11 Internal Bra Technique in the Breast with Poor Soft Tissue Support
Summary
The chapter discusses use of a mesh scaffold “internal bra,” which has been previously described for mastopexy alone. These constructs also have utility in addressing breast implant malposition or for patients desiring substantial upper pole fullness, especially when there is a low inframammary fold crease or poor soft tissue support. Examples include AlloDerm (BioHorizons, Birmingham, AL), or other acellular dermal matrices, and GalaFLEX (poly-4-hydroxybutyrate, or P4HB; Galatea Surgical, Lexington, MA) bioresorbable mesh. Combining mesh with breast shaping and implants can help obtain a durable aesthetic result attributable to a resistant support system. One should be cognizant of the complexity of these internal bra techniques, especially in cases of severe tissue weakening, including the risk for delayed healing, implant extrusion, skin necrosis, residual asymmetry, and need for a secondary procedure to fine-tune results. However, when executed correctly in the right indications, the use of surgical mesh in revisional aesthetic surgery can yield safe, reliable, and excellent outcomes, particularly for the patient seeking upper pole volume and improved cleavage when the soft tissues are too weak to provide requisite support.
11.1 Introduction
One of the limitations of any cosmetic breast procedure is the patient’s baseline anatomy, including the quality of the patient’s skin and breast tissue (soft tissue support) and the overall position of the inframammary fold (IMF) crease. In patients with poor soft tissue support, achieving and maintaining upper pole volume can be challenging. What ultimately holds up the breast in any cosmetic procedure is the quality of the patient’s tissue, despite techniques to tighten loose skin or manipulate an existing capsule. The position of the IMF crease also helps determine how high the augmented breast sits on the chest wall. What can a plastic surgeon do to achieve desired upper pole fullness in cases where there is evidence of poor soft tissue support, 1 there is a low IMF crease (i.e., tall chest wall height), 2 or both? Although internal capsulorraphy is a well-established option, the authors find this approach limited in cases of suboptimal soft tissue support (poor tissue quality), especially when the patient is opting for larger or heavier implants.
Single-stage mastopexy–augmentation presents unique challenges in aesthetic breast surgery, in attempting simultaneously to counterbalance the gravitational forces of the breast implant with skin and parenchymal reshaping to correct ptosis. 1 , 2 , 3 The additional variable of poor underlying soft tissue support—whether secondary to age, repeated surgery, postpartum changes, or weight loss history—only increases the potential for recurrent ptosis and rates of complications. 4 , 5
Use of de-epithelialized dermoglandular flaps for breast reshaping formed the basis for Sampaio Góes’ periareolar approach, described in 1989. 6 However, in following patients longitudinally, surgeons noted that this tissue construct was inadequate in preserving an optimal shape of the remodeled breast. Thus, an internal support construct was deemed necessary for stability and prevention of soft tissue relaxation, which enables increases in breast base and areolar diameter. Sampaio Góes began to utilize mesh placed in between the external, intact skin envelope and the de-epithelialized internal layer. 7 The innovation helps provide a longer-lasting aesthetic result that is reliant on a more resistant support system. The mesh maintains the ideal gland position postoperatively and facilitates tissue fixation, opposing gravitational forces on the breast.
Internal bra meshes have been fabricated from different kinds of materials. For instance, some surgeons have used acellular dermal matrices (ADMs) for internal bras. Polyglactin 910 was among those absorbable meshes first described and was found to preserve aesthetic results for up to 2 years, after which partial loss was reported. Thereafter, mixed mesh composed of polyglactin 910 and polyester was utilized, showing durable results for several years’ follow-up. 8 Other described mesh polymers include Vypro, made of polypropylene and polyglactin (Ethicon, Bridgewater, NJ); UltraPro, made of polypropylene and Monocryl (poliglecaprone 25; Ethicon, Bridgewater, NJ); SERI scaffold, made of raw silk protein filaments (Sofregen Medical, Medford, MA); and more recently GalaFLEX, made of poly-4-hydroxybutyrate (P4HB; Galatea Surgical, Lexington, MA). 9 Importantly, nonabsorbable meshes have not directly shown complications attributable to their inherent material, which heuristically is sensible, as routine suture threads similarly are well-tolerated in general.
11.2 Patient Selection
Indications for use of the internal bra technique for augmentation mastopexy include but are not limited to
Severely loose skin with poor soft tissue support; tissue quality unable to support an implant in the desired position (upper pole fullness).
Low-riding breasts with very low IMFs or tall chest wall height.
Bottomed-out breasts with low IMFs.
Fold restoration following a total capsulectomy of a severely calcified breast implant capsule.
Implant malposition (lateral or inferior malposition).
Symmastia reconstruction.
Breast asymmetries (fold asymmetry).
Combined with mastopexy, use of a mesh scaffold with an internal bra technique facilitates breast elevation, raises the patient’s IMF, and addresses lateral malposition. In milder cases of ptosis, a mastopexy may not be warranted. A mastopexy also may not be warranted in the case of a younger patient seeking upper pole volume with good tissue quality but very low IMF crease position (i.e., tall chest wall height)
In cases with significant asymmetries of the breasts as well as IMFs, coupled with extensive prior breast surgeries, patients must be counseled extensively regarding their challenging anatomy as well as on surgical risks, limitations of the procedure, and possible need for secondary revisions. Even with the senior author’s extensive experience with internal bra technique procedures in revisional augmentation mastopexy, the authors advise all patients of an up to 20% chance of needing a secondary procedure to refine the result. It is important to educate the patient that the internal bra technique is not merely an augmentation mastopexy; it is an advanced technique to essentially reengineer breast anatomy. Often, surgeons are addressing multiple variables in one case: implant size, lateral malposition, inferior malposition, fold asymmetries, excess skin, ptosis and nipple position, and symmetry. Hence, the patient must be made aware of the need to fine-tune results, which should be part of a detailed informed consent process. Furthermore, we strongly advise including a separate consent for the surgeon’s choice of surgical mesh/ADM for proper informed consent.
11.3 Patient Assessment and Markings
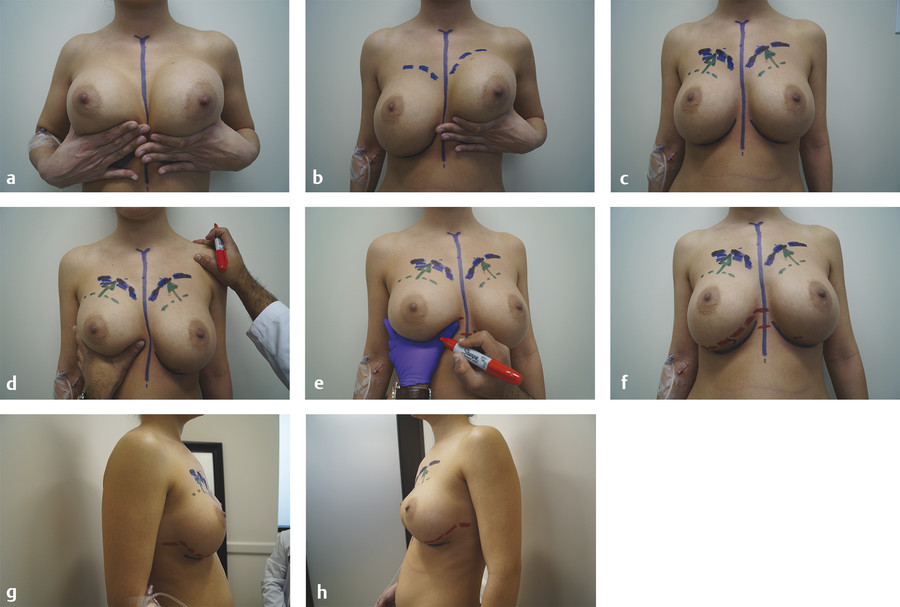
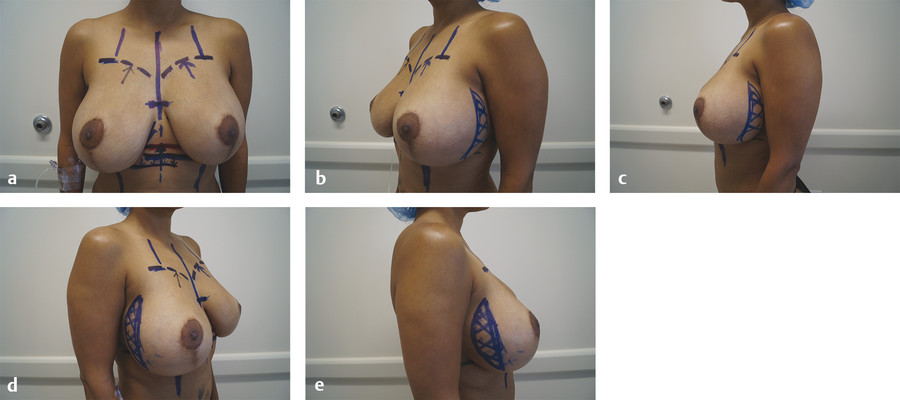
The authors routinely mark the patient midline and current IMF crease. All markings are done in the upright position, with the patient observing all markings in the mirror. During the initial consultation, we document any fold asymmetries that may exist at baseline. It is important to re-highlight baseline fold asymmetries to the patient during preoperative marking. We advise the patient to use her hands to mimic the effect of a push-up bra to demonstrate how she wants her breasts to sit on her chest wall. While the patient is pushing her current/old implants up demonstrating her desired “cleavage takeoff point,” or the point at which the upper pole of breast volume begins, it is important to mark out this new upper pole border (Fig. 11‑1). Now the surgeon must estimate the base width of the new implant and estimate where the neo-IMF should sit. A key question is to what extent the surgeon needs to raise the IMF? It is important to mark out the medial and lateral borders of the desired neo-IMF. These markings will be utilized intraoperatively and will help to ensure symmetry when reconstructing or raising the patient’s IMF (Fig. 11‑2).
11.4 Surgical Technique
11.4.1 Considerations
Local anesthetic is infiltrated along the patient’s IMF and around any anticipated mastopexy incisions to aid in hemostasis and facilitate pain control. In secondary cases, an IMF crease approach is typically utilized. If the patient presents with severe loose skin that will require a circum-vertical or full mastopexy, a generous 4- to 5-cm vertical incision along the breast meridian, below the nipple areola complex (NAC), can be utilized for access to the patient’s original implants; this incision will later be buried into the subsequent mastopexy. In cases that will require only a periareolar mastopexy, the authors have utilized an IMF crease approach, occasionally utilizing a limited inferior periareolar access incision if needed.
11.4.2 Planning the Neo-IMF Crease Position
The degree to which the IMF will need to be elevated is estimated based on preoperative markings, and the IMF incision marked appropriately to minimize visible scarring. Preoperatively, the authors recommend having the patient demonstrate her desired result: have the patient show you where she wants the upper border of her breast to be. Then, based on this position, mark where you think the neo-IMF crease needs to be to achieve the desired result (Fig. 11‑1).
11.4.3 Management of the Breast Capsule in Revisional Cases
If the capsule is benign and nonpathologic, a total capsulectomy is not warranted. If there is lateral malposition present, a lateral capsulorraphy can be performed. The surgical mesh or ADM product can also be utilized to prevent lateral malposition as well. A total capsulectomy is indicated, by contrast, when capsules demonstrate thickening or calcification. In some revisional cases, the IMF crease and structure are notably low on the chest wall and occasionally extend into the upper abdominal space. In severe cases of capsular contracture and/or in cases of poor soft tissue support or quality, the patient can be left with a weakened IMF when the capsule is removed from the inferior gutter of the implant pocket. In these cases, the patient may be at increased risk for bottoming out or inferior malposition, especially if a larger implant is placed. Use of the internal bra technique is an option in these cases to restore the integrity of the fold and/or raise its position on the chest wall.
11.4.4 Mesh Application
On each side, the chest wall is marked above the current IMF, delineating where the mesh scaffold is to be anchored. If lateral malposition is present, the chest wall can be additionally marked where the mesh is to be anchored laterally to correct lateral malposition. If a lateral capsulorraphy has been performed, simply placing the surgical mesh as an overlay can suffice. Mesh scaffold is selected and soaked in antibiotic solution per manufacturer and product specifications. Intraoperative paper templates may be used to estimate mesh size needed to accommodate the contour of the patient’s anticipated new implants. It is important to remember the natural curvature of the new implant to be placed. If the mesh is too small to accommodate the curvature of the implant, this can blunt and distort the lower pole of the breast. The choice of mesh is otherwise prepped per industry recommendations, including any irrigation fluid soaks and washes to clear retained preservative, if needed.
At this time, the authors’ preferred surgical mesh is GalaFLEX, made of poly-4-hydroxybutyrate (P4HB). The advantages of GalaFLEX include but are not limited to (1) use of a long-standing safe suture material that dissolves over 18–24 months, (2) relatively low cost compared to other ADM or surgical mesh products, (3) reliable safety profile with low risk of extrusion, and (4) rapid integration and adherence to surrounding tissue.
Related posts:
 7 Preoperative Evaluation of Patients with Macromastia and Ptosis
7 Preoperative Evaluation of Patients with Macromastia and Ptosis
 12 Reduction Mammaplasty
12 Reduction Mammaplasty
 8 Mastopexy Techniques—Basic Principles
8 Mastopexy Techniques—Basic Principles
 10 Management of the Massive-Weight-Loss Breast
10 Management of the Massive-Weight-Loss Breast
 9 Augmentation and Mastopexy—Basic Principles to Develop a Treatment Plan and Technical Pearls
9 Augmentation and Mastopexy—Basic Principles to Develop a Treatment Plan and Technical Pearls
 22 Nipple Areolar Procedures and Aesthetics
22 Nipple Areolar Procedures and Aesthetics
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


