Dermatologists have been leaders in the field of cosmetic surgery. Many procedures, products, and technologies in esthetic dermatologic surgery have been developed and researched by dermatologists. In addition, patients are increasingly turning to dermatologists for the management of concerns related to appearance. As a result, the specialty must continue to be at the forefront of cosmetic procedures and remain committed to advancing the field through innovation and scientific progress.
Soft Tissue Augmentation
Soft tissue augmentation continues to remain popular as patients seek cosmetic improvement without undergoing invasive procedures. Numerous fillers are available to correct soft tissue contour abnormalities and provide cosmetic enhancement. Although they provide numerous advantages over surgical techniques, the temporary nature of most fillers requires repeated treatment to maintain a desired outcome. Some patients find that the temporary nature of these agents is less than ideal, but one must also consider that any undesired outcomes that may potentially occur due to treatment are also temporary. In the last few years the number of available agents has increased. In Europe there are as many as 30 different filler choices. The U.S. Food and Drug Administration (FDA) has approved fewer fillers, although several new products have recently become available.
Bovine Collagen
Bovine-derived collagen has been used for decades and is the gold standard against which all filler substances are compared. However, due to advances in newer products, as well as some of the limitations of collagen (discussed later), the use of collagen for soft tissue augmentation has fallen out of popularity. However, for historical perspective and completeness as a comparison with the newer products used today, a full discussion of collagen is included here.
There are currently three FDA-approved brand-name products for use in soft tissue augmentation: Zyderm I, Zyderm II, and Zyplast (Allergan, Irvine, CA). The source for all three bovine types is a closed herd in the United States, and there have been no cases of bovine spongiform encephalopathy associated with these products. All are composed of 95% type I collagen and the remainder of type III collagen, suspended in buffered saline and 0.3% lidocaine. Zyderm I consists of 35 mg/mL of collagen, and Zyderm II has a higher concentration of 65 mg/mL. Zyplast is cross-linked with glutaraldehyde, making it more resistant to proteolytic degradation, which provides longer duration. All three products come preloaded into syringes and are stored at 4°C.
Bovine collagen hypersensitivity occurs in about 3% of the population, making skin testing a requirement before using these products. Additionally, 1%–2% of patients with a negative skin test will subsequently develop an allergic reaction after treatment. Therefore many dermatologists recommend a second skin test after an initial negative test. Patients may also develop allergy after multiple treatments. Therefore in patients with a span between treatments of more than 2 years, repeated skin testing is indicated.
Zyderm I and Zyderm II are injected into the superficial dermis, whereas Zyplast is placed deeper. A combination of threading, fanning, and serial puncture injection techniques with a 30-gauge needle can be used. Anesthesia may not be required because the product already contains lidocaine; however, regional nerve blocks may be helpful in sensitive patients or when injecting the lips. Slight overcorrection is recommended when using bovine collagen because a reduction of volume is noted due to the amount of water in the product that is absorbed.
Patients can expect 2–5 months of improvement, depending on the location of placement. Dynamic rhytids (e.g., caused by muscular activity) have a shorter duration of correction, unlike more static conditions (e.g., acne scars). Zyplast may have a longer duration because of its relative protection from enzymatic degradation. However, it must be placed deeper in the dermis to avoid a beaded surface appearance and is therefore less useful for correction of superficial rhytids.
Complications with bovine collagen include delayed hypersensitivity reactions. Although rare, allergic reactions can occur in 1% of patients who have had two negative skin tests. This presents as swollen granulomas or sterile abscesses at the treatment site. Although self-limiting, these reactions can take up to 1 year to resolve. Intralesional steroid injections, antibiotics, and systemic antiinflammatory drugs can be considered for treatment. Zyplast placed in the glabellar complex has resulted in vascular occlusion and necrosis. This may be caused by the deeper placement required with this product and the associated adverse pressure-related effects on cutaneous vasculature.
Human Collagen
One of the main shortcomings of bovine collagen is the risk of hypersensitivity reaction. Synthetic human collagen has been developed as an alternative that does not require multiple skin testing and can be administered immediately. There has been no documented cross-reaction between bovine and bioengineered human collagen, allowing patients with a documented allergy to bovine collagen to be treated safely with human collagen.
Cosmoderm 1 and 2 and Cosmoplast (Allergan) are FDA-approved bioengineered human collagen derived from neonatal foreskin. Synthetic human collagen has a very similar formulation to its bovine counterpart and is packaged in similar concentrations. Cosmoderm 1 has a concentration of 35 mg/mL and is in phosphate-buffered saline with 0.3% lidocaine. Cosmoderm 2 has a concentration of 65 mg/mL. Cosmoplast has 35 mg/mL of human-derived collagen and is cross-linked with glutaraldehyde. All products have the same indications, are injected in a similar manner to their bovine counterparts, and have similar cosmetic results and longevity.
The clinical use of collagen continues to decline as manufacturers have decreased production and transitioned to the manufacturing and promotion of hyaluronic acid fillers.
Hyaluronic Acid
Hyaluronic acid, a polysaccharide, is a natural component of human connective tissue. A member of the family of glycosaminoglycans, hyaluronic acid is composed of repeating disaccharide units. This molecule has the advantage of being identical across all species. As such, hypersensitivity reactions should not occur, and skin testing is not required before treatment. However, early formulations of hyaluronic acid did produce rare hypersensitivity reaction, although the incidence has declined with the introduction of a more purified product. Granulomatous foreign body reactions have been described in case reports.
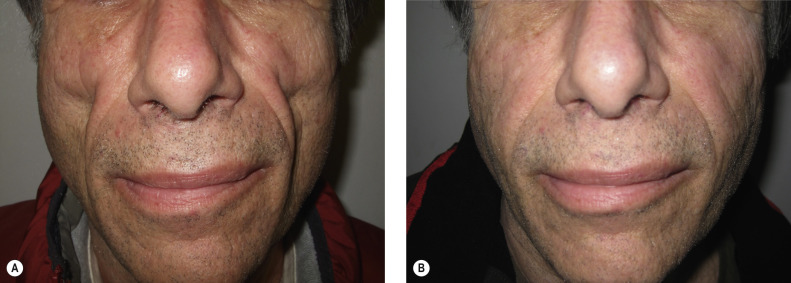
Hyaluronic acid avidly binds water, and patients may experience redness, swelling, and bruising in the first few days after treatment. Most of the volume is maintained after placement, making overcorrection unnecessary when injecting. Hyaluronic acid products consist of a clear gel in a prepackaged syringe. Early products did not contain lidocaine, often necessitating the use of local anesthesia and regional blocks for patient comfort. However, many current preparations of hyaluronic acid now include lidocaine premixed in the syringe, thus eliminating the need for adjuvant anesthesia and making them significantly more comfortable for patients. Hyaluronic acid fillers can produce a more durable esthetic improvement than collagen, often lasting from 5 to 8 months ( Fig. 39.1 ; see ).

The two types of hyaluronic acid filler substances are streptococcal derived and animal (i.e., rooster comb) derived. Streptococcal-derived filler is by far the most common as manufacturers and consumers have moved away from animal-derived products due to lack of longevity. There are numerous evolving proprietary formulations, including Restylane and its various formulations (Silk, Lyft, Refyne, and Defyne) (Galderma, Fort Worth, TX), with the “L” designation for the lidocaine-containing formulation; Juvederm and its various formulations (Voluma, Ultra, Vollure, and Volbella) (Allergan, Irvine, CA), with the “XC” designation for the lidocaine-containing formulation; and Belotero Balance (Merz; Greensboro, NC). All these fillers come in prepackaged syringes and do not require refrigeration.
The characteristics and viscosity of the different products are largely determined by the size and concentration of the molecule within each preparation. Restylane contains 20 mg/mL of hyaluronic acid, with a particle size of 100,000/mL, and is injected with a 30-gauge needle. Restylane Silk also has a concentration of 20 mg/mL, but a much larger particle size of 8000/mL, and is appropriate for deeper contour abnormalities. In contrast, Restylane Silk has a similar concentration of 20 mg/mL, but a much smaller particle size, about one fifth the size of Restylane. This make it much more appropriate for fine perioral lines. Juvederm is available in two formulations, Ultra and Ultra Plus (“XC” indicates lidocaine-containing product). Both have a concentration of 24 mg/mL, with Ultra Plus being about 20% thicker, making it more appropriate for deeper folds. Voluma, Vollure, and Volbella all are manufactured with a propriety cross-linking technology that results in longer duration of action. They have varying concentrations of HA and as a result have different consistencies and indications for use. Voluma has a concentration of 20 mg/mL and is indicated for cheek augmentation of age-related volume loss to the middle of the face. Vollure has a concentration of 17.5 mg/mL and is indicated for moderate to severe facial wrinkles and folds. Volbella has a concentration of 15 mg/mL and is the indicated for lip augmentation or perioral rhytids. Belotero Balance has a concentration of 22.5 mg/mL and has an FDA indication for moderate facial wrinkles and folds. However, due to the “thin” nature of the product, it can be used for fine superficial lines, such as perioral rhytids.
Hyaluronic acids tend to produce more swelling and bruising than collagen. Proper preoperative consultation is necessary to ensure that the patient understands this and does not have upcoming social engagements. Some have advocated the use of cannulas instead of needles to minimize the risk of bruising. Injection site necrosis is an extremely uncommon but concerning complication that has been reported with fillers. This is typically due to occlusion of arterial vessels. Application of nitroglycerin paste may help to reduce the size of the resultant ischemia. Knowledge on the impending signs of ischemia and appropriate urgent management is required for all physicians who use fillers. Improper placement of hyaluronic acid too superficially can result in a blue discoloration or nodule on the skin surface, known as the Tyndall effect. An incision with a large-gauge needle or No. 11 blade and expression of the product can be performed. Hyaluronidase injections can dissolve the product if either a reaction or unevenness results, a considerable advantage over other filler substances.
Poly-L-Lactic Acid
Microparticles of poly-L-lactic acid (Sculptra; Galderma, Fort Worth, TX) are used as an injectable implant to replace diffuse volume loss, rather than the small-volume injections of other fillers. This product is currently FDA approved for correcting facial lipoatrophy in patients with human immunodeficiency virus (HIV) infection and for esthetic treatment of lines and contour deficiencies.
Poly-L-lactic acid (PLLA) is a biodegradable, biocompatible, and immunologically inert product that does not require skin testing. PLLA has been used as absorbable suture material (e.g., Vicryl). The material is absorbed gradually in the skin, inducing a fibroblastic response and de novo collagen synthesis. Multiple treatment sessions at intervals of 4–6 weeks are often required to achieve the final result ( Fig. 39.2 ). Because correction depends on the formation of new collagen, patients must be counseled that an immediate effect does not occur with this product and they should be patient to await final improvement. Results can last for up to 2 years.
PLLA comes packaged as a freeze-dried powder and must be reconstituted for a minimum of 4 hours before injection to ensure adequate hydration of the particles. Lidocaine can be added to the vial to reduce injection pain. The product is injected using a 25-gauge needle at the level of the deep dermis and subcutaneous junction in a fanning or cross-hatch fashion. Postinjection massage for several days can help reduce nodule formation.
Side effects include bruising, swelling, redness, and delayed foreign body granulomas at injection sites. Intralesional 5-fluorouracil (5-FU) or triamcinolone may be used for the treatment of these papules.
Calcium Hydroxylapatite
Calcium hydroxylapatite (Radiesse; Merz, Greensboro, NC) consists of fine particles (25–45 µm) of material traditionally used to reconstruct bone. Once injected into the dermal–subcutaneous junction, the particles act as scaffolding for autologous collagen synthesis. The ensuing fibrotic reaction results in soft tissue correction that can last for 9–12 months. It is FDA approved for correction of moderate to severe folds and wrinkles, such as nasolabial folds, and for HIV facial lipoatrophy.
Injections can be quite painful, and local anesthesia is generally used. Calcium hydroxylapatite is injected into the deep dermis and subcutaneous junction with a threading technique using a 27-gauge needle. It comes prepackaged in syringes and can be stored at room temperature.
Nodules are more often seen when calcium hydroxylapatite is injected into the lips, thus discouraging its use in the treatment of hypolabium. Caution must be exercised; any product that requires a fibrotic reaction to be effective can result in a granulomatous reaction and an untoward result. Because calcium is radiopaque, the product may be detected and may interfere with radiologic imaging.
Silicone
Silicone has been used in the past for soft tissue augmentation by dermatologists. This product was never FDA approved, and issues of purity and safety limited its widespread use. In 1994 the FDA removed silicone from the market. Recently, however, the FDA approved 1000-centistoke liquid silicone (Silikon 1000; Alcon Labs, Fort Worth, TX) for the treatment of retinal detachment. It is currently being used off-label as permanent filler for HIV-associated facial lipoatrophy, scars, and rhytids.
The potential for delayed and severe complications with this permanent filler, as well as legal concerns and restrictions, has limited use of silicone. Adverse reactions associated with silicone injections include granuloma formation and migration of implant, which are compounded by the permanent nature of the product. Many of the past reported complications of silicone injection were the result of using either an impure, non–medical-grade substance or an improper technique with large-volume injections. A multisession, microdroplet technique, placing multiple depot injections of 0.01 mL of product into the deep dermis in 1–3 mm intervals, significantly reduces the complication rate. An additional consideration is that the current FDA-approved product is more concentrated than the previous silicone products. Further study is needed to evaluate the long-term safety and efficacy of silicone oil injections for correction of soft tissue contour deficiencies.
Polymethylmethacrylate
Bellafill (Suneva Medical, San Diego, CA), formerly ArteFill, is an FDA-approved suspension containing 20% polymethylmethacrylate (PMMA, commonly known as Lucite) microspheres of 30–40 µm in diameter, suspended in 80% bovine collagen, for soft tissue augmentation. The carrier collagen provides initial correction and is degraded over several months, leaving the PMMA microspheres. PMMA is nondegradable and serves as a permanent framework for connective tissue deposition and can produce long-term correction.
Technique is critical to successful outcomes. If injected too deeply, the implant is ineffective; superficial placement can cause prolonged erythema. Granuloma formation and hypertrophic scarring can occur and have been reported as a delayed reaction. Intralesional triamcinolone can be used for treatment of these reactions. One patient who developed a delayed foreign body granuloma 6 years after injection with PMMA was successfully treated with a 24-week course of 600 mg/day of allopurinol. Intralesional triamcinolone has also been used as a treatment for granulomas. Because the product contains bovine collagen, skin testing is required before use. Early indications suggest efficacy of triamcinolone treatment for acne scarring.
Expanded Polytetrafluoroethylene
Expanded polytetrafluoroethylene (ePTFE) is a synthetic solid material that is soft and pliable, is not degraded, and has the advantage of being permanent. The material is placed through a small skin incision and positioned in the desired location. Areas typically treated include lip margins or the muscular portion of the vermillion for enhancement, nasolabial folds, and soft tissue depressions. Complications associated with ePTFE include extrusion, migration, shrinkage, and hardening.
Autologous Fat Transplantation
Autologous lipotransfer allows for soft tissue augmentation without the risk of allergy, rejection, or infectious transmission. Unlike other filler techniques, fat transfer is truly a grafting procedure. As such, its success is predicated on the survival of the transferred adipocytes. Fat is harvested from a choice of donor sites, typically the abdomen, buttock, thigh, or knee. There is no consensus as to the advantages of harvesting with a liposuction cannula, syringe extraction with a large-bore needle, or open surgical method. The fat is then separated from anesthetic fluid and blood and injected through a large-bore needle (16–18 gauge) into the desired location. Any remaining fat can be frozen at −70°C for use later, with varying claims regarding loss of efficacy.
The variable rate of graft survival, the recipient site reaction (bruising, swelling), and the added morbidity of a donor site are limiting factors in patient satisfaction with this technique. In some cases, partial survival results in uneven correction that may require additional treatments. Some argue that multiple smaller-volume injections spaced over two or three treatments are more effective than single, large-volume lipotransfer. If the fat survives, it can provide a very natural correction. However, local factors such as motor activity and gravitational effects will mitigate against permanent correction. This technique is not useful for the correction of superficial rhytids and mainly corrects deeper defects such as nasolabial folds, hypolabium, buccal depression, and deep scars.
Bachmann F, et al: The spectrum of adverse reactions after treatment with injectable fillers in the glabellar region. Dermatol Surg 2009; 35: 1629.
Benedetto AV, Lewis AT: Injecting 1000 centistoke liquid silicone with ease and precision. Dermatol Surg 2003; 29: 211.
Chen F, et al: HIV-associated facial lipoatrophy treated with injectable silicone oil. J Am Acad Dermatol 2013; 69: 431.
França Wanick FB, et al: Skin remodeling using hyaluronic acid filler injections in photo-aged faces. Dermatol Surg 2016; 42: 352.
Glogau RG: Fillers. Semin Cutan Med Surg 2012; 31: 78.
Goldman MP: Cosmetic use of poly-L-lactic acid. Dermatol Surg 2011; 37: 688.
Hexsel D, de Morais MR: Management of complications of injectable silicone. Facial Plast Surg 2014; 30: 623.
Jagdeo J, et al: A systematic review of filler agents for aesthetic treatment of HIV facial lipoatrophy (FLA). J Am Acad Dermatol 2015; 73: 1040.
Joseph JH, et al: Current concepts in the use of Bellafill. Plast Reconstr Surg 2015; 136: 171S.
Kadouch JA, et al: Delayed-onset complications of facial soft tissue augmentation with permanent fillers in 85 patients. Dermatol Surg 2013; 39: 1474.
Landau M: Hyaluronidase caveats in treating filler complications. Dermatol Surg 2015; 41: S347.
Ledon JA, et al: Inflammatory nodules following soft tissue filler use. Am J Clin Dermatol. 2013; 14: 401.
Levy RM, et al: Treatment of HIV lipoatrophy and lipoatrophy of aging with poly-L-lactic acid. J Am Acad Dermatol 2008; 59: 923.
Lorenc ZP, et al: Review of key Belotero Balance safety and efficacy trials. Plast Reconstr Surg 2013; 132: 33S.
Matarasso SL: Injectable collagens. Plast Reconstr Surg 2007; 120: 17S.
Moulonguet I, et al: Foreign body reaction to Radiesse. Am J Dermatopathol 2013; 35: e37.
Rayess HM, et al: A cross-sectional analysis of adverse events and litigation for injectable fillers. JAMA Facial Plast Surg 2017 Dec 21; ePub ahead of print.
Requena L, et al: Adverse reactions to injectable soft tissue fillers. J Am Acad Dermatol 2011; 64: 1.
Tzikas TL: A 52-month summary of results using calcium hydroxylapatite for facial soft tissue augmentation. Dermatol Surg 2008; 34: S9.
Botulinum Toxin
The use of botulinum toxin (BTX) in dermatology has increased rapidly over the years, and at present it is one of the most common cosmetic procedure performed in the United States. In 2002 the FDA approved onabotulinumtoxinA for the treatment of dynamic glabellar frown lines. Although BTX is most frequently used for relaxation of dynamic rhytids in the upper third of the face, advanced esthetic treatment techniques for additional anatomic sites have been developed and are currently used off-label.
Produced by Clostridium botulinum, there are seven different serotypes of BTX: A, B, C1, D, E, F, and G. These serotypes inhibit the release of acetylcholine from the presynaptic motor neuron, resulting in chemodenervation and paralysis of the treated muscle. Over time, new nerve terminals form and create new neuromuscular junctions with the muscle fibers, which gradually restore motor function.
BTX type A (Botox Cosmetic [onabotulinumtoxinA], Allergan; Dysport [abobotulinumtoxinA], Medicis); Xeomin (incobotulinumtoxinA; Merz) is the most common serotype. Its mechanism of action is through the cleavage of SNAP-25, a presynaptic membrane protein required for fusion of neurotransmitter-containing vesicles. Effect is generally noted 2–5 days after treatment with BTX-A, but the delay can be as long as 2 weeks in some cases. Results can last 2–5 months. In addition to esthetic indications, onabotulinumtoxinA is FDA approved for the treatment of blepharospasm, strabismus, cervical dystonia, upper limb spasticity, chromic migraine, urinary incontinence, and axillary hyperhidrosis.
Each of these BTX-A products has a similar mechanism of action, but each formulation also has unique characteristics. For dosing purposes, onabotulinumtoxinA and incobotulinumtoxinA have a similar potency (clinical equivalency ratio of 1 unit = 1 unit). AbobotulinumtoxinA has equivalency of 3 : 1 compared with the other formulations. Therefore it is critical that physicians perform appropriate dosage conversions when switching among different products. AbobotulinumtoxinA appears to have greater spread once injected into the skin. IncobotulinumtoxinA is unique in that it is formulated with no complex proteins and thus, in theory, may have a lower risk of neutralizing antibody formation (although the risks of this occurring in esthetic use is exceedingly low with all current formulations of BTX-A). In addition, incobotulinumtoxinA has the advantage of being able to be stored refrigerated or at room temperature, whereas the other products require refrigeration. Newer formulations of BTX-A are currently under investigation and may result in even more options for the patient and physician in the future.
The only other serotype that is currently available commercially is BTX type B (Myobloc [rimabotulinumtoxinB]; Solstice Neurosciences, Malvern, PA). Its mechanism of action is through the cleavage of a vesicle-associated membrane protein (VAMP), also known as synaptobrevin. This serotype has more rapid onset of effect than BTX-A. In addition, differences in potency suggest that approximately 100 units of Myobloc are equivalent to 1 unit of Botox. It currently has FDA approval for the treatment of cervical dystonia.
BTX-A is distributed in vials as a vacuum-dried powder, which is reconstituted with 1.0–5.0 mL of saline. Many physicians think that the dilution of BTX does not a make a significant difference in patient outcome, and studies appear to confirm this. Others argue that higher concentrations with smaller injection volumes reduce the amount of unintended diffusion. It is more important to use the same dilution every time to ensure that the physician does not need to do “mental math,” and to reduce confusion with each new vial of BTX.
Despite package insert recommendations, experience suggests that there is little loss of potency over several weeks after reconstitution with preserved saline. The American Society for Dermatologic Surgery has put out a consensus statement regarding the storage and reuse of previously reconstituted botulinum toxin. The use of preserved saline for reconstitution reduces the burning and pain associated with injection from the anesthetic properties of the benzyl alcohol in preserved saline.
BTX-A is predominantly used in dermatology for treatment of dynamic rhytids on the upper third of the face. The key to successful treatment is understanding the anatomy involved in facial expression, rather than performing the procedure by rote. Having the patient frown, squint, and raise the brows before treatment helps identify the active target muscles and serves as a guide for proper placement.
Glabellar Frown Lines
Currently, treatment of glabellar frown lines is the only FDA-approved cosmetic indication for BTX-A. These lines result from contraction of the corrugator supercilii muscle, which pulls the brows medially, and the procerus muscle, which pulls the brow inferiorly. In addition, by inactivating the brow depressors, unopposed action of the brow elevators (e.g., frontalis muscle) can result in a slight but noticeable brow lift.
Approximately 20–35 units of onabotulinumtoxinA (or equivalent if using different product) are typically injected into the corrugators and procerus in a five-point injection method ( Fig. 39.3 ; see ). Male patients and those with larger muscle mass may require a higher number of units (30–50). By having the patient furrow the brow, one can identify the origin and insertion of the corrugator supercilii. By grasping with the thumb and index finger, the physician can isolate the muscle and ensure accurate toxin placement.










