Abstract
Preservation rhinoplasty (PR) is a new chapter in rhinoplasty history. The term was first coined by Daniel in 2018, and represents a fundamental change in philosophy. Just as the open approach transformed rhinoplasty surgery, so has PR as surgeons rethink traditional dogma. In certain cases, the standard teaching of reduce and rebuild can be replaced with preserve and reshape. Structural rhinoplasty evolved as surgeons realized that when nasal anatomy is taken apart and/or made smaller, structures must be rebuilt and strengthened to resist the forces of scar contracture. However, if anatomy is preserved less structural rebuilding is necessary. This chapter details the PR, which includes preservation of the soft tissue envelope, alar cartilages, and osseocartilaginous dorsum.
21 The Preservation Rhinoplasty
Key Points
Preservation rhinoplasty involves preservation of the soft tissue envelope, ligaments, alar cartilages, and dorsum.
Preservation rhinoplasty is a change in rhinoplasty philosophy where resection is replaced with reshaping.
Preserve as much of the native structures of the nose as possible and the surgeon will have less to rebuild and less chance for scar contracture, warping, and distortion in the future.
21.1 Preoperative Steps
The patient is evaluated during consultation by asking what three things the patient wants to change about his or her nose.
Physical examination is done sequentially with a focus on the ability to preserve all aspects of the nose including the soft tissue envelope, the nasal ligaments, the alar cartilages, and the dorsum.
The author begins with an evaluation of the thickness and quality of the soft tissue envelope to assess the surgical plane of dissection for both the tip and the dorsum—subSMAS, subperichondrial, or subdermal.
Evaluation of the alar cartilages is then performed with a focus on the volume and the strength of the lower lateral cartilages. The anterior strength and projection of the alar cartilages against the soft tissue envelope of the nose will determine the crispness of the nasal polygons.
Finally, the dorsum is evaluated first on anterior view, and then on profile view, for suitability of dorsal preservation—a two-step procedure where a septal strip is removed followed by osteotomies to lower the dorsal profile and to maintain the patient’s natural dorsal aesthetic lines without opening the cartilaginous vault.
21.2 Operative Steps
See Video 21.1.
21.2.1 Soft Tissue Envelope Preservation
Preservation of the soft tissue envelope can be done in the open or closed approach. Described below will be the open approach for the purposes of this text.
A unilateral hemitransfixion incision is made and the anterior septal angle is exposed. Using sharp scissors, the subperichondrial plane is found and dissected laterally to the intersection of the vertical and longitudinal scroll ligaments bilaterally. This subperichondrial dissection is continued up to the caudal portion of the nasal bones where a subperiosteal plane is entered up to the nasal radix and down to the cheeks in preparation for piezoelectric surgery. This is the extended open approach of the nasal dorsum.
Bilateral infracartilaginous incisions are made and at the turning point of the lateral crura, the backside of a #15 blade is used to scrape the perichondrium. Once a subperichondrial plane is developed, it is dissected to the midline and over the domes.
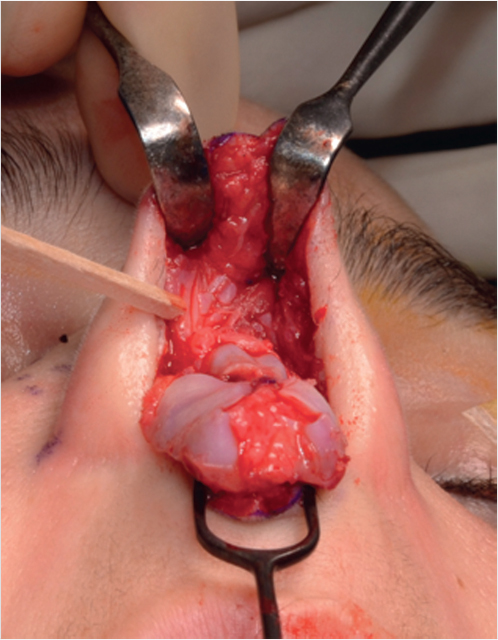
A transcolumellar incision is made, dividing the superficial Pitanguy’s ligament. The deep Pitanguy’s ligament is encountered in the midline along with its lateral vertical scroll attachments. The deep Pitanguy’s ligament is marked with a pen or two sutures and divided. The vertical scroll attachments are carefully divided, connecting the subperiochondrial dissection of the tip and dorsum. If done correctly, the scroll sesamoid cartilages should move up on the skin flap (Fig. 21.1).
In this way, a full subperichondrial-subperiosteal dissection of the nose is done and the ligaments are preserved for reattachment at the end of the rhinoplasty surgery.
21.2.2 Dorsal Preservation (High Septal Strip)
For the purpose of this text, I will be describing the high, subdorsal strip pushdown procedure as popularized by Saban.
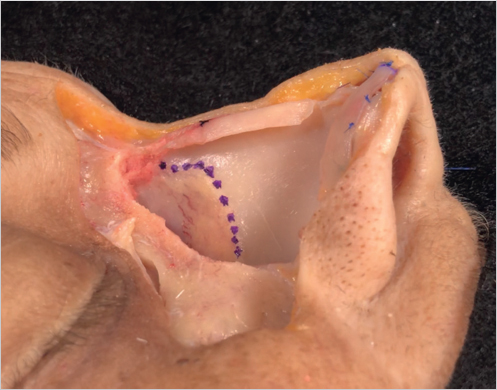
At the point where the caudal upper lateral cartilages attach to the dorsal septum (the W-point, which is often 1 cm cephalic to the anterior septal angle), a subdorsal cut is made directly under the dorsum up to the perpendicular plate of ethmoid (PPE). A second cut is made 2 mm below and a cartilaginous strip is removed. At times, a small amount of PPE is removed with a rongeur directly under the dorsum to allow space for downward impaction of the dorsum. At this point, the osseocartilaginous vault is released from the septum (Fig. 21.2).
Using straight and curved piezoelectric saws, bilateral low-to-low osteotomies are connected to bilateral transverse osteotomies and a radix osteotomy. At this point, the osseocartilaginous pyramid has been released not only from the septum, but also from face. A side-to-side movement confirms mobility of the nasal pyramid. Once this is confirmed, the dorsum is squeezed and “pushed down” into the pyriform aperture.
Incremental strips of cartilage can be removed for further lowering and flexion of the osseocartilaginous joint.
If the surgeon is having trouble with descent of the dorsum, several blocking points are checked including all osteotomy lines, the separation of the dorsum from the septum, and that space has been created laterally for descent into the pyriform aperture.
Once the dorsum has been lowered and the surgeon is satisfied, at least one suture is used to reattach the dorsum to the septum at the W-point. More sutures can be added to the keystone area between the dorsum and subdorsal septum as needed, but is not mandatory. Finally, the W-ASA segment (the area between the W-point and anterior septal angle) can be modified to adjust the height at the supratip.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


