49 Preventing and Managing Complications in Latissimus Dorsi Flap Reconstruction
Summary
This chapter summarizes the key complications in latissimus dorsi flap reconstruction. Each complication, its cause, and prevention is outlined.
Key Teaching Points
Pedicle torsion or traction injury should be prevented at all costs.
Pedicle compression in the axilla causes venous congestion.
Failure to secure the flap to the chest wall causes implant malposition.
Seroma is the commonest problem in latissimus dorsi flap reconstruction.
Long-term drainage reduces seroma.
Animation deformity is prevented by thoracodorsal nerve division.
Complications in Latissimus Dorsi Flap Reconstruction
Pedicle twisting causing ischemia.
Poor flap design causing ischemia.
Pedicle compression in the axilla.
Implant dislocation into the donor site.
Seroma formation.
Poor donor site scarring.
Lateral chest wall bulging.
Flap animation deformity.
Step-off deformity of the skin island.
49.1 Pedicle Twisting Causing Ischemia
The latissimus flap has a remarkably dependable and consistent vascular pedicle. Problems can occur when transposing the flap to the anterior chest, which requires rotation of almost 180 degrees from posterior to anterior. In addition, the flap itself may be rotated on itself to sit comfortably on the anterior recipient site. All of these maneuvers take place when passing the flap through a subcutaneous tunnel high in the axilla. If care is not taken during this transposition, the pedicle can inadvertently be twisted along its vertical axis or kinked if the edges of the subcutaneous tunnel are not generous enough. Failure to release the superior aspect of the tunnel can create a situation in which the pedicle is bent in an L shape as it passes into the mastectomy site causing a kink in the pedicle restricting blood flow.
Technical Pearls
Prevention of Twisting
Create a generous tunnel for transposition.
Ensure a gentle curve is created at the superior edge of the tunnel to prevent kinking on the fascial attachments at the entrance to the tunnel.
Mark the pedicle with a longitudinal ink mark, which can be observed to ensure that the orientation remains linear throughout the tunnel track.
Prevent excessive tension on the pedicle during inset.
49.2 Poor Flap Design
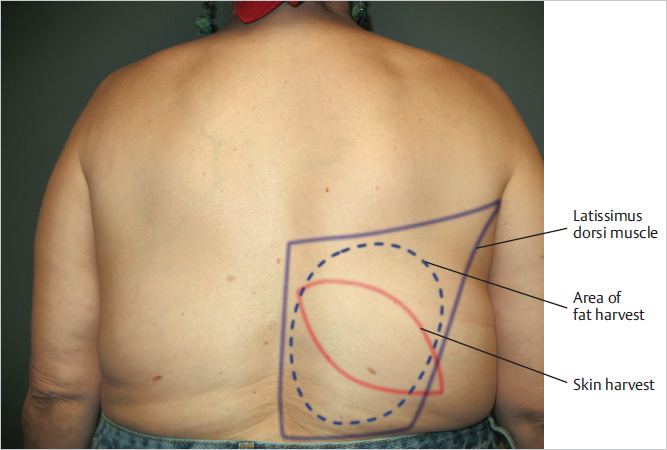
Perforators supplying the latissimus muscle are derived from the thoracodorsal axis laterally and the paraspinal perforators medially. Thoracodorsal supply will maintain vascular supply to the entire muscle, although its reach can become more limited at the extreme inferior and medial edges of the flap. Most skin islands placed on the upper half of the muscle for breast reconstruction have an incredibly robust circulation despite interruption of the paraspinal perforators. As the skin island is moved inferiorly and medially, it may become more reliant upon the medial paraspinal circulation.
Technical Pearl
Any skin island designed over the inferior and lateral border of the muscle, particularly if it overhangs the lateral border, is likely to encounter ischemic complications resulting in loss of the skin despite proximal muscle survival (▶Fig. 49.1).
49.3 Pedicle Compression in the Axilla
The contents of the subcutaneous tunnel created to allow passage of the latissimus dorsi (LD) flap onto the anterior chest from the posterior donor site include the following:
The vascular pedicle.
The distal insertion of the muscle (now detached from the humerus).
Potentially variable amounts of fat harvested with the flap.
The fat of the axillary skin.
Technical Pearl
When harvesting the flap, the point was made in Chapter 48, that no fat should be harvested over the distal muscle from a point level with the tip of the scapula to the humeral insertion.
Related posts:
 40 Two-Stage Subpectoral Tissue Expander–Implant Reconstruction
40 Two-Stage Subpectoral Tissue Expander–Implant Reconstruction
 47 Latissimus Dorsi Flap Anatomy
47 Latissimus Dorsi Flap Anatomy
 44 Two-Stage Prepectoral Prosthetic Breast Reconstruction
44 Two-Stage Prepectoral Prosthetic Breast Reconstruction
 42 Prepectoral Direct-to-Implant Breast Reconstruction
42 Prepectoral Direct-to-Implant Breast Reconstruction
 39 Prepectoral Breast Reconstruction: Direct-to-Implant versus Two-Stage
39 Prepectoral Breast Reconstruction: Direct-to-Implant versus Two-Stage
 51 Transverse Rectus Abdominis Musculocutaneous Flaps
51 Transverse Rectus Abdominis Musculocutaneous Flaps
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


