22 Nipple Areolar Procedures and Aesthetics
Summary
An integral part of breast surgery is to preserve or re-create the natural appearance of the breast. Attaining quality aesthetic results after breast surgery is an important factor in physical appearance and psychological body image, which affects patients’ quality of life after breast surgery. A key factor in the aesthetics of breast surgery is the preservation, recreation, and reconstruction of the nipple areolar complex (NAC). Factors that affect the aesthetics of the NAC include location, orientation, angulation, size, shape, color, and symmetry. To improve aesthetic results after breast surgery, several procedures have been developed to address the NAC. This chapter will review the anatomy, embryology, and physiology of the NAC, including the milk-secreting system, lymphatic drainage, innervation, and vascular supply. Furthermore, it will discuss the “ideal breast,” describing the proportions and relative placement of the NAC on the breast that is associated with the greatest aesthetic result in the literature. Finally, primary pathology of the NAC, including inverted nipple and nipple hypertrophy, are discussed with surgical approaches for correction.
22.1 Introduction
An integral part of breast surgery is to preserve or re-create the natural appearance of the breast. Attaining quality aesthetic results after breast surgery is an important factor in physical appearance and psychological body image, which affects patients’ quality of life after breast surgery. 1 A key factor in the aesthetics of breast surgery is the preservation, re-creation, and reconstruction of the nipple areolar complex (NAC). 2 , 3 Several factors affect the aesthetics of the NAC, including location, orientation, angulation, size, shape, color, and symmetry. Several primary pathologies of the NAC affect its aesthetic appearance, including inverted nipple and nipple hypertrophy; these have been studied in order to develop better surgical techniques for correction.
22.2 Nipple Areola Complex Anatomy
22.2.1 Embryology, Structure, Development
The NAC is a central breast structure that consists of the areola, which is distinguished from the rest of the surrounding breast tissue by its distinct change in skin pigment, as well as the nipple itself. The physiologic purpose of the NAC is to deliver milk, produced in the mammary glands of the breast, to an infant. The normal color of the areola can range from lighter to darker skin tones and can span the spectrum of pink to red to brown or nearly black, depending on the underlying skin color of the individual. Typically it is paler in those with lighter skin tones and darker in those with darker skin tones, but the pigment differs from that of the surrounding breast skin. Many believe this color difference makes it more visible and draws the attention of an infant attempting to breastfeed.
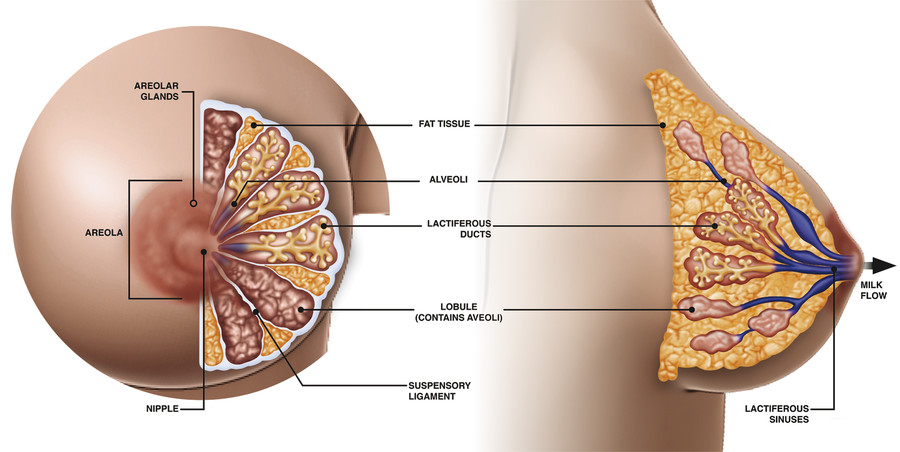
The breast tissue and makeup can be divided into parenchymal tissue and stromal tissue. In utero, the parenchymal tissue forms a system of branching ducts, which develop into secretory acinar cells and eventually form the lactiferous ductal system. The stromal tissue develops into the fatty breast tissue, which provides an environment for proper development of the ductal system. This system slowly develops in utero in conjunction with proliferation of mesoderm. The proliferation of mesoderm causes eversion of the nipples at the skin level shortly after birth. This is the same time in development when the change in pigmentation of the NAC occurs. Further development of erectile tissue within the NAC causes nipple protrusion. 4 In the mature breast the NAC contains Montgomery’s glands, or areolar glands, which are large sebaceous glands that secrete a lubricating fluid to prevent chafing during breastfeeding. 5 These glands then open at Montgomery’s tubercles, which are small raised papules on the areola. The milk-secreting system consists of glandular lobes containing cells that secrete milk into lactiferous sinuses, which empty into the lactiferous ducts, which secrete the milk through the nipple when stimulated (Fig. 22‑1). 5 , 6 It is important to note that the overlying skin is continuous with the ducts, which has oncologic implications and allows malignancy to travel from within the ducts to the overlying skin.
22.2.2 Lymphatic Drainage
There are four major lymphatic drainage pathways of the breast, including two deep lymphatic systems and two superficial lymphatic systems. The primary lymphatic drainage of the NAC is Sappey’s plexus, a complex, subareolar lymphatic system that is in communication with one of the superficial drainage pathways. This superficial plexus then communicates with one of the deeper lymphatic systems, the glandular plexus, which runs with the lactiferous ducts. These lymphatic pathways eventually drain into the axillary lymph node system. The skin and glandular tissue have the same embryonic origin and therefore the same lymphatic drainage pathway. This is what enables breast surgeons to inject subcutaneous radiotracer or methylene blue in the subareolar or periareolar tissue and trace this to the axillary sentinel node in breast cancer surgery. 7
22.2.3 Innervation
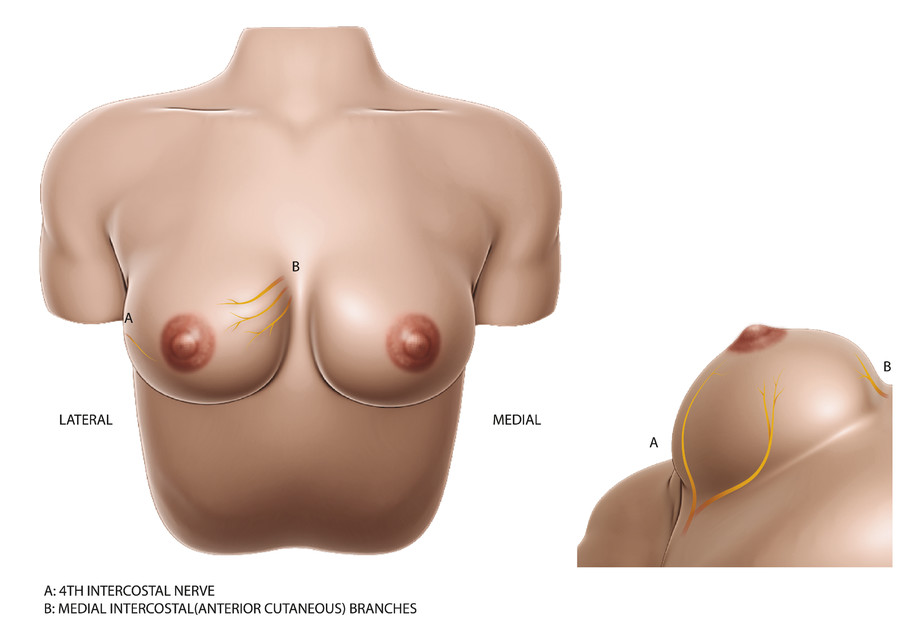
The nerve supply to the NAC is of particular importance, as the sensitivity plays a major role in morbidity and patient satisfaction after breast surgery. In several cadaveric studies, the nerve supply of the NAC has been dissected in order to understand its cutaneous innervation better. 8 , 9 The majority of the contribution to the sensory innervation of the NAC comes from lateral and anterior cutaneous branches of the second through fifth intercostal nerves (Fig. 22‑2). These studies have demonstrated that the most consistent of these contributions originates from the fourth intercostal nerve, specifically the lateral cutaneous branch; however, the anterior cutaneous branches of the third and fourth intercostal nerves were also highly consistent.
22.2.4 Blood Supply
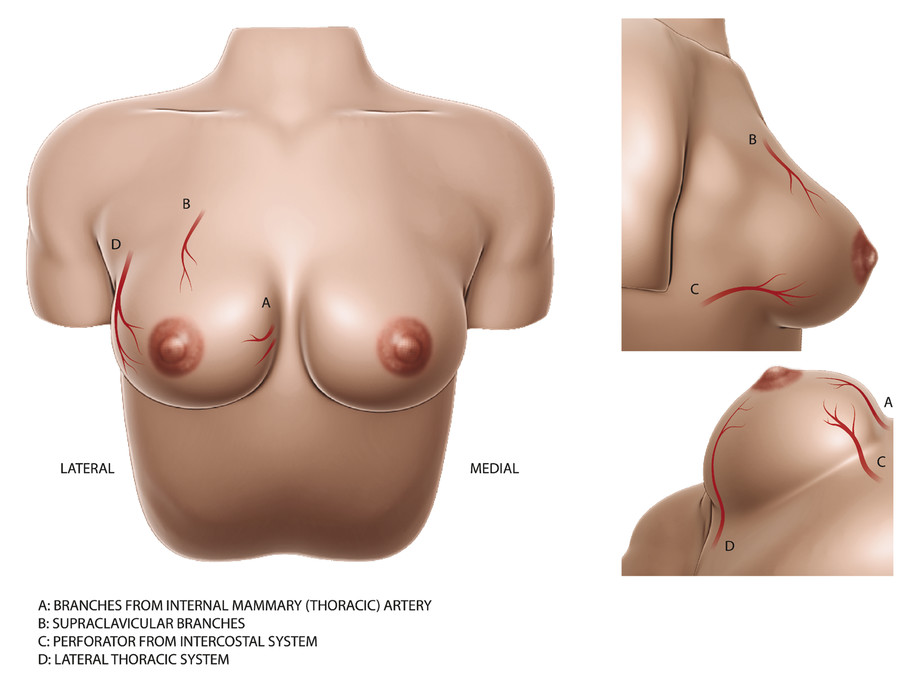
The blood supply to the NAC generally has contributions from the internal thoracic artery (internal mammary artery), intercostal arteries, and lateral thoracic artery (Fig. 22‑3). Studies have been made in order to understand better the contribution of each arterial system to the NAC so as to guide better surgical techniques. In one particular cadaveric study, van Deventer dissected the arterial anatomy of 27 female breasts and found that the most consistent contribution to the NAC was the internal thoracic artery (100%), followed by the anterior intercostal arteries (74%) and the lateral thoracic artery (70%). 10 In a separate study that reviewed thoracic computed tomography (CT) angiograms to identify arterial supply to the NAC, Stirling et al found that perforating branches from the internal thoracic artery contributed to NAC blood supply in 81.8% of patients, followed by lateral thoracic contribution in 23.5% of patients and anterior intercostal artery contributions in 15.9% of patients. 11 Other studies have also described minor contributions directly from other arterial systems, including the axillary artery and posterior intercostal arteries. Given that the NAC receives blood supply from multiple sources, one would think it is a highly vascularized structure with collateral supply if needed during surgery. Iris et al analyzed breast magnetic resonance imaging (MRI) in order to understand with what frequency the NAC was receiving blood from multiple zones or arterial systems rather than from one arterial system. They found that in 58% of patients, blood supply came from one general breast zone (medial, lateral, central, superior, or inferior), with the great majority coming from medial perforating vessels. Only 42% of patients had NAC blood supply come from multiple zones, with the vast majority being medial and lateral perforating branches. 12 This suggests that the majority of the blood supply to the NAC comes from medial perforating vessels from the internal thoracic artery, as well as some contribution from lateral perforating vessels from the long thoracic artery and intercostal arteries. Knowledge of the origin and direction from which the NAC receives its blood supply can better direct surgical approach and dissection in order to avoid disrupting NAC perfusion, which could lead to necrosis and nipple loss during surgery.
22.3 The Ideal Nipple Areola Complex
22.3.1 General Principles
In regard to reconstruction and preservation of the NAC, one must keep several general principles in mind to have an aesthetically successful surgery. First and foremost, it is important to remember that every patient is different and will have certain preferences for the desired outcome. Therefore, it is important to discuss this and set these expectations with the patient prior to surgery. 13 Some texts have described a technique in which the patient is able to partake in the positioning of the NAC by using markers or stickers to designate possible placement in the preoperative setting. This allows the patient to see several possible positions and choose what they believe is the most aesthetically pleasing prior to surgery. The patient and the surgeon can use this technique to find the ideal NAC placement and proportions together, which optimizes aesthetic outcomes. 4
It should also be noted that any aesthetically pleasing outcome will incorporate and maintain symmetry between the breasts. This symmetry should incorporate parameters including color, texture, size, projection, angulation, placement, and relative proportions. In a unilateral reconstruction, the contralateral breast and NAC should be used as a template for the reconstruction. In bilateral reconstruction, symmetry of the NAC should be of highest consideration. 13
Related posts:
 20 Evaluation and Treatment of Congenital Breast Deformities
20 Evaluation and Treatment of Congenital Breast Deformities
 24 Breast Implant Illness
24 Breast Implant Illness
 21 Transgender Breast Surgery
25 Appendix: Update on Breast Implant–Associated Anaplastic Large-Cell Lymphoma
21 Transgender Breast Surgery
25 Appendix: Update on Breast Implant–Associated Anaplastic Large-Cell Lymphoma
 23 Marketing a Cosmetic Breast Surgery Practice through Social Media Outlets
23 Marketing a Cosmetic Breast Surgery Practice through Social Media Outlets
 11 Internal Bra Technique in the Breast with Poor Soft Tissue Support
11 Internal Bra Technique in the Breast with Poor Soft Tissue Support
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


