The main objectives of rhinoplasty in African descendants are to improve the definition and projection of the nasal tip, augment the dorsum, and reduce the alar base. Open rhinoplasty using costal cartilage graft, with lateral crural tensioning and septal extension graft associated with en bloc dorsal augmentation is the workhorse. Cartilage resections should be minimal. Oral isotretinoin and triamcinolone injection may improve tip definition. Surgical success ultimately depends on the ability of the surgeon to accurately identify the anatomic variables and reconcile these anatomic realities with the patient’s aesthetic expectations and his or her sense of ethnic identity.
Key points
- •
The main objectives of rhinoplasty in African descendant patients are to improve the definition and projection of the nasal tip, augment the dorsum, and reduce the alar base.
- •
Open rhinoplasty with costal cartilage graft is the preferred technique for rhinoplasty in African descendants.
- •
Lateral crural tensioning with septal extension graft associated with en bloc dorsal augmentation is the workhorse in rhinoplasty of African descendants.
- •
The use of isotretinoin in pre- and postoperative periods may lead to better outcomes in tip definition.
- •
Postoperative injections of triamcinolone can help reduce supra-tip edema and tip definition.
Introduction
The study of anthropometry in Negroid (originally named Ethiopian) faces and noses has been well documented for decades. More recently, an increase in the number of patients of African descent searching for aesthetic procedures has brought a lot of new scientific information to the field.
Based on a survey, the American Society of Plastic Surgeons (ASPS) estimates that 18 million cosmetic procedures were performed in United States during 2019. Segmenting, 30% of those procedures were performed on non-Caucasian patients. In 2005, non-Caucasian patients accounted for 22% of all cosmetic procedures. In 2019, 9% of the patients were black or African American, representing approximately 1.7 million cosmetic procedures. In 2004, this population comprised 5% of cosmetic procedures. , From 1999 to 2001, there was a reported 340% increase in African American patients requesting cosmetic procedures.
The same survey from the ASPS estimates that more than 200,000 rhinoplasties were performed in 2019, whereas 7% of those were performed on patients of African descent, which translates to approximately 14,000 rhinoplasties. This article discusses new advances in surgical techniques and clinical care for rhinoplasty in African descendants.
Anatomy and clinical features
The African descendant’s nose presents specific anatomic characteristics that are relevant to rhinoplasty.
Skin and Subcutaneous Features
The skin on the nose of the African descendants is thicker, sebaceous, and inelastic, especially at the tip, which is bulbous, flattened, and ill-defined. It is necessary to remember, at the time of grafting, that over the upper nasal third the nasal skin and subcutaneous fat is fairly thick and becomes relatively thin over the middle third.
In the subcutaneous tissue, mainly in the nasal tip, there is a greater amount of fibrofatty tissue (about 2–4 mm), one of the factors that compete for not defining the tip.
This traditional description may not reflect the whole diversity of skin thickness encountered among patients of African descent. Categorizing the African nasal skin envelope as mild, intermediate, or severely thick is more helpful in anticipating its response to rhinoplasty.
Nasal Tip
Lower lateral cartilages (LLCs), skin, and subcutaneous tissue form the nasal tip. The LLCs are not thinner and weaker than those of Caucasians, as was thought initially. , The large amount of fibrofatty tissue between the domes, the obtuse angle (>90°) between the medial and lateral crura, the acute lateral crural cartilage angle of inclination relative to the maxilla, 3 short columella, and the hypodeveloped nasal spine cause the lack of projection and definition of the nasal tip, creating an aspect of a flat and bulbous tip.
In African descendants, the projection of the tip of the nose is generally smaller than in Caucasians (0.67 times the ideal nasal length), approximately 0.5 times the ideal nasal length. The rotation may vary, but, in general, there is an under-rotated tip (African American vs Caucasian is 86–91 vs 99 in women and 83 vs 98–100 in men, respectively).
Nasal Pyramid
The nasal bones in African descendant patients are shorter and have an obtuse angle between each other, resulting in a flatter and broader appearance of the dorsum, both in the upper and the middle thirds.
The nasofrontal angle is usually at the height or caudal to the pupil line and varies from equal to more obtuse than in Caucasians, because the radix is deeper set and wider (25–27 mm compared with 15–16 mm in Caucasians).
Alar Base
In the African descendants, the columella is short and wide, contributing to the ovoid shape and horizontal oriented nostril. The columella to tip lobule relationship is usually 1.4 to 1.5:1, which is shorter than the classic 2:1 ratio. , , , The nasolabial angle is acute because of the more cephalic position of the nasal septum and the underdevelopment of nasal spine.
The pyriform aperture shape more ovoid and with a shorter vertical height compared with Caucasians, contributing to an extremely wide alar base. , Compared with the traditional ratio of a 1:1 relationship between intercanthal distance and nasal base width, the relationship is 1:1.25 and 1:3 in African American women and men. ,
Further, a more horizontal orientation of the LLCs leads the ala to flare beyond the alar base attachment in African descendants by more than 2 mm. The lateral wall of the nostril can be bulky.
Goals
Among patients of African descent, the final ideal result should be a balanced-looking nose that blends in with the patient’s face, preserving the ethnic features. The objective is to have a nose as close possible of the standard of beauty, maintaining its ethnic characteristics and creating better harmony and nasofacial balance. Therefore, the objectives of rhinoplasty in African descendants are to improve the definition and projection of the nasal tip, augment the dorsum, and reduce the alar base.
To operate on the nose of African descendants, one must first have a careful conversation with the patient, realistically defining the changes proposals, keeping the nose as close as possible to the standard of beauty, without losing its ethnic characteristics. ,
Preoperative clinical treatment
The medical treatment of the skin-soft tissue envelope with isotretinoin is recommended. There are few studies; however, evidence suggests that the use of oral isotretinoin in patients with thick skin accelerates improvement in cosmetic results during the early months after surgery, and the patients were more satisfied with their operation outcomes and experienced fewer skin problems. On the other hand, it seems that isotretinoin does not significantly affect the final cosmetic result in 1 year.
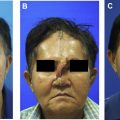
Patients usually receive a drug regimen a dose ranging from 0.25 mg/kg to 0.5 mg/kg for a period of 4 to 6 months. The authors’ protocol starts 30 to 60 days before surgery and is suspended 7 days before surgery. Then, 15 days after surgery it is resumed and kept for approximately 6 months ( Fig. 1 ). All patients should be monitored with hepatic function tests.

Surgical techinique
Anesthesia
All procedures are performed under general anesthesia with remifentanil and propofol (topical anesthesia with cotton soaked in 2% tetracaine with adrenaline 1: 1,000, which remains in the nasal cavity for 10 minutes; local anesthesia with extravascular infiltration of 5 mL of 1% ropivacaine with adrenaline 1: 100,000).
Obtaining Autologous Grafts
The grafts can be obtained from septal cartilage, conchal cartilage, or costal cartilage. However, in most rhinoplasties in African descendants, the septal cartilage is weak; thus it is strongly recommended to harvest costal cartilage. Implants should be avoided.
The nasal septum cartilage is obtained through routine septoplasty with elevation of the mucosa, releasing the cartilage septum from its junction with the perpendicular plate of the ethmoid (PPE) and incising it dorsally and caudally, preserving 1.5 cm anteriorly and 1.5 cm dorsally. It can be used as a septal extension graft (SEG), a tip graft, alar contour grafts, and dorsum augmentation. The PPE can also be harvested and used as a splint to the septum or to the SEG. As previously stated, there are few cases in which the septal cartilage is enough for rhinoplasty in African descendants.
The conchal cartilage, because of its flabbiness, can be used as camouflage or dorsum augmentation, but cannot be used as structural grafts, so it is almost never used.
Costal cartilage is the preferred material for grafts in rhinoplasty of African descendants. A piece with 5.0 to 7.0 cm can be obtained with a 1.5 to 2.0 cm incision. Rectus abdominis fascia can also be harvested through the same incision. Using the oblique split technique to carve the grafts avoids cartilage wrapping.
Incision/Dissection
Open rhinoplasty is the preferred approach. Despite the skin being thick and oily, the transcolumellar scar is inconspicuous. Bilateral marginal incisions are joined with an inverted V incision in the middle of the columella. Dissection of the lower lateral cartilages is performed in the supraperichondrial plane. The subperichondrial plane may be tricky, because the weakness of the LLC may jeopardize tip sutures. Care should be taken exposing the Pitanguy ligament in the midline; it should be transected carefully and preserved for reconstruction as a final step of the surgery. The bony dorsum is dissected in a subperichondrial/subperiosteal plane, creating a pocket limited to the area in which reduction or augmentation is planned.
Osteotomies
The nasal bone of African descendants usually has a broad base, requiring lateral osteotomies with a 3 mm chisel, with upward perforation at the nasomaxillary angle, with fracture in the medial direction for narrowing the nose. In cases with the nasal dorsum excessively low and in which a large augmentation will be necessary, the osteotomy might be unnecessary. Other osteotomies are reserved for crooked noses.
Nasal Tip
The maneuvers performed on the tip of the African descendant’s nose aim to improve projection and definition of the nasal tip, to set rotation desired by the patient, and balance it with the height of the dorsum. The algorithm of treatment of tip is defatting, SEG, LCT, tongue in groove, tip graft, and alar rim graft.
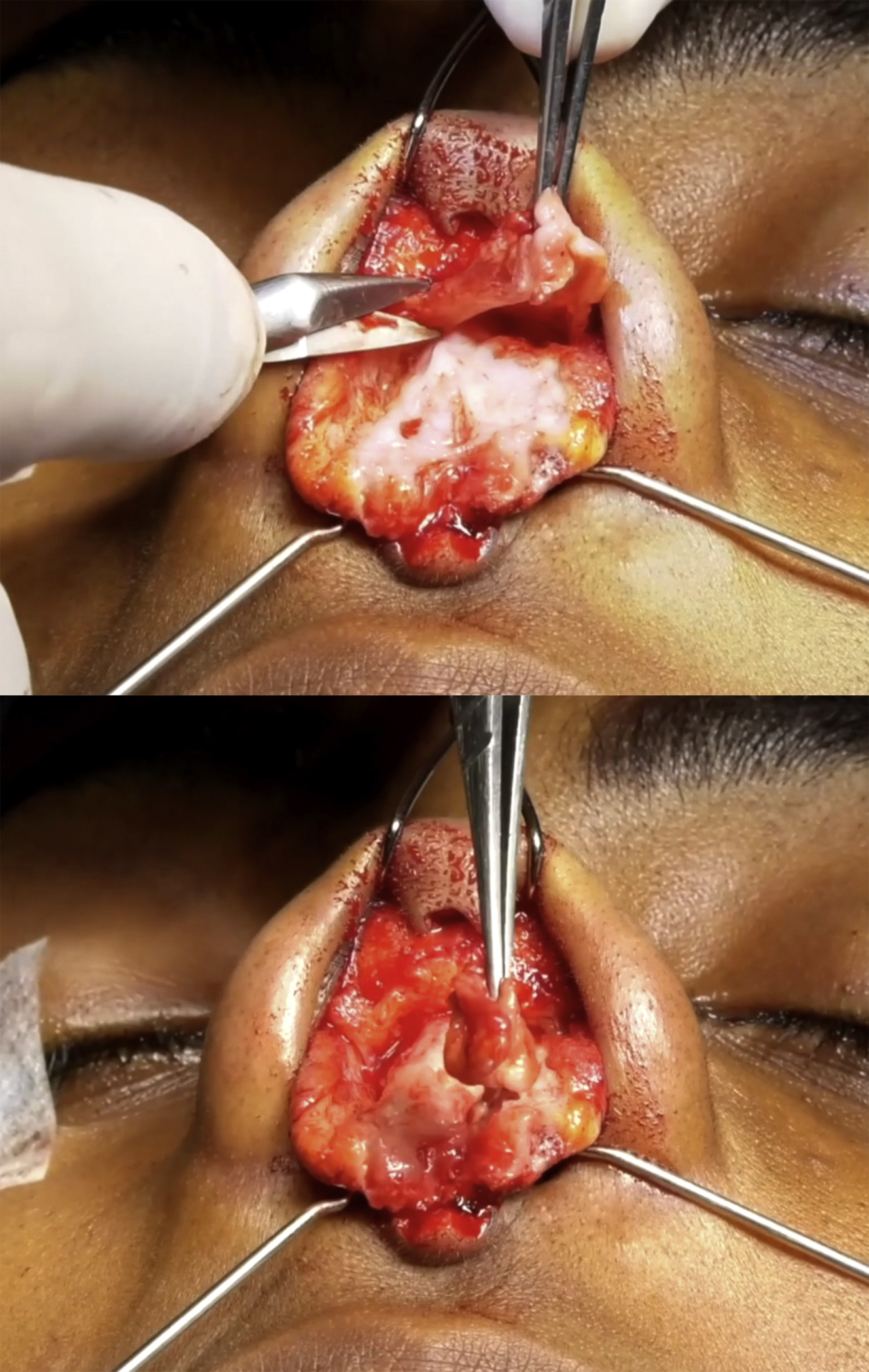
The defatting is an important step to help control skin thickness ( Fig. 2 ). Selective debulking allows one to maintain the highlights in the center of the tip and to help keep the shadows in the supra tip and scroll areas, giving a better refined tip. , The Pitanguy ligament should be totally dissected, transected at the supra tip area, and preserved for reinsertion at the end of the procedure. Carrying the dissection further posteriorly to the anterior nasal spine between the medial crura creates a soft tissue flap that can be used at end of the operation to cover all the grafts of the tip.
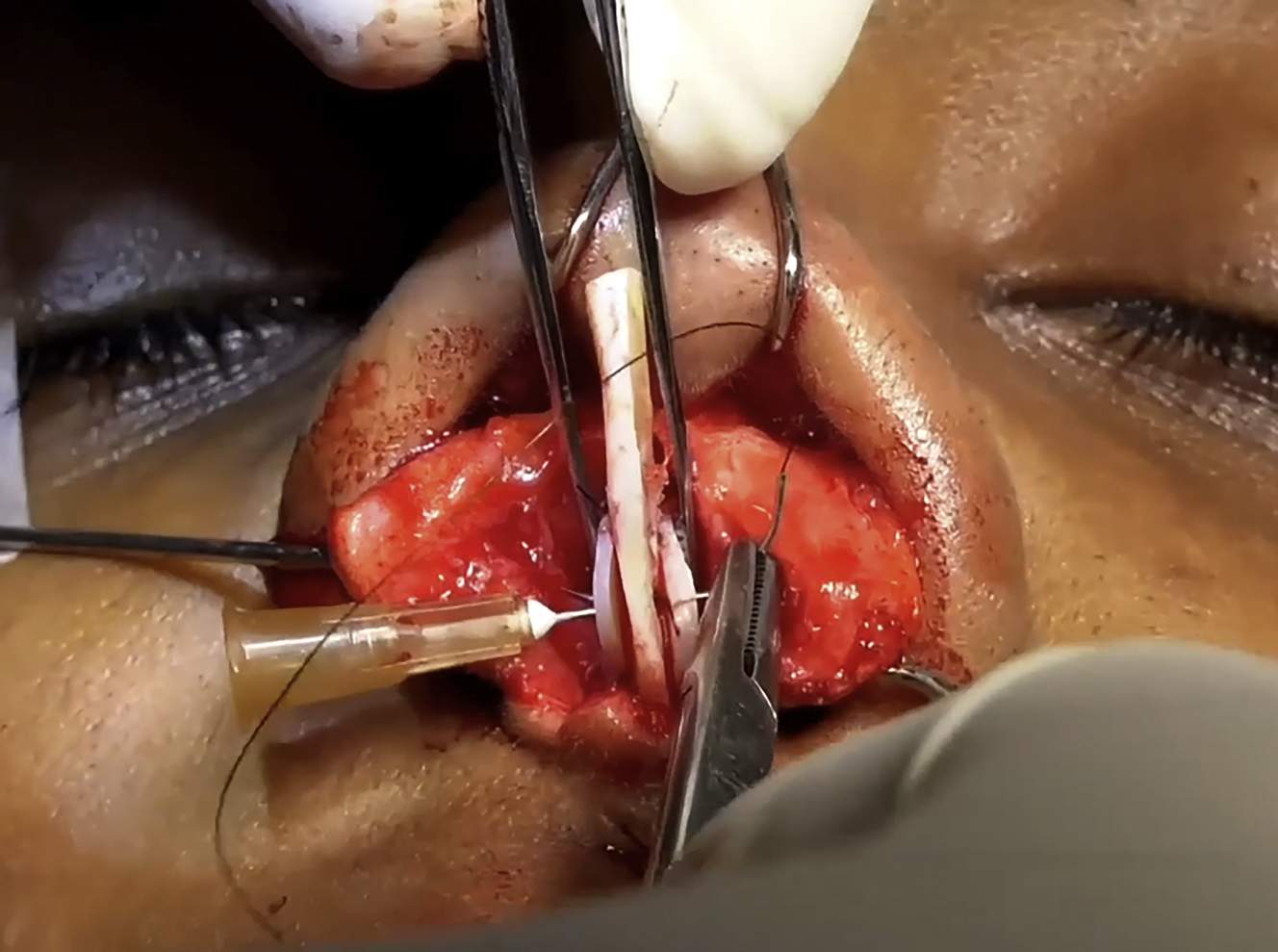
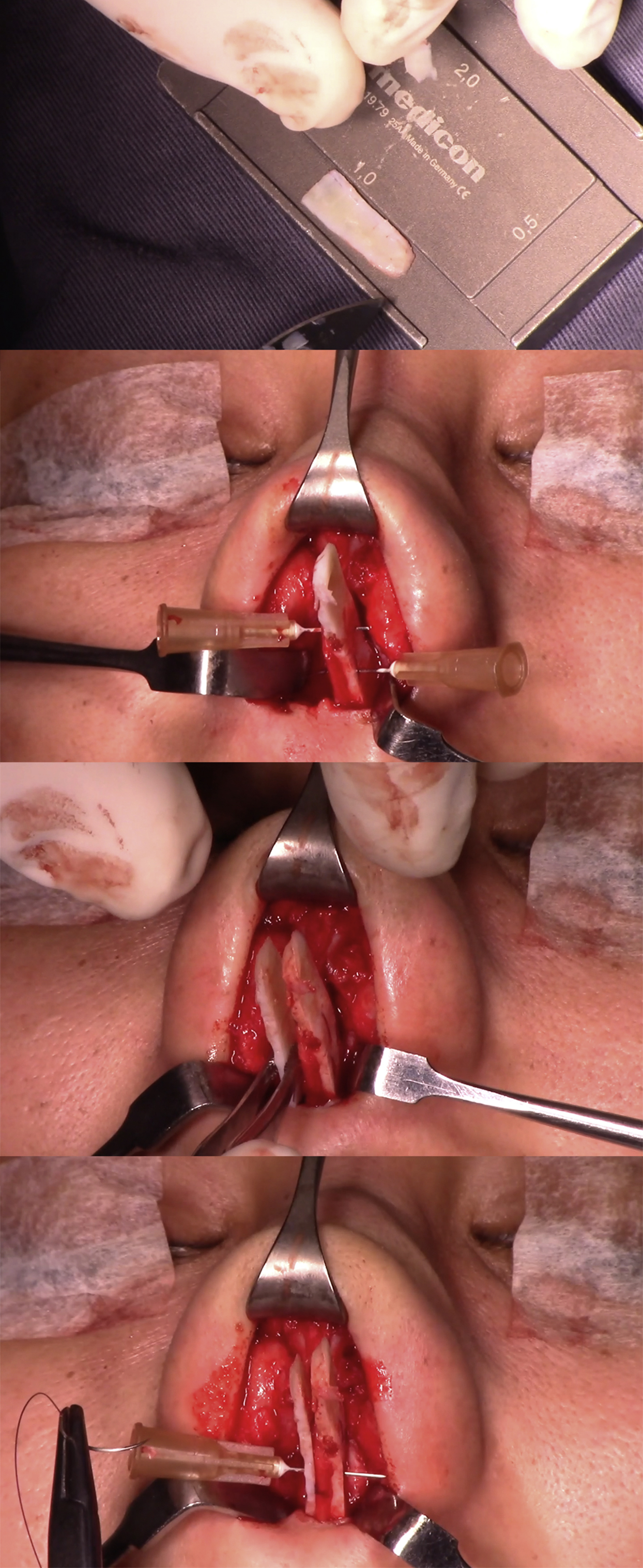
The SEG is the most important graft in modern rhinoplasty, especially in African descendants in whom there is total absence of nasal tip support a very thick skin. Without adequate tip support is unlikely to achieve long-term tip definition and projection. The SEG is fixed to the caudal septal to increase septal length and height. The position of the graft will set the tip rotation and projection; therefore, it should be carved carefully and may receive minor adjustments after its fixation. The stabilization of the SEG with additional cartilage or bone splints is mandatory. In end-to-end fixation, bilateral extended spreader grafts and bilateral splints in the posterior septal angle must be used to avoid tilting ( Fig. 3 ). In lateral-to-lateral fixation, a contralateral splint should be used to set the midline. The authors advocate the use of lateral-to-lateral fixation, but with the use of bilateral costal cartilage SEG to have the maximum support possible to counteract skin thickness and scar contracture ( Fig. 4 ). The graft is carved to span the whole height of the caudal septum and to set the tip position 10 to 12 mm above the final dorsum height. The 2 SEGs are fixated to the caudal septum with several 5-0 polydioxanone mattress sutures. After desired projection and rotation are achieved, the tip of the SEG should be trimmed to achieve better tip refinement and projection.
Related posts:
 Forehead Lift for Asians
Forehead Lift for Asians
 Incisional Blepharoplasty for the Asian Eye
Incisional Blepharoplasty for the Asian Eye
 Special Considerations in Facial Reconstruction in the Non-White Patient
Special Considerations in Facial Reconstruction in the Non-White Patient
 Recent Trends in Orthognathic Surgery in Asia
Recent Trends in Orthognathic Surgery in Asia
 Special Consideration in Rhinoplasty for Deformed Nose of East Asians
Special Consideration in Rhinoplasty for Deformed Nose of East Asians
 Cosmetic Bone-Contouring Surgery for Asians
Cosmetic Bone-Contouring Surgery for Asians
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


