9 Augmentation and Mastopexy—Basic Principles to Develop a Treatment Plan and Technical Pearls
Summary
This chapter describes the operative technique for single-stage breast augmentation with mastopexy. The preoperative evaluation of the patient, including musculoskeletal, nipple areolar, inframammary fold, skin type, ptosis, and volume, assessment, is detailed. Three techniques for the mastopexy are then described in depth: circumareolar, vertical or “lollipop,” and Wise pattern. The chapter concludes with a brief description of useful adjunctive procedures (liposuction and nipple reduction) and postoperative care.
9.1 Introduction
Single-stage augmentation mastopexy remains a key operation in plastic surgery because there are no effective nonsurgical modalities to lift the breast. The authors present an overview that represents the senior author’s personal techniques, which have evolved over three decades of experience with the benefit of long-term follow-up and revisiting existing literature. 1 , 2 , 3 , 4 , 5 , 6 This chapter is in no way intended to discard alternative procedures that may prove to be useful in the future. For example, acellular dermal matrix and other scaffolds are being developed that may be proven to provide long-term additional support and better outcomes. The authors recognize that techniques will continue to evolve.
The tendency toward using shortened scars has often pushed surgeons to the brink and beyond, sacrificing breast shape and long-term results to avoid a few additional centimeters of scar. A wise man once said, “If there are many ways to perform a procedure, there is usually no perfect answer” (Melvin Spira, M.D. F.A.C.S., personal communication). This chapter describes three different techniques for augmentation mastopexy: circumareolar, vertical “lollipop,” and a Wise-pattern mastopexy. In the opinion of the authors, the surgeon should be well versed in all techniques to avoid stretching indications and producing poor results. When indications are stretched, techniques that are good become techniques that do not work. For example, a circumareolar lift that attempts to overcome excess ptosis and poor skin quality will result in a stretched, deformed areola with minimal or no improvement in glandular ptosis (Fig. 9‑1). A vertical “lollipop” mastopexy, which extends the circumareolar mastopexy to incorporate a vertical skin excision, represents a middle ground between the circumareolar and the Wise-pattern mastopexy. If overused, the vertical mastopexy can result in scars that are too long, a too-high-nipple deformity, redundant glandular ptosis, and the need for lower-pole horizontal skin excision. The Wise pattern is the “go-to” for breast excellence in the majority of cases because it is predictable, consistent, and versatile. In the authors’ experience, a small minority of patients present with good skin elasticity and minimal ptosis, and these are the patients that benefit from circumareolar or vertical mastopexies. All techniques can be overused or exaggerated, therefore creating suboptimal results with any of them. Consequently, the preoperative plan and realistic expectations are the keys to quality outcomes.

9.2 Preoperative Evaluation
9.2.1 Patient Evaluation
Images of the ideal youthful breasts found in popular fashion advertising, most notably Victoria’s Secret, have simultaneously created the best- and worst-case scenario for plastic surgeons. The best-case scenario is an increased desire for breast enhancement. The worst-case scenario is that all women expect their breasts to be round, full, without any element of ptosis. The patients often fail to recognize that these are painstakingly selected models who are naturally anatomically blessed and/or often have had breast enhancement. When a surgeon fails to match reality and patient expectations, unhappiness ensues for both patient and surgeon. Skin type, breast tissue type, body habitus, age, skeletal issues, postpartum status, and menopause will all influence outcomes. Moreover, all results are subject to forces of time, gravity, and the aging process. Skin may not “hold up” because of inherent loss of elasticity in spite of a perfectly executed procedure. A critical part of the preoperative evaluation, therefore, involves listening to the patient’s concerns and setting realistic expectations. This includes reviewing photos of what they can expect, discussing how realistic their expectations are, and explaining how results can change over time (Fig. 9‑2).

The authors’ preference is to meet with patients while they are fully clothed. This allows a neutral setting to discuss concerns regarding size, ptosis, and any existing asymmetry. A detailed past medical history is taken, with particular attention paid to weight fluctuations, pregnancies, breastfeeding, menopause, hormonal replacement therapy, oral contraceptives, age of onset of breast growth/rapid breast growth in younger women, personal or family history of breast cancer, and appropriate radiographic breast evaluation. The authors recommend an early baseline mammogram for patients 35 years of age or older. The risks of needing further imaging or even biopsies, as well as the current recommendations for screening guidelines, are discussed. If patients younger than 40 years old refuse mammograms, this is documented in the chart. Patients who are 40 years of age or older must have imaging within 1 year of the surgery to proceed. All patients are evaluated within 30 days of surgery because weight changes and skin changes can occur rapidly, significantly altering the preoperative appearance and potentially requiring a different operative technique.
9.2.2 Examination
Musculoskeletal Assessment
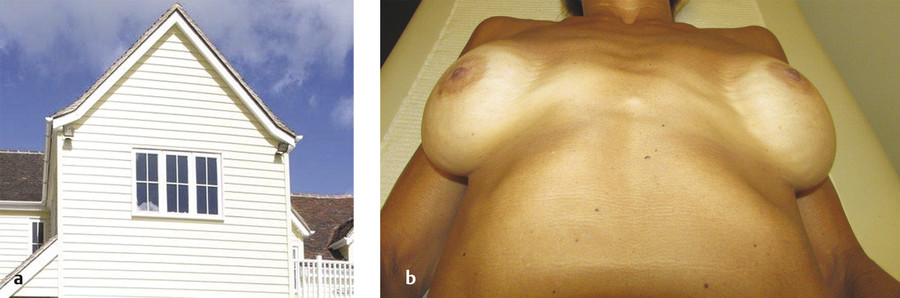
Examine the patient’s skeletal framework and look for scoliosis and other skeletal abnormalities: pectus deformities, prominent ribs, or a downward and laterally sloping chest wall. All skeletal abnormalities and asymmetries can and will be exaggerated postoperatively following implant placement. Excess lateralization of implants is frequently a consequence of a common chest wall variant, which we refer to as a sloping chest wall. In this variant, the sternum is the peak of the “roof,” and the laterally sloping ribcage does not provide a level platform to support the implant (Fig. 9‑3). These skeletal asymmetries cannot be emphasized enough. Patients are often unaware of them and do not comprehend the challenges that their unique anatomy presents and cannot be overcome. 7
Nipple Areolar Assessment
Measure the distance from the sternal notch to the nipple bilaterally and also from mid-sternum to nipple. Point out any asymmetries. The youthful ideal nipple position is an equilateral triangle of 21 cm on each side, but this is rarely seen in patients requiring a mastopexy. 8 Markings of nipple position should be made by simultaneously palpating the inframammary fold (IMF) and the breast tissue to approximate the new nipple position. Lowering the nipple position based on the location of the IMF and the patient’s individual anatomy will lessen the likelihood of a “too-high-nipple deformity.” Nipples can be long and ptotic, or overly projecting.
Nipple reduction should be discussed with the patient as a possible adjunct, much as a chin implant or genioplasty may be mentioned to a rhinoplasty patient to correct facial imbalance.
Inframammary Fold
Note the medial take-off (D1) and lateral extent of the IMFs (D2). The diameter of each and the position of the IMF on the chest wall are frequently asymmetric, and these asymmetries should be pointed out to the patient. Patients are asked to lift their breasts to reveal the true height of the IMFs that are concealed by existing glandular ptosis. The presence and adjunctive treatment of axillary fat deposits may be discussed at this time.
Patients may present with a long torso, and thus have a long breast footprint. 9 The patient often perceives this as ptosis, when it really reflects a lowered position of the breast itself and the IMF. It exacerbates ptosis and the perception of ptosis. The position of the IMF cannot be raised in a routine mastopexy, and attempting to correct the long breast footprint with raising the nipple areolar complex (NAC) will result in a too-high-nipple deformity.
Skin Type
Skin type is evaluated by visual examination and palpation. Shiny thin skin, telangiectasias, and striae indicate atrophy. Sun damage and wrinkles in the décolletage should be noted, as well. The pinch test can also be used to evaluate for elasticity, as well as the traditional 1 inch (2.5 cm) of breast glandular tissue to cover an implant. If patients with minimal glandular ptosis but poor elasticity receive a circumareolar lift, they will be doomed to bottom out once the implant weight asserts itself.
Degree of Ptosis
The surgeon must evaluate pseudoptosis (glandular ptosis) and ptosis of the NAC. There are more nuances than the classic grading system of mild/moderate/severe ptosis defines. 10 Recognizing these subtleties and patient specific factors (skin type, chest wall length, etc.) helps determine the best type of mastopexy to perform.
Volume Assessment
Bra size is subjective. Sizes vary between bra manufacturers: for example, European bras are sized much smaller than bras manufactured in the United States. Many women also do not understand the relationship between base diameter and cup size. For example, a broad-chested woman may want an A or B cup, but this is an anatomic impossibility because her wide base size precludes a small cup size. Showing bras to the patient helps illustrate this. Furthermore, women often wear the incorrect bra size to accommodate redundant skin with a larger cup or band size. They may also wear a smaller cup size to push the breasts up, or they may refuse to increase the band or cup size because of a reluctance to wear a bigger number.
As an aid in evaluating breast volume without the impact of ptosis, paper tape is used to simulate the mastopexy by taping the breasts “up” (Fig. 9‑4). At this time, the surgeon can re-emphasize skin elasticity, skin type, skeletal issues, NAC position, and any other asymmetries. Implant sizers with a soft bra are tried on by the patient to demonstrate implant volume. This is critical, because patients often have a false idea of volume and will refer to a “friend’s” implant volume and subsequent bra size without understanding their own preoperative anatomy. The surgeon also explains that the exact implant size is less important than the range, and there is an “artistic license” that the surgeon must have. Patients should not fixate on a specific number. It is perfectly reasonable for patients to have an idea of what volume they will be receiving, but a single size option will “handcuff” the surgeon and compromise the aesthetic result. Ideally the surgeon has an assortment of priles and sizes available. If this is not possible, the surgeon should work with the implant manufacturer to have an adequate range of sizes available for each case.

Summarizing the Procedure for the Patient
At the end of each consultation, review the patient’s unique anatomy and review the proposed surgical plan and implant size range. Take your finger or a marker and draw on the patient the extent and length of scars. Give her the benefit of your experience regarding the unpredictability of hypertrophic scarring and keloidal scarring. Recommend any adjunctive procedures at this time.
9.3 Techniques
9.3.1 Circumareolar Mastopexy
Circumareolar mastopexy is best employed in patients who have good skin quality and minimal glandular ptosis/pseudoptosis and require minimal nipple areolar elevation. The planned elevation should be 1.5–2 centimeters or less. 11 The patient is marked in a standing position, placing the nipple 1–2 cm above the IMF.
The operating table should be tested to verify 90° flexion before the patient enters the room. The patient must be placed symmetrically on the table with shoulders and hips aligned. Poor alignment can result in an iatrogenic asymmetry when the patient is placed in a sitting position. Procedures can be effectively done with monitored anesthesia care (MAC) or general anesthesia with laryngeal mask airway (LMA) versus endotracheal tube (ETT) depending on the preference of the anesthesiologist. Our preference is general anesthesia with an ETT to allow muscle relaxation when the pectoralis is elevated. A long circuit is required to enable the patient to be placed in a sitting position during the procedure. Intravenous antibiotics are administered, and sequential compression devices (SCDs) are applied. After induction of anesthesia, the arms are adducted, flexed gently at the elbow, and placed across the abdomen. Elbow pads are used, and a sheet with tape is then used to secure the arms (Fig. 9‑5). This prevents unnecessary stretching of the pectoralis and better simulates the expected postoperative position of the implants. Note that if liposuction of the axilla is planned, the arms are placed abducted on padded arm boards and secured in place with 6-inch Ace wraps (3M, St. Paul, MN). The chest is prepped with povidone-iodine and then draped in the standard sterile fashion.

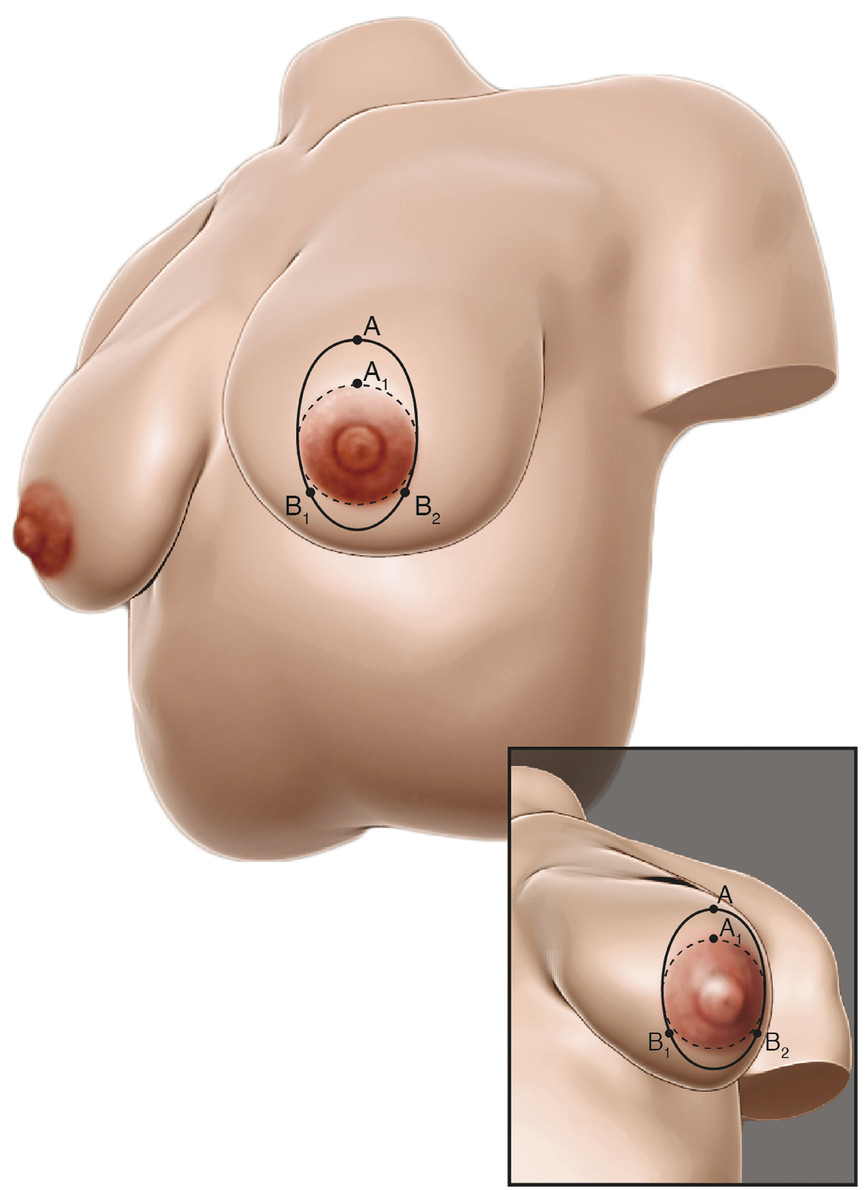
In all mastopexies, the surgeon must have a fixed point on which to base the skin resection. The superior aspect of the planned new areolar position is this fixed A point, and it is predetermined at the time of marking with the patient standing (Fig. 9‑6). The extent of the circumareolar skin excision is determined intraoperatively with tailor tacking and temporary skin staples. The final skin excision, however, occurs after the implant has been placed. A cookie cutter template is used to mark the areola size, which is between 4 and 5 cm, based on the patient’s breast diameter to maintain appropriate proportions. A solution of 0.5% lidocaine with 1:200,000 epinephrine is injected at the site of the incision and as a local field block. At the end of the procedure, this block is repeated with 0.25% marcaine with 1:200,000 epinephrine. The intraareolar incision is made into, but not through, the deep dermis with the breast under tension. The tension applied by the surgical assistant to the breast must be the same on each side to prevent asymmetries between areolar sizes. The breast parenchyma is entered between 3 and 9 o’clock, preserving adequate blood supply to the NAC. Dissection proceeds meticulously with electrocautery. The vast majority of implants are placed in the subpectoral plane, superiorly covered by the pectoralis major muscle and inferiorly subglandular. Exceptions are patients who present for secondary surgery to address size change and ptosis with previously placed subglandular implants without capsular contracture or rippling. Body builders are another example of patients who may be candidates for subglandular placement. Avoid blunt dissection or the avulsion of muscle from the rib cage, as this leads to an increase in bleeding and postoperative pain. 6 Avoid extensive lateral dissection and overdissection of the pocket. When necessary, correct for constricted IMFs by dissecting more inferiorly to lower the fold. After completion of dissection and inspection for hemostasis, sizers are utilized to determine the appropriate final implant size. The mastopexy is then tailor-tacked, and the implant selection is finalized. The authors use smooth gel implants given the association of textured implants with breast implant–associated anaplastic large cell lymphoma. 12
After the implants are placed, a small crescent of breast tissue may be resected inferiorly to plicate redundant breast tissue internally to assist with glandular ptosis. The pocket is irrigated copiously with triple antibiotic solution (cefazolin, bacitracin, gentamicin), and the patient’s chest is again prepped with povidone-iodine. Povidone-iodine is placed directly in the pocket, as well. The surgical assistant partially opens the implant package and bathes the implant in the triple antibiotic solution combined with povidone-iodine. Gloves are changed. Then the permanent implants are placed, minimizing any contact between the prepped skin and the implant. The breast issue is then reapproximated with 4–0 absorbable braided sutures (Vicryl, Ethicon, Bridgewater, NJ). The mastopexy skin resection is then tailor-tacked with staples and finalized by placing the patient in the sitting position. After any needed adjustments are made, the patient is placed in the supine position to complete the final skin excision. The areola is then closed with a 3–0 polytetrafluoroethylene (PTFE) suture (Cytpolast, Osteogenics Biomedical, Lubbock, TX) on a Keith needle in a “purse-string” fashion, paying careful attention to start the suture deep in the dermis and end deep. The knot is prepped with povidone-iodine prior to burying it. The final layer is a 5–0 monofilament absorbable suture (Monocryl, Ethicon, Bridgewater, NJ) run subcuticularly. Approximate the incision as needed with 6–0 simple interrupted sutures using permanent suture (nylon or polypropylene). If the patient has not had previous surgery, Mastisol liquid adhesive (Ferndale Laboratories, Ferndale, MI) and Steri-Strips (3M, St. Paul, MN) are applied. In secondary cases, skin adhesive is avoided because of numerous allergic reactions. Pleating of the areolar edge usually resolves within 6 months. The patient is placed in a soft surgical bra on the day of surgery with gauze padding placed lightly over the incisions.
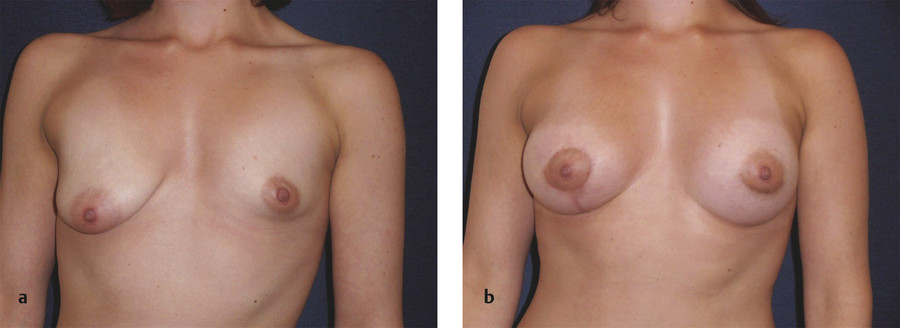
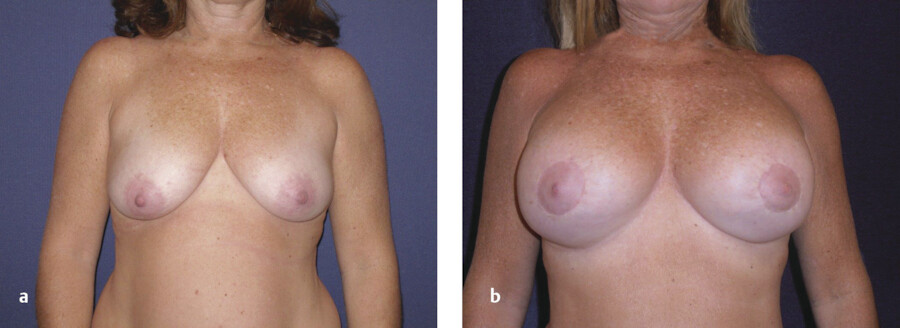
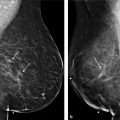
Two cases are illustrated in Fig. 9‑7 and Fig. 9‑8.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


