Abstract
The approach to the nasal tip requires a combination of techniques that will improve tip shape and establish proper support. Here, we provide a focused review of nasal tip analysis and surgical technique, with particular emphasis on tip sutures and cartilage grafts.
17 Graduated Approach to Tip Projection
Key Points
Understanding the underlying anatomic components that provide nasal tip support, and their effect on tip projection and shape is a prerequisite for successful tip shaping.
A comprehensive and systematic nasofacial analysis is the most important initial step in establishing goals and formulating a precise surgical plan for nasal tip projection and shape.
17.1 Factors that Determine Tip Projection
Length, width, and strength of the lower lateral cartilages.
Length and stability of the medial crura.
Suspensory ligament that spans the crura over the anterior septal angle.
Fibrous connections between the upper and lower lateral cartilages.
Abutment with the pyriform aperture.
Anterior septal angle.
Skin and soft tissue thickness.
17.2 Preoperative Planning
17.2.1 Nasofacial Proportions and Systematic Nasal Analysis: “10–7-5” Nasal Analysis
On the front view, evaluation should include 10 key areas: Facial proportions, skin type/skin thickness, symmetry/nasal deviation, bony vault width, midvault asymmetry, dorsal aesthetic lines, tip shape/tip-defining points, alar rims/base, infratip lobular projection, and periapical hypoplasia/upper lip length.
The profile view includes 7 areas: Radix height and position, dorsal convexity, nasal length, tip projection, tip rotation, alar–columellar relationship, and chin projection.
The base view aids in the assessment of 5 areas: Nasal projection, nostril shape/symmetry, columella symmetry/width, alar base width, and alar rim flaring.
17.2.2 Nasal Tip Assessment
Thick and sebaceous skin may camouflage the results of tip modification.
Domal asymmetry, tip dysmorphology (boxy or bulbous tip), degree of nostril show, columellar excess, caudal septal deviation, and a plunging or hyperdynamic tip should be noted.
Animated views should be obtained to diagnose depressor septi nasi hyperactivity resulting in hyperdynamic tip ptosis.
On the lateral view, 50 to 60% of the tip should lie anterior to a vertical line drawn adjacent to the most projecting part of the upper lip and can also be measured as 0.67 times the ideal nasal length (Fig. 17.1a, b).
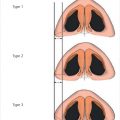
On the basal view, the ideal nostril–tip relationship should be approximately 2:1 (Fig. 17.2).
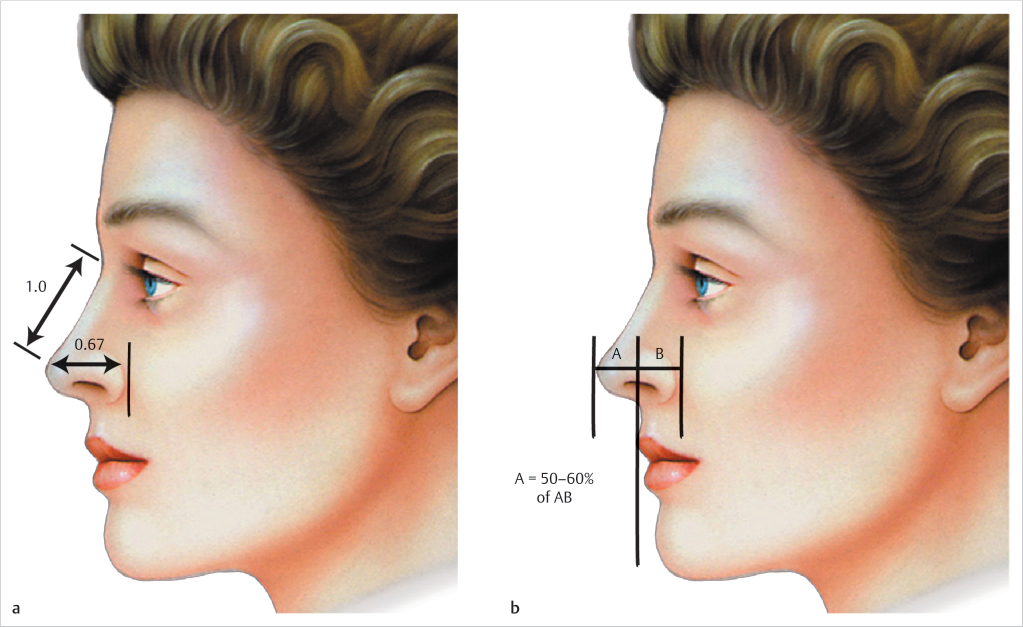
Fig. 17.1 (a, b) Ideal nasal projection on the lateral view. About 50 to 60% of the tip should lie anterior to a vertical line drawn adjacent to the most projecting part of the upper lip and can also be measured as 0.67 times the ideal nasal length. (Reproduced with permission from Rohrich R, Adams W, Ahmad J, eds. Dallas Rhinoplasty: Nasal Surgery by the Masters. 1st ed. Thieme; 2014.) 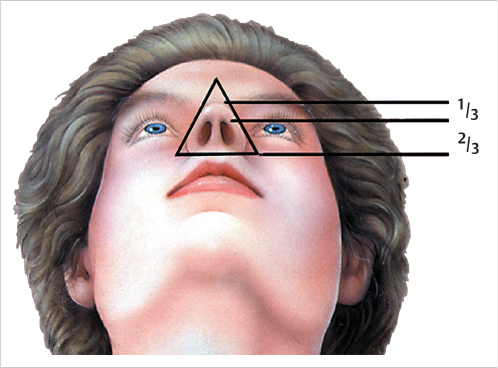
Fig. 17.2 Ideal nostril–tip relationship should be approximately 2:1 on the basal view. (Reproduced with permission from Rohrich R, Adams W, Ahmad J, eds. Dallas Rhinoplasty: Nasal Surgery by the Masters. 1st ed. Thieme; 2014.)
17.3 Intraoperative Assessment
The lateral crura are assessed for their degree of convexity/concavity, length/width dimensions, position, and symmetry.
Analysis of the length and strength of the medial crura are critical for tip projection and definition:
Medial crura that are long and stable are less likely to contribute to loss of tip projection postoperatively.
Short and/or weak medial crura can lead to a loss of supratip definition as the differential between dorsal height and domal peak is diminished.
The domes are characterized in terms of the domal arch width, angle of divergence, and degree of symmetry.
Analyzing the relationship between the lateral crura, domes, and medial crura is important as modifications to one will often have an effect on the others.
17.4 Operative Technique
Cephalic trim: It is performed in cases of bulbous or boxy domes by separating the lower lateral cartilages from the upper lateral cartilages at the scroll area and trimming them, leaving at least a 6-mm-wide rim strip. This reduces the length of the cartilaginous framework and facilitates passive cephalic rotation of the lower lateral cartilage (Fig. 17.3).
Septal extension graft: A versatile graft that effectively controls tip projection, shape, and rotation whereas a columellar strut graft is only effective for unifying the nasal tip and maintaining projection while lacking control over nasal tip rotation. The septal extension graft is keel-shaped to mimic the inferior margin of the middle crura. It is placed onto the anterior septal angle as a “fixed-floating” graft with extension beyond the anterior septal angle into the interdomal space with the most caudal and inferior portion of the graft placed on the cephalic border of the medial crus at the columellar-lobular angle.
A four-step suture technique is performed (Fig. 17.4):
Body fixation horizontal mattress suture.
Superior stabilization suture.
Inferior stabilization suture.
Body stabilization horizontal mattress suture.
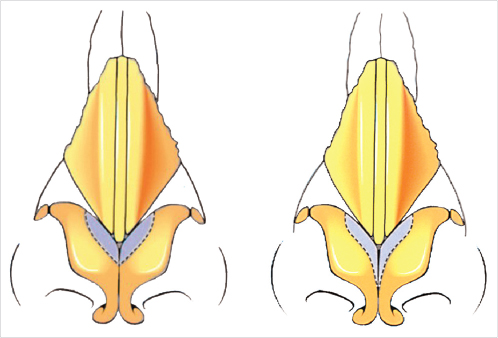
Fig. 17.3 Cephalic trim of the lateral crus of the lower lateral cartilages. (Reproduced with permission from Rohrich R, Ahmad J, eds. The Dallas Rhinoplasty and Dallas Cosmetic Surgery Dissection Guide. 1st ed. Thieme; 2018.) 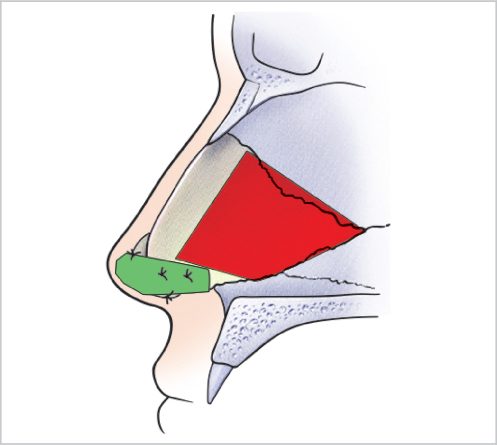
Fig. 17.4 Septal extension graft. Four-step suture technique.
17.4.1 Reshaping of the Nasal Tip Proceeds Using a Bottom-up Approach
Medial crural footplate approximation corrects footplate deformities and asymmetries (Fig. 17.5).
“Low” medial crural approximation stabilizes the graft, corrects asymmetries, controls columellar width, and strengthens the medial crura (Fig. 17.6).
“High” medial crural approximation further stabilizes the medial crura to the graft and aids in establishing columellar width and proper symmetry (Fig. 17.6).
Transdomal suturing increases tip projection, corrects lateral crural convexities, and narrows and defines the tip (Fig. 17.7).
Interdomal approximation decreases the angle of divergence, narrows the tip-defining points, and corrects vertical asymmetries (Fig. 17.8).
Tip grafts are used to camouflage prominent and sharp angles of the underlying framework. Cap grafts, infratip lobular grafts, and morselized cartilage are examples of commonly used grafts (Fig. 17.9).
See Video 17.1.
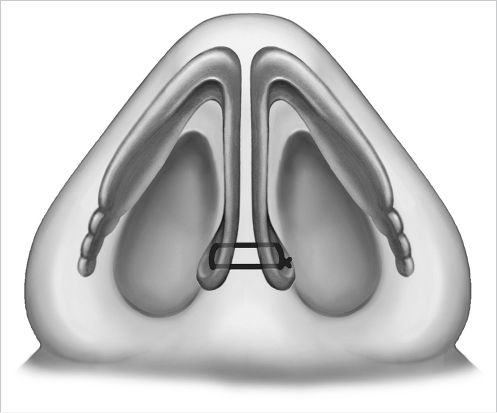
Fig. 17.5 Medial crural footplate suture. (Reproduced with permission from Janis J, ed. Essentials of Aesthetic Surgery. 1st ed. Thieme; 2018.) 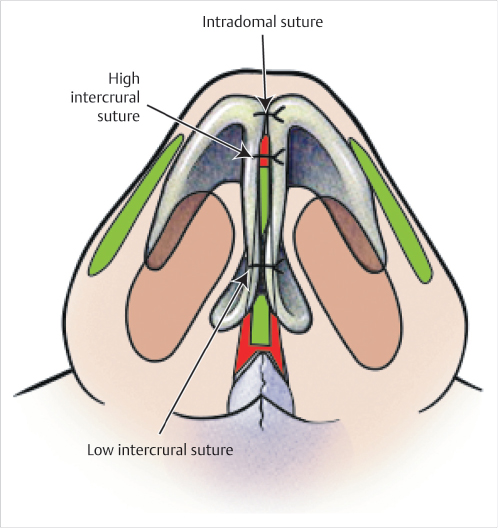
Fig. 17.6 Low and high intercrural sutures. (Reproduced with permission from Rohrich R, Ahmad J, eds. The Dallas Rhinoplasty and Dallas Cosmetic Surgery Dissection Guide. 1st ed. Thieme; 2018.) 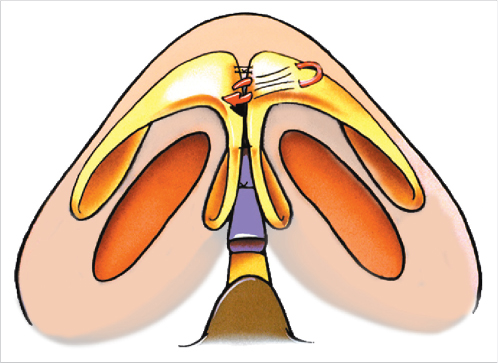
Fig. 17.7 Transdomal suture. (Reproduced with permission from Rohrich R, Ahmad J, eds. The Dallas Rhinoplasty and Dallas Cosmetic Surgery Dissection Guide. 1st ed. Thieme; 2018.) 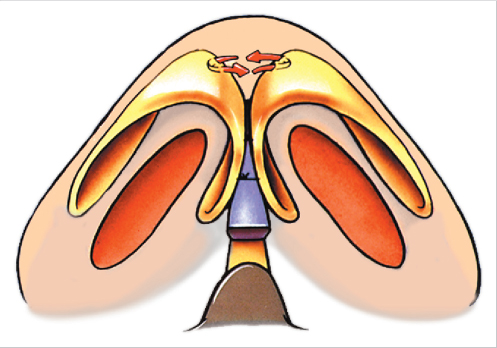
Fig. 17.8 Interdomal suture. (Reproduced with permission from Rohrich R, Ahmad J, eds. The Dallas Rhinoplasty and Dallas Cosmetic Surgery Dissection Guide. 1st ed. Thieme; 2018.) 
Fig. 17.9 Butterfly graft. (Reproduced with permission from Rohrich R, Ahmad J, eds. The Dallas Rhinoplasty and Dallas Cosmetic Surgery Dissection Guide. 1st ed. Thieme; 2018.)
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


