The world changed on the day we now know as “9/11.” In this new era, physicians in the United States and worldwide have an additional responsibility to know the fundamentals of recognizing and diagnosing an outbreak associated with biologic agents. In this regard, the dermatologist has a particularly important role because most illnesses that arise from biologic agents can have a cutaneous component.
The Centers for Disease Control and Prevention (CDC) has identified six biologic agents as Category A agents, which pose the greatest risk for use in terrorism (Table 47-1). The assessment of risk is based on the ease of production, ease of dissemination, rate of subsequent person-to-person transmission, lethality, and psychosocial effects (literally, how terrified the community will be). These six agents are smallpox, anthrax, botulism, tularemia, plague, and viral hemorrhagic fevers.
In some, for example, smallpox, skin involvement is the most dramatic feature of the disease. In others, cutaneous manifestations are not a central feature, but it is possible, even likely, that the diagnosis of the index case will be made from cutaneous findings, whether they are subtle or obvious. For this reason, an in-depth discussion of the most dermatologically important of these agents, smallpox and anthrax, follows. The other four agents will be briefly discussed high-lighting their cutaneous findings.
Category B and C agents, second- and third-highest priority, respectively, are presented in Tables 47-2 and 47-3.
Smallpox
The patient with smallpox presents a terrible picture, unequalled in any other disease. A picture that fully justifies the horror and fright with which smallpox is associated in the public mind.
William Osler from The Principles and Practice of Medicine
Historical Aspects
The World Health Organization (WHO) regards smallpox, also called variola, as humankind’s deadliest disease. Indeed, smallpox has caused perhaps 10% of all human deaths and, even during its waning years in the 20th century, smallpox killed half a billion people. One third of its victims die. Survivors are usually maimed for life with pocked scars or blindness. Because of the mortality and morbidity associated with smallpox, people long sought ways to prevent, ameliorate, or cure the disease. Fortunately for humankind, smallpox had several characteristics that made it amenable to eradication: there is no subclinical carrier state in humans, the disease is not transmitted by food or water, and there are no animal reservoirs or vectors. The disease occurs only in humans and, during the smallpox era, it was readily diagnosed on a clinical basis alone. A person who survived a bout of smallpox achieved lifelong immunity, but most important, smallpox was preventable through vaccination.
The cowpox vaccine, which Edward Jenner used, and the vaccine that replaced it (one derived from the closely related vaccinia virus) confer near-complete immunity against smallpox. A concerted global vaccination program, led by the health organizations and governments around the world, used the vaccine to quell this disease. The last naturally occurring cases were in Bangladesh and Somalia during the mid-1970s, and a few years later the WHO proclaimed the eradication of smallpox. Shortly afterward, all laboratory stocks of variola virus were destroyed except for a few facilities that maintained small amounts of the virus, putatively for research purposes. There is worrisome speculation, however, that stocks of virus are in unmonitored hands. In addition, the ability to synthesize viral genomes in vitro brings these concerns to a new level as the altered or engineered viral strains could have virulence-enhancing properties. Consequently, there is a risk, at least theoretically, that smallpox might recur. If so, the reappearance of this disease will mark one of the most catastrophic medical, public health, and criminal events that our species has witnessed. For this reason, it is worth bringing smallpox out of the history books and into our current textbooks.
Presentation and Characteristics
Virology
Smallpox is caused by the variola virus, a member of the Orthopoxvirus genus within the poxvirus family. This genus also includes cowpox, vaccinia, monkeypox, and a few other viruses that cause mostly nonhuman disease. The poxvirus family has two other genera, one with the familiar molluscum contagiosum, and the other with the zoonotic disorders of orf and milker’s nodules. All members in the poxvirus family are DNA viruses that replicate within the host cell’s cytoplasm, unlike nearly all other viruses that replicate inside the nuclei.
TABLE 47-1 ▪ CDC Category A Agents: Biologic Agents Most Likely to Be Used in Terrorism or Warfare*
Disease
Pathogen
Likely Presentation When Used as a Bioweapon
Cutaneous Manifestations
% of Patients in a Bioterrorism Setting Who Have Cutaneous Manifestations
Smallpox
Variola, an orthopoxvirus
Classic illness described in chapter
Exanthem followed by classic vesiculopustular eruption predominantly on acral surfaces; “pearls of pus”
All
Anthrax
Bacillus anthracis, an aerobic encapsulated spore-forming gram-positive rod
Inhalational disease starts with flulike presentation and progresses
Edematous papule or plaque evolving into an ulcer surmounted by a black eschar
Roughly 50%
Plague
Yersinia pestis,an aerobic gram-negative rod with safety-pin bipolar staining
Fever, weakness, and rapidly developing pneumonia with dyspnea, chest pain, and bloody cough, leading to respiratory failure, shock, and rapid death
Bubonic form from fleabites produces painful tender enlarged lymph nodes (buboes); pneumonic plague may cause DIC with purpura
Not known
Tularemia
Francisella tularensis, an aerobic pleomorphic gram-negative coccobacillus
Hemorrhagic bronchopneumonia with fever
If acquired transcutaneously, then an ulceroglandular or lymphocutaneous presentation
Not known
Botulism
Toxin produced by the anaerobic gram-positive rod, Clostridium botulinum
Rapid onset of symmetric descending flaccid, paralysis starting in bulbar muscles; afebrile, normal mental status, and no sensory deficits
Smallpox is transmitted primarily in a respiratory manner by droplets from close contact with infected individuals. Fomite transmission, for example, from skin crusts can occur but it is rare. It is feared that weaponized smallpox, on the other hand, will be spread long distances through aerosolization of the virus.
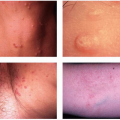
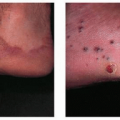
Smallpox has three clinical stages. The first, the incubation phase, starts when a person is initially infected with the virus. Incubation lasts approximately 12 to 14 days (range: 7 to 17 days) and during this time, individuals are unaware that they are infected. They feel well, have no clinical manifestations, and cannot transmit the virus to others. The second stage, the prodrome, begins with a sudden high fever (typically 102°F to 105°F) accompanied by severe headache and backache. During the prodrome, the patient is viremic, appears toxic, is often prostrate with pain, and may be delirious. After 2 to 4 days, the prodrome ends with a slight defervescence and the appearance of an oropharyngeal enanthem. This marks the beginning of the eruptive stage and now the patient is infectious. The classic exanthem has several distinctive features (Fig. 47-1). Individual lesions evolve gradually through several morphologic forms over 14 to 18 days. Lesions progress from macules to papules to vesicles to umbilicated vesicles to pustules to crusted scabs, with each form lasting 1 to 2 days. An important diagnostic feature of smallpox is that at any one time, all lesions are in the same morphologic stage of development in the region of the body. In contrast, chickenpox lesions progress rapidly and asynchronously; thus, all morphologic forms (e.g., papules, vesicles, pustules, and crusts) are typically present at any moment in the same region of the body.
TABLE 47-2 ▪ Category B Agents: Second-Highest Priority Biologic Agents to Be Used in Terrorism or Warfare
Agents/Diseases
Pathogen
Likely Presentation When Used as a Bioweapon
Cutaneous Manifestations
Brucellosis (undulant fever)
Brucella species
Flulike symptoms (fever, sweats, headaches, back pains, and physical weakness)
May cause wound infection
Epsilon toxin
Clostridium perfringens
Pulmonary edema leading to renal failure and cardiovascular collapse*
None
Food safety threats
Salmonella species Escherichia coli 0157:H7 Shigella
GI symptoms “Rose spots” in typhoid fever (Salmonella typhi)†
Malaise, myalgias, headaches, fever, chills; neurologic symptoms such as meningismus and coma may develop
Centrifugally spreading eruption that spares the palms and soles; begins as erythematous, nonconfluent, blanching macules that become maculopapular and petechial
Viral encephalitis
Togaviridae (Eastern equine encephalitis, Venezuelan equine encephalitis, and Western equine encephalitis viruses)§
Flaviviridae (Japanese encephalitis, St. Louis encephalitis, West Nile Virus)
Facial/periorbital edema, jaundice, flushing, lymphadenopathy, alopecia, palatal vesicular or petechialeruption, cutaneous morbilliform or petechial eruption may be present¶