overlies, and is densely adherent to, the underlying temporalis muscle (see Fig. 2.1 ) .
The deep fascia of the lateral midface is termed the parotidomasseteric fascia. This fascia covers the parotid gland and the parotid duct, and includes the buccal branches of the facial nerve. As this fascia travels towards the temple over the zygomatic bone, it becomes continuous with the superficial lamina of the DTF. The deep fascia of the neck is designated deep investing fascia. All deep fascial layers (V) are relatively fixed to the structures they overlie, and become good fixation points for repositioning of soft tissues and surgical procedures such as rhytidectomy or browlifting.
Regional Considerations
Forehead
The boundaries of the forehead are the frontal hairline (superiorly), the eyebrows and the nasal root (inferiorly), and the temples (laterally). The transition between the forehead and the temporal regions are the superior temporal lines, or the anterosuperior extent of the temporalis muscles. In this region, the fascial planes fuse and are termed the conjoined tendon (see Fig. 2.5B ).
The layers of the forehead consist of a thick skin layer (I) overlying a densely attached subcutaneous tissue (II). The skin is thick, averaging almost 2400 µm . Just deep to the subcutaneous fat is the galea aponeurosis (III). This superficial fascia of the forehead envelopes the paired frontalis muscle ( Figs. 2.6 – 2.7 ). The frontalis muscle is the only elevator of the eyebrow. Contraction of this muscle tightens the scalp, elevates the brow, and creates horizontal forehead rhytids. Deep to the galea aponeurosis/frontalis muscle is loose areolar tissue (IV) and the pericranium (V). The pericranium is the deep fascia of the forehead and is densely attached to the underlying frontal skull. As the frontalis muscle contracts, the superficial layers of the forehead slide over the underlying periosteum. This glide plane of layer III sliding over layer V affects how individuals age and how surgeons rejuvenate faces by elevating ptotic soft tissues.