48 Latissimus Dorsi Flap Reconstruction
Summary
The latissimus dorsi flap remains one of the most useful autologous flaps for breast reconstruction and is particularly useful in salvage reconstruction. Its robust, consistent blood supply and generous proportions make it an ideal flap for reconstruction of the female breast after mastectomy for breast cancer. It often requires an implant for adequate volume.
Key Teaching Points
Design skin island along the back fat roll in Lange’s lines.
Maintain the skin island in contact with the muscle throughout.
Keep skin island width less than 9 cm if possible to reduce closure tension.
Denervate the muscle to prevent animation deformity of the flap.
The serratus fat pad aids in guiding posterior dissection.
Drain the donor site long term to prevent seroma.
Once transposed anteriorly, anchor the lateral muscle to the chest wall to prevent implant dislocation back into the donor site.
Place the muscle in the prepectoral position within the mastectomy defect.
A small piece of acellular dermal matrix can be incorporated into the reconstruction to reduce capsular contracture.
48.1 Observations
Prior to the 1970s, implant-based reconstruction was the only modality available and the results were abysmal. Radovan’s introduction of tissue expansion in 1976 revolutionized implant reconstruction but did little to improve the quality of skin available for reconstruction. The resurrection of Tanzini’s latissimus dorsi (LD) musculocutaneous island flap (first described in 1906) began another revolution in the late 1970s, introducing the concept of autologous replacement or augmentation of chest wall skin. At that time many women with breast cancer had undergone radical mastectomies, and this flap was the most reliable source available for supplementing missing skin, replacing the missing pectoralis major muscle, and supplying additional autologous fill. The insertion of a breast implant under the flap was usually necessary to augment breast volume because of the limited tissue available from the muscle and skin island.
With the trend to a more conservative approach to local treatment of breast cancer using breast conservation surgery with irradiation or a modified radical mastectomy, often with skin-sparing incisions and immediate breast restoration, new methods for partial and total breast reconstruction were developed. The introduction of purely autologous tissue breast reconstruction with the transverse rectus abdominus myocutaneous (TRAM) flap and its variants relegated the LD flap to a much less prominent position in breast reconstruction.
LD flap breast reconstruction techniques have evolved along with advances in other methods of breast reconstruction. In recent years, this versatile and reliable flap has undergone a considerable and entirely justified resurgence in popularity. The development of the extended autologous LD musculocutaneous flap, with its potential for harvesting additional volume, has enabled many women to have a totally autologous reconstruction without the need for an implant. Endoscopic harvest of the LD through reduced skin incisions makes partial breast reconstruction possible after quadrantectomy and lumpectomy without adding significant additional scars. The LD muscle and fat can also be harvested with a minimal donor site scar when skin is not a requirement for the reconstruction but additional autologous tissue is needed. Thus, the LD flap is now frequently used as a primary method of reconstruction as well as to supplement other techniques.
While microsurgical techniques have evolved and become more sophisticated, many surgeons favor the latissimus flap for its reliability, ease, and speed of dissection. It is an exceptional procedure for salvage of complex problems. If muscle is not required, a thoracodorsal artery perforator (TAP) flap maybe raised although the lack of muscle compromises the volume of this flap very significantly.
48.2 Indications for Latissimus Dorsi Flap
Lack of anterior mastectomy skin flap surface area.
Poor quality mastectomy skin flaps (radiation or scarring).
Poor candidate for tissue expansion.
Resurfacing the nipple–areolar deficit after skin-sparing mastectomy through circumareolar incisions.
Salvage of necrotic mastectomy skin after skin-sparing mastectomy.
Lack of available abdominal autologous tissue for transverse rectus abdominus myocutaneous (TRAM)/deep inferior epigastric perforator (DIEP) flap.
Salvage of partial abdominal flap necrosis (TRAM or DIEP).
Coverage of chest wall defects after full-thickness resection for radiation necrosis.
Reconstruction of Poland’s syndrome.
Reconstruction of partial mastectomy defects.
48.3 Contraindications to Latissimus Dorsi Flap Reconstruction
Transected latissimus muscle after thoracotomy.
Irreversible damage to the thoracodorsal vascular pedicle.
Patient with unique requirements for preservation of LD muscle—rowing, swimming, climbing, cross-country skiing, etc.
48.4 Anatomical Synopsis
For expanded details see Chapter 47.
48.4.1 Morphology
An asymmetric rhomboid-shaped muscle of the back overlying the posterior ribs and tip of the scapula.
48.4.2 Origin
T6 to T12, lumbar fascia.
48.4.3 Insertion
Medial lip of the intertubercular groove of the humerus.
48.4.4 Blood Supply
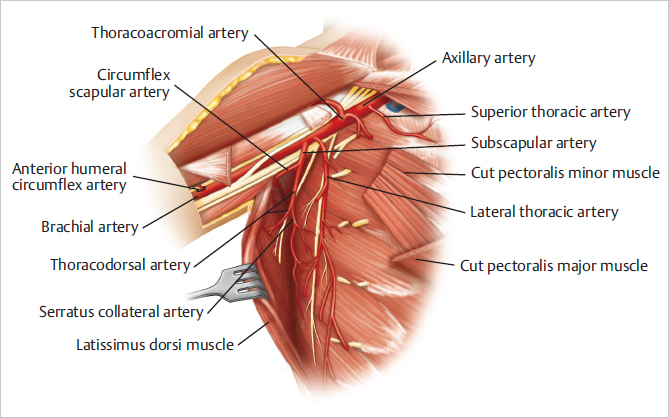
Thoracodorsal branch of the subscapular vessels derived from the axillary artery.
48.4.5 Nerve Supply
Thoracodorsal nerve—root value C6 to C8.
48.4.6 Function
Extension, adduction, and internal rotation of the humerus.
48.4.7 Skin Island Dimensions
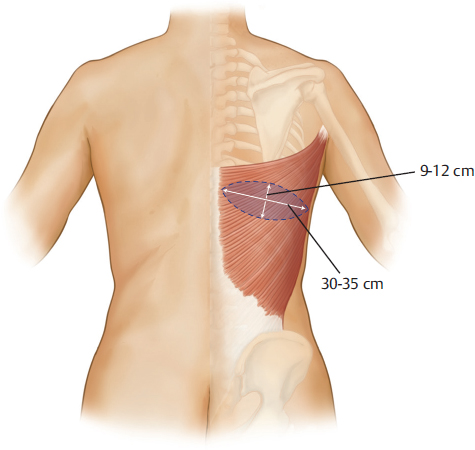
The dimension is measured as 7 × 20 cm average (9–12 cm x 35 cm maximum depending on the patient’s back width) (▶Fig. 48.1).
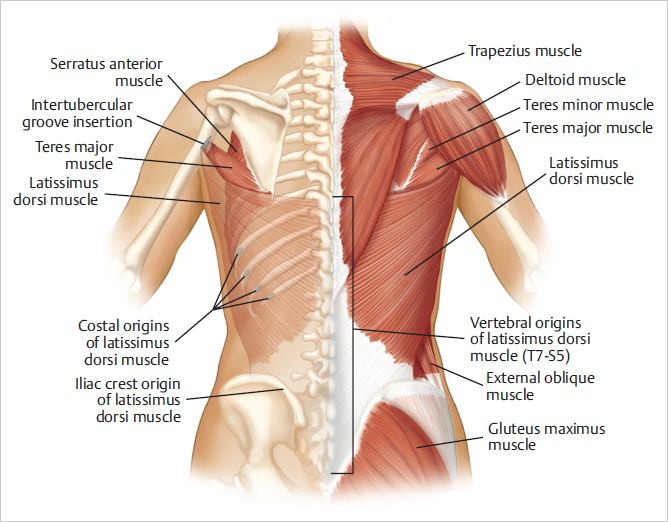
The muscular anatomy of the LD muscle from a posterior view is indicated in ▶Fig. 48.2.
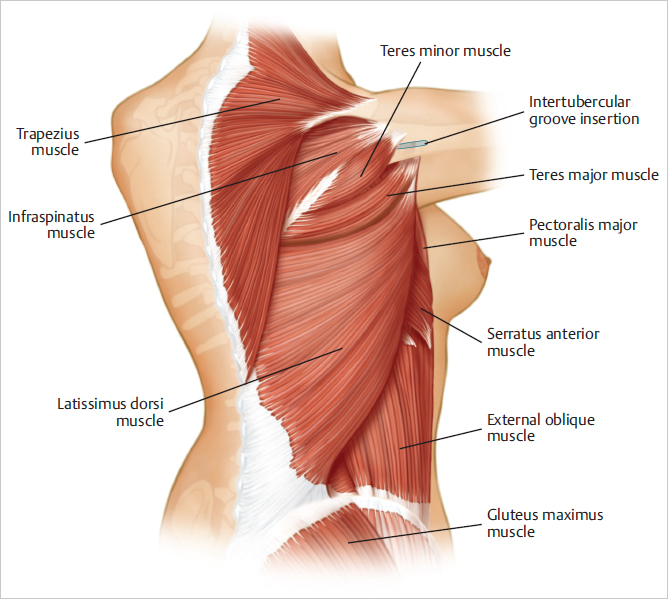
The anatomical relationships of the LD are illustrated in ▶Fig. 48.3.
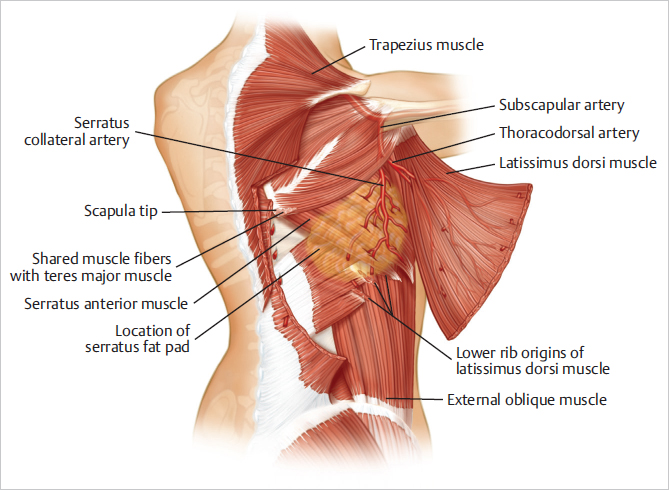
The anatomy of the deep surface of the muscle is shown in ▶Fig. 48.4.
The vascular anatomy of the thoracodorsal pedicle is outlined in ▶Fig. 48.5.
48.5 Patient Assessment and Selection
The best candidates for the LD flap are as follows:
Women with a modified radical mastectomy deformity who have a moderate percentage of body fat.
A full, soft opposite breast with some breast ptosis.
Limited mastectomy site skin for expansion.
Little upper abdominal skin to recruit for tissue expansion or to elevate and advance for lower breast supplementation.
These women often have a redundant roll of tissue in the bra strap line, suitable for harvest with the LD muscle for transfer to the lower portion of the reconstructed breast.
In thin patients, a breast implant is usually needed to restore adequate breast volume. I try to avoid additional tissue expansion where possible. Candidates for totally autologous breast reconstruction with the LD flap have a higher body mass index (BMI) with significant midback fullness that approximates their breast volume requirement. Women with limited tissue requirements, such as those who need upper breast fullness, muscle coverage of a breast implant, or partial breast reconstruction, are also good candidates for an LD flap. It can be used as a microsurgical free flap transfer for breast reconstruction.
48.6 Planning Considerations
48.6.1 The Opposite Breast
If the opposite breast is to be emulated, it is measured carefully to ensure that the tissue added by the flap will provide the same amount of skin cover; a tissue expander or implant can then provide fill. When the opposite breast has some hypertrophy or ptosis, the modified opposite breast is the model for breast reconstruction. The reconstructive surgeon must know how much skin cover will be left after the opposite breast correction and plan to replace a sufficient amount of skin with the LD flap.
The images of ▶Fig. 48.6 depict the measurement of the chest wall on the mastectomy site compared with that on the contralateral side to be matched by the reconstruction.
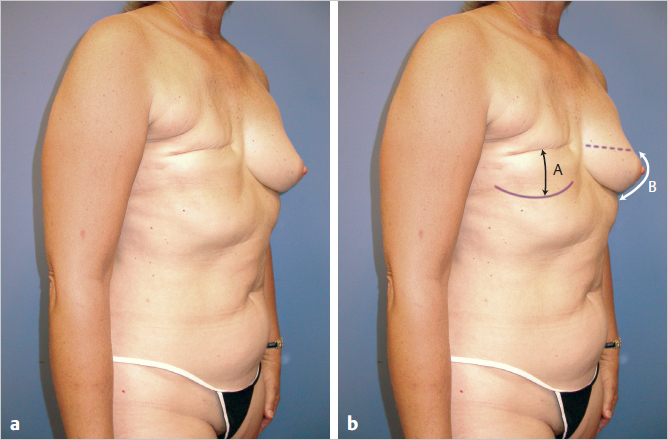
Technical Pearl
The difference in vertical measurement between the two breasts reflects the diameter of the latissimus skin island required to bridge the deficit created by mastectomy. Volume is provided by the implant or extended autologous harvest alone. This assumes that the opposite unoperated breast is the goal to be attained by reconstruction.
Because an implant is usually needed for an LD flap reconstruction, it is sometimes advantageous to incorporate an implant (or tissue expander) in the plan for correction of the opposite breast, particularly if the latter is hypoplastic or displays involutional atrophy. This approach gives the surgeon additional latitude and more control of final breast appearance.
The opposite natural breast is often fuller inferiorly and laterally that can be achieved with tissue expansion alone. Consequently, the LD flap should be positioned low and laterally to provide volume where it is most needed.
Recognizing that the footprint of the opposite breast has three dimensions, the surgeon must replace a sufficient volume of skin vertically, horizontally, and anteriorly to create a natural breast contour with forward projection.
48.6.2 Skin and Subcutaneous Tissue
The thickness, mobility, and texture of the remaining mastectomy skin are evaluated. Skin grafts or radiation changes must be considered when planning the flap to ensure complete muscle cover over the implant, thus avoiding later exposure from skin thinning or ulceration. When a skin graft covers the site of the mastectomy, it should be removed and replaced with the skin island of the latissimus flap.
Technical Pearl
No flap exhibits wider variation in skin thickness, pliability, and elasticity than the latissimus flap. The skin of the back is extremely thick, and in some women it has very little elasticity and ability to stretch while in others it is very soft, compliant, and easily stretched. These physical attributes of the latissimus dorsi flap skin island have to be borne in mind when planning reconstruction.
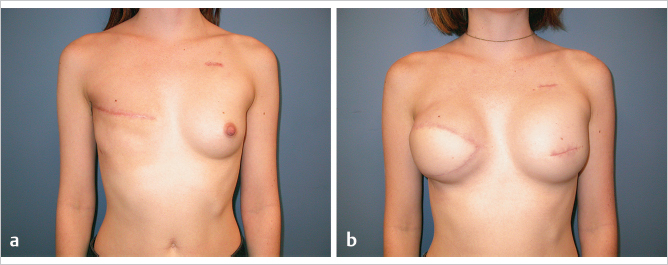
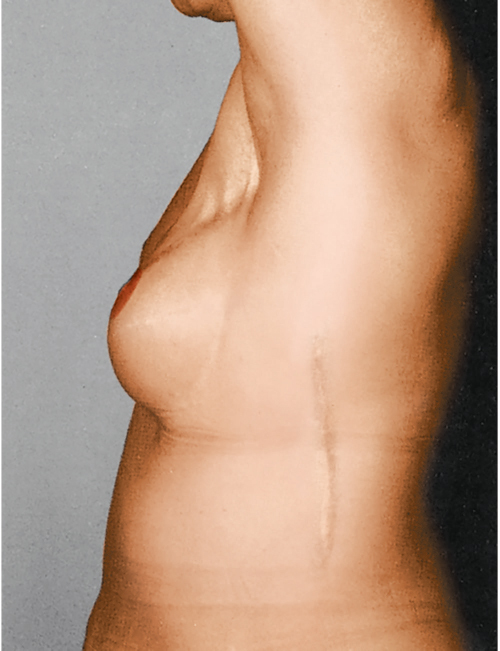
This 23-year-old woman was diagnosed with right breast carcinoma and underwent mastectomy with chemotherapy followed by radiation therapy. Because she was found to have the BRCA1 oncogene, she elected to undergo a simple mastectomy on the left side with immediate implant reconstruction, coupled with an LD flap delayed reconstruction on the right with implant placement to be performed concurrently. She was very thin, requiring a significant skin island to achieve adequate surface area, and her TRAM donor site was deemed inadequate. Her back skin was soft and pliable. For this reason, a latissimus skin island measuring 7 × 14 cm was used without requiring expansion. She is shown before nipple reconstruction (▶Fig. 48.7).
The chest skin is also evaluated to determine whether it can be safely elevated. Large defects may indicate the need for a TRAM/DIEP flap, which provides a larger skin island than a latissimus flap ever can. If heavily irradiated, the skin may need to be replaced. If the mastectomy skin flaps are intact but thin, most likely they have been effectively “delayed,” and it is safe to elevate them, especially if they are placed back onto well-vascularized LD muscle. Flaps that are paper thin because of the mastectomy and postoperative radiation therapy should be replaced with healthy, well-vascularized skin.
Ordinarily the normal “ideal” breast measures 20 to 22 cm from clavicle to nipple and an additional 7 cm to the inframammary crease. Measurements from midline to nipple and nipple to midaxillary line indicate the flap volume that is needed to replace missing skin in the horizontal direction. The breast width is as important as the vertical dimension.
Technical Pearl
With primary back donor site closure, the practical limits of the latissimus dorsi skin island are usually 30 to 35 cm long and 9 to 12 cm wide. Ordinarily, the flap is 7 to 9 cm wide and 20 to 25 cm long (▶Fig. 48.1).
When the requirements of the LD flap are greater than can be provided with primary elevation, preexpansion of the LD flap is an option. With this strategy, flaps with skin islands from 10 to 20 cm wide can be developed with subsequent primary closure of the back donor site. This is difficult for the patient to tolerate and is rarely performed.
48.7 Evaluation of Back Fat for Extended Autologous Latissimus Dorsi Flap
A natural extension of the traditional LD flap is the extended autologous procedure in which additional subcutaneous tissue harvested with the elevated flap provides extra autologous tissue for breast reconstruction through a standard lower back ellipse.
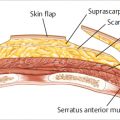
Subcutaneous fat is harvested at or immediately beneath the level of Scarpa’s fascia and is beveled peripherally onto the muscle.
Subcutaneous fat can be harvested above Scarpa’s fascia, but this thins the overlying skin flap thickness and may result in ischemic necrosis at the donor site.
Fat should not be harvested between the insertion of the muscle and the posterior axillary fold, because this simply adds unwanted bulk in the axilla.
The addition of a fat layer 1 cm thick over a muscle measuring 20 × 15 cm will provide an additional 300 cc of flap volume to the procedure that would be absent in the traditional approach. This can be enough to obviate the need for an implant in many patients.
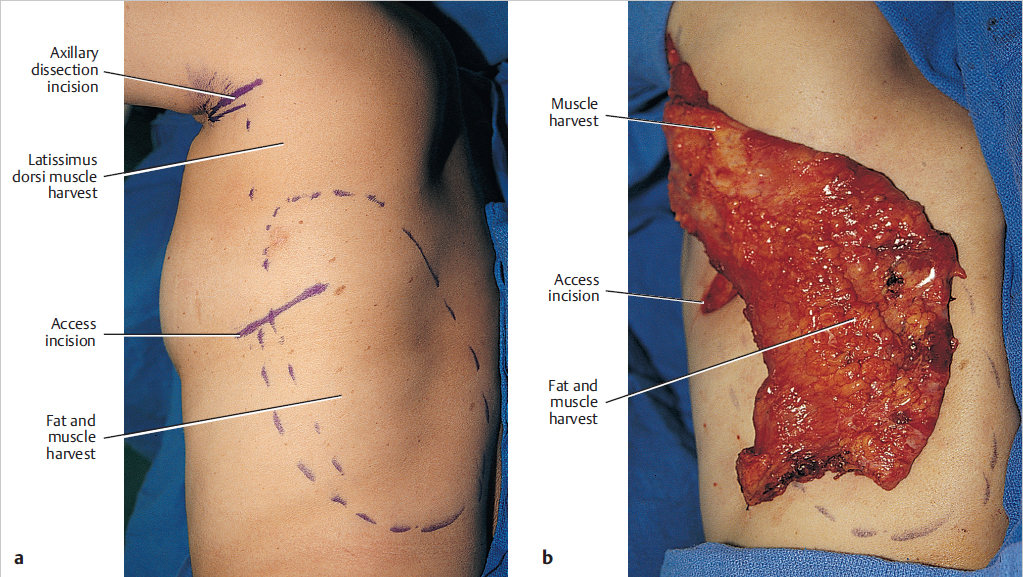
If the patient has had a nipple-sparing mastectomy and does not require additional skin, the flap may be harvested endoscopically incorporating only subcutaneous fat and muscle. In this patient, the lateral two-thirds of the LD muscle was harvested with its overlying subcutaneous tissue. The endoscope was inserted through the axillary incision as well as through the lateral incision. To control bleeding, wetting solution was infiltrated over the muscle and pretunneling was performed just below the subdermal plexus. The LD margins were identified laterally, divided inferiorly, and separated from the teres major medially. The LD was divided medially from the region of the tip of the scapula inferiorly. If the patient has sufficient subcutaneous tissue, this approach provides a substantial flap for reconstructing partial or complete mastectomy deformities.
Subcutaneous tissue is removed up to the clavicle during a mastectomy. If the reconstructive effort attempts to match an opposite breast containing a large amount of subcutaneous tissue, a single layer of latissimus muscle will not be sufficient to fill the contour deformity. In this case, subcutaneous tissue is taken from the back over the latissimus muscle to provide additional bulk or extra LD muscle is folded on itself for this purpose. I try to place as much cover over the implant as possible when autologous tissue is insufficient and a breast implant is needed.
The quantity of skin excised during mastectomy also indicates the skin requirements for breast restoration. For instance, when the skin differential between the sides of the chest is smaller than 6 cm, a skin flap is probably not needed. The remaining tissue can expand sufficiently to provide a well-contoured breast with simple implant placement or tissue expansion. A layer of LD muscle, however, may be needed to provide satisfactory cover for a breast expander or a breast implant and create a more natural implant reconstruction (▶Fig. 48.8).
48.8 Status of the Thoracodorsal Pedicle
Before the surgeon harvests the LD flap, it is essential to assess the status of the thoracodorsal pedicle. Most contemporary surgeons preserve it but its presence should always be confirmed before raising the muscle. If a patient presents for delayed reconstruction, the integrity of the pedicle can usually be presumed if the thoracodorsal nerve is still intact and functioning leading to a functional contractile muscle. If the muscle does not contract, it should lead to a high index of suspicion for vascular pedicle damage as well as nerve damage. Preoperative ultrasound evaluation and/or angiography would be prudent in such a case.
48.9 Donor Site Incision Placement
The donor site scar for the LD flap can be placed in one of the three locations:
Horizontal oblique (most favorable).
Transverse.
Vertical lateral oblique (least favorable).
The horizontal oblique variants place the incision in a location that falls within the bra strap line and is therefore more easily concealed. The vertical lateral oblique incision creates an extremely unattractive, easily visible scar that is prone to severe widening as skin tension pulls across the scar. When only the LD muscle is needed, it can be harvested through a short vertical or horizontal lateral incision. Endoscopic harvest can be accomplished through an axillary incision and one or two short incisions over the muscle.
48.9.1 Lateral and Transverse Incisions
The typical location and length of the oblique lateral donor site scar are shown, as well as its tendency to widen (▶Fig. 48.9).
48.9.2 Oblique Incision within Lange’s Lines
An incision made in the natural skin lines of the back is ideal for a patient who wants the finest posterior scarring, which can usually be concealed by a brassiere strap. The relaxed skin tension lines flow inferolaterally. The incisions and donor site defects in these lines heal favorably. Placement of the skin island in this low oblique position permits anterior transfer of a large surface area of skin and muscle (▶Fig. 48.10).

The donor site is shown for an LD musculocutaneous island flap taken from a natural crease in the direction of the natural skin lines of this patient’s back. The back scar has remained thin (▶Fig. 48.11).

A guide to skin island decision making and planning is provided in ▶Table 48.1.
48.10 Operative Technique for Immediate Breast Reconstruction
Surgical Plan
Preoperative marking.
Patient positioning on the operating table.
Skin island incisions.
Harvesting fat for extended autologous harvest.
Identification of the superior and anterior muscle borders.
Division of the inferior and medial border and reflection over the serratus fat pad.
Pedicle dissection.
Muscle insertion division.
Creation of a high subcutaneous tunnel.
Transposition of the muscle.
Inset.
48.10.1 Preoperative Marking
The patient is always marked in the erect position. The tip of the scapula is palpated and marked. The anterior border of the latissimus muscle is palpated and marked obliquely down to the waist. The upper border of the muscle overlaps the tip of the scapula and can be marked in its approximate location transversely. The paramedian origin of the muscle is drawn. The skin island is delineated by the extent of the oblique fat roll in the mid back of most women in the area of the bra strap line. The upper border should be marked so as not to extend above the superior aspect of the muscle. The width of the flap is usually determined preoperatively and can be drawn on the back and tested for ease of closure based on the skin tension using a pinch test (▶Fig. 48.10).
48.10.2 Patient Positioning
In most instances, LD harvest is performed with the patient placed on a bean bag in the lateral decubitus position, with careful padding to all pressure points, including the brachial plexus in the axilla and the peroneal nerve of the dependent leg. An axillary roll must be placed in the axilla, and the patient’s head should be placed on a thick, supportive foam pad so the nerves of the brachial plexus are not stretched as they emerge from the cervical foramina. Many surgeons place the arm on the operative side onto a stabilized arm support. However, this requires complex draping and does not allow intraoperative repositioning (▶Fig. 48.12).
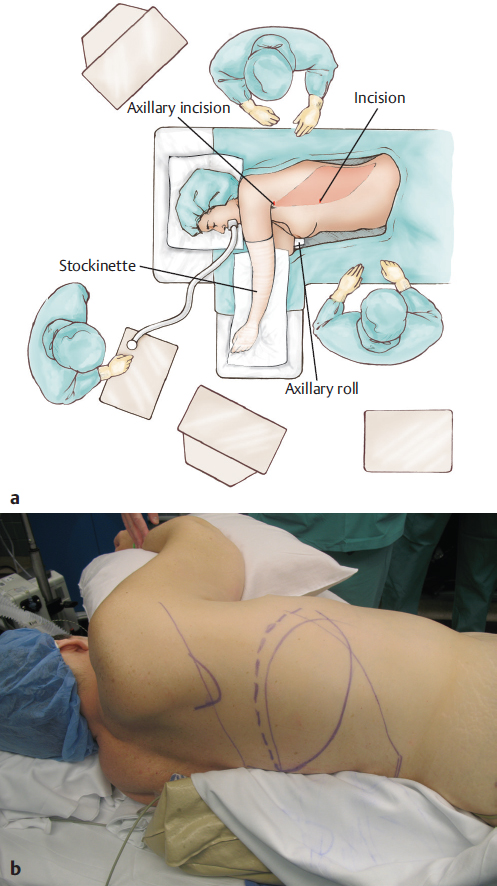
Technical Pearl
I always prep the arm into the sterile field and cover the hand and forearm with an impervious stockinette sleeve, which allows me to flex and extend the humerus at the shoulder, providing easier donor site closure and ready access to the mastectomy site for muscle transposition anteriorly.
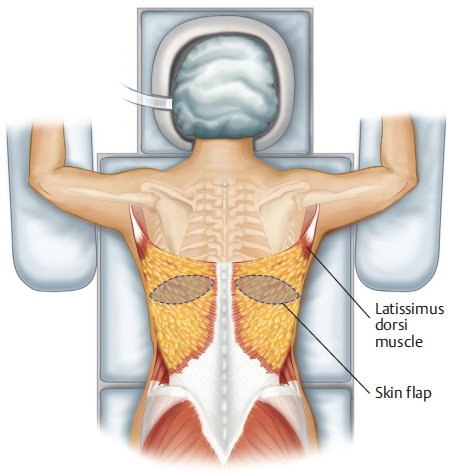
If the patient is having bilateral reconstruction, I start with her in the prone position, raise both flaps, and place them in the axillae before closing the back. The patient is then turned to the supine position, and the flaps are brought into the mastectomy sites anteriorly for positioning and insetting (▶Fig. 48.13).
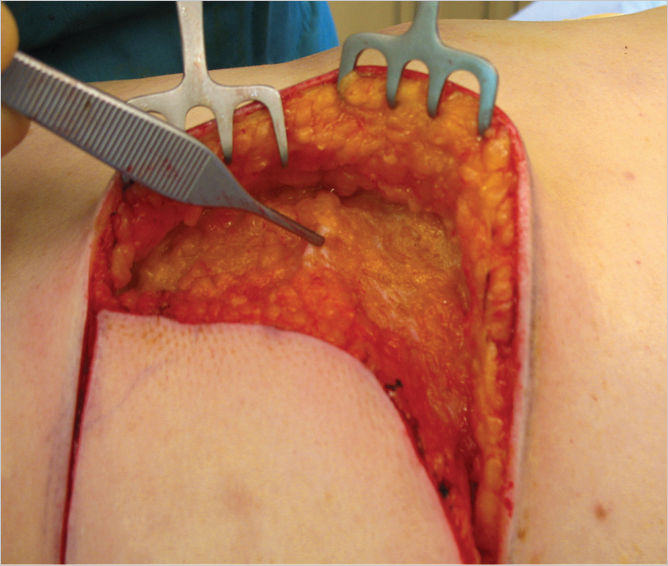
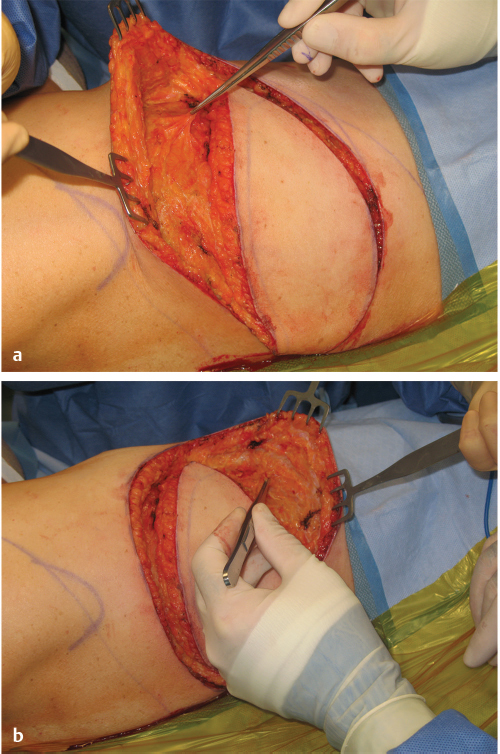
48.10.3 Skin Island Incision
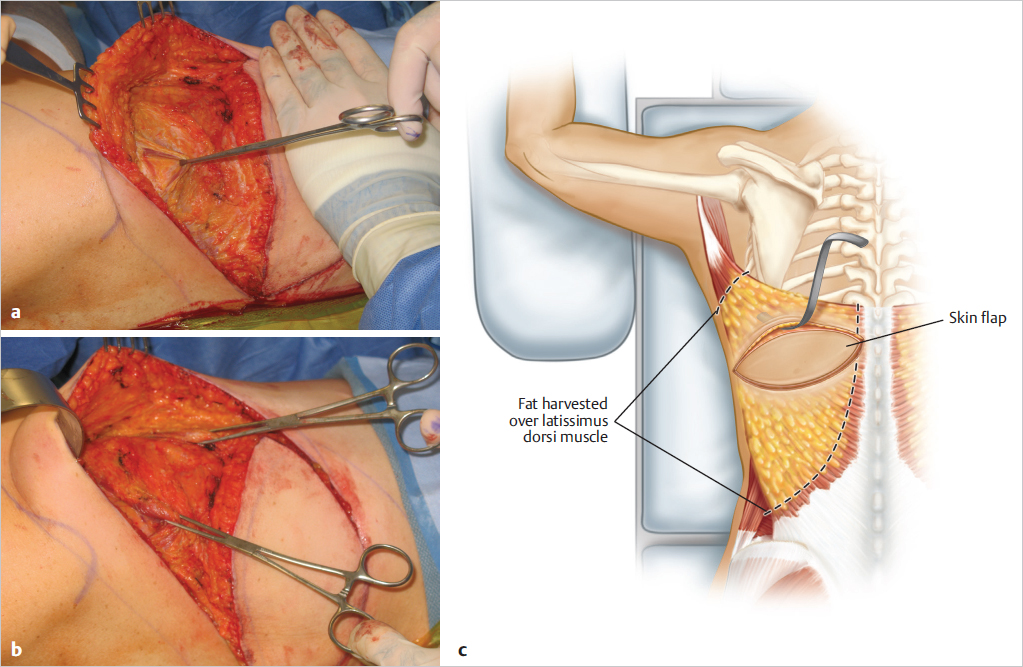
The upper border of the skin island is incised and subcutaneous dissection beveled in the cephalad direction down to Scarpa’s fascia. If dissection is taken down vertically onto the muscle, it is sometimes difficult to create a pleasing inset of the latissimus island into the breast anteriorly, because the thickness of the back skin and subcutaneous fat creates an unsightly step-off before the muscle belly is reached. This can be very visible through thin mastectomy skin flaps and can be prevented by beveling the fat harvest gently onto the underlying muscle as shown in ▶Fig. 48.14. As mentioned earlier, fat can be harvested over much of the muscle surface thereby increasing the available volume for reconstruction (▶Fig. 48.15). Once the upper border of the latissimus is reached, the fat harvest is beveled directly onto the muscle belly and no further fat harvest is carried out toward the insertion of the muscle as this provides unwanted bulk in the axillary tunnel after transposition.
48.10.4 Initial Muscle Dissection
The inferior limit of the flap is incised and a similar beveled dissection is carried inferiorly, stopping the fat harvest near the waistline. The superior, medial, lateral, and inferior borders of the muscle are identified. The medial and inferior borders are incised with electrocautery and are elevated with an Allis tissue forceps (▶Fig. 48.16).
48.10.5 Latissimus Dorsi Muscle Harvest over the Serratus Fat Pad
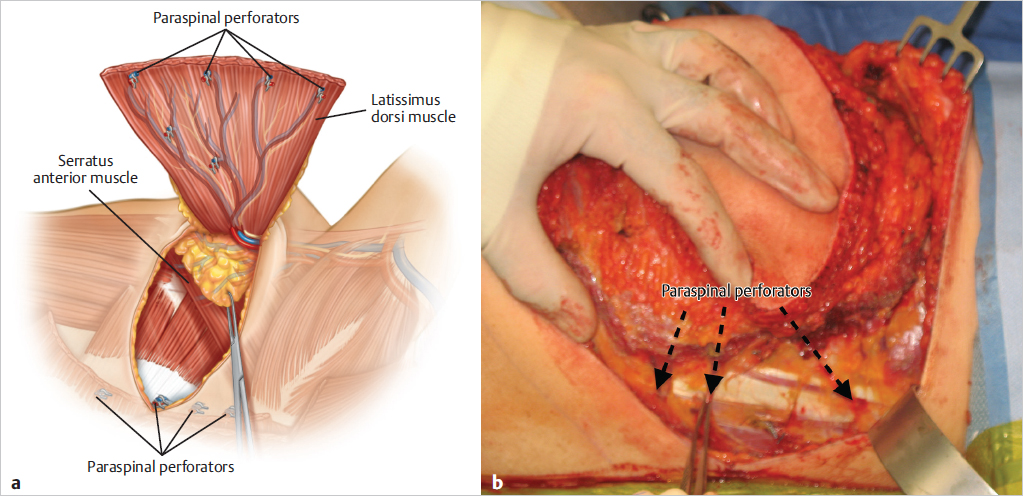
The flap is reflected from medial to lateral, dividing the paraspinal perforators with Ligaclips as they are encountered (▶Fig. 48.17). Failure to control these vessels well can result in hematoma formation as they are quite sizeable.
The latissimus muscle is reflected laterally until the fat pad between it and the serratus anterior is encountered. A tissue forceps is placed on the fat pad to provide countertraction, and the latissimus muscle is elevated superficial to the fat pad, off the surface of the serratus anterior (▶Fig. 48.18).
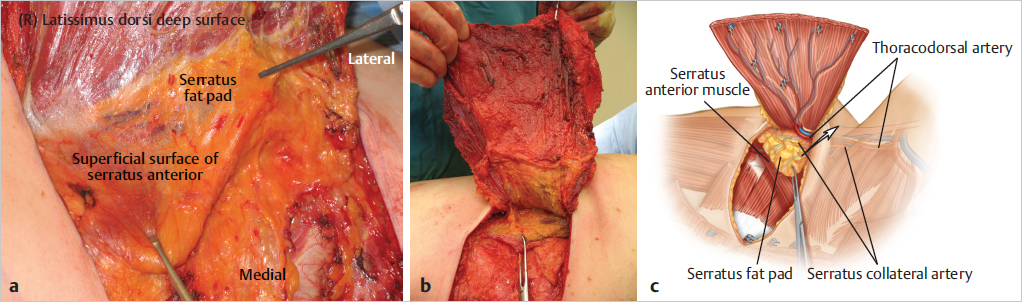
Teaching Pearl
The serratus fat pad is a key element to simplifying the posterior approach to latissimus dorsi flap dissection. Once identified, it guides the surgeon clearly over the serratus muscle, preventing accidental damage to the pedicle or elevation of serratus anterior with latissimus.
Related posts:
 49 Preventing and Managing Complications in Latissimus Dorsi Flap Reconstruction
49 Preventing and Managing Complications in Latissimus Dorsi Flap Reconstruction
 45 Preventing and Managing Complications of Expander–Implant Reconstruction
45 Preventing and Managing Complications of Expander–Implant Reconstruction
 47 Latissimus Dorsi Flap Anatomy
47 Latissimus Dorsi Flap Anatomy
 42 Prepectoral Direct-to-Implant Breast Reconstruction
42 Prepectoral Direct-to-Implant Breast Reconstruction
 39 Prepectoral Breast Reconstruction: Direct-to-Implant versus Two-Stage
39 Prepectoral Breast Reconstruction: Direct-to-Implant versus Two-Stage
 51 Transverse Rectus Abdominis Musculocutaneous Flaps
51 Transverse Rectus Abdominis Musculocutaneous Flaps
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


