Abstract
Success in ethnic rhinoplasty can be achieved through accurate preoperative analysis, recognition of the common and variable features within each ethnic group, and precise technical maneuvers. The open approach allows for precise intraoperative anatomic diagnosis and the construction of an ethnically congruent nose. Familiarity with a range of cartilage grafting techniques is critical to the surgeon’s repertoire. A combination of tip suturing techniques is needed in ethnic rhinoplasty; however, overly exaggerated modification is to be avoided. Skin redraping is done throughout the process of dorsal modification and tip shaping to assess the influence of each maneuver on the external surface. The cartilaginous frame should be fashioned by maneuvers that increase tip support and add refinement. Selective debulking of the nasal skin/soft tissue envelope improves its contractile response to the underlying architecture. Ethnic patients, in particular, are counseled on the prolonged postoperative healing and instructed on self-taping to help with edema.
Although ethnic rhinoplasty is far more complicated than in Caucasian patients, excellent outcomes can be obtained by experienced surgeons who recognize that the ultimate goal is nasofacial harmony.
20 The Ethnic Nose
Key Points
Patient selection and management of expectations are prerequisites to achieving good outcomes and patient satisfaction in ethnic rhinoplasty.
Although a variable spectrum of nasal morphology exists within each ethnic group, certain characteristics are generally present and can overlap with other ethnicities (Table 20.1).
Patients generally fall into two categories: those whose desire a nose aligned with Caucasian ideals, and those who want to preserve their ancestral traits.
The surgeon must recognize which presenting traits require which treatments and what combination of techniques will ultimately produce a racially congruent aesthetic result.
Familiarity with a range of cartilage grafting techniques is critical to the surgeon’s repertoire.
A combination of tip suturing techniques is needed in ethnic rhinoplasty; however, overly exaggerated modification is to be avoided.
Regardless of ethnic origin, the ultimate goal is to create nasofacial harmony.
20.1 Preoperative Steps
A thorough approach to nasofacial analysis is critical to achieving harmony and balance in ethnic rhinoplasty.
Appreciate the most common goals in rhinoplasty among different ethnic groups (Table 20.2).
Evaluate each nose individually, define problematic areas across nasofacial morphologies, and recognize anatomical features that allow for ethnic congruity (Fig. 20.1a–c).
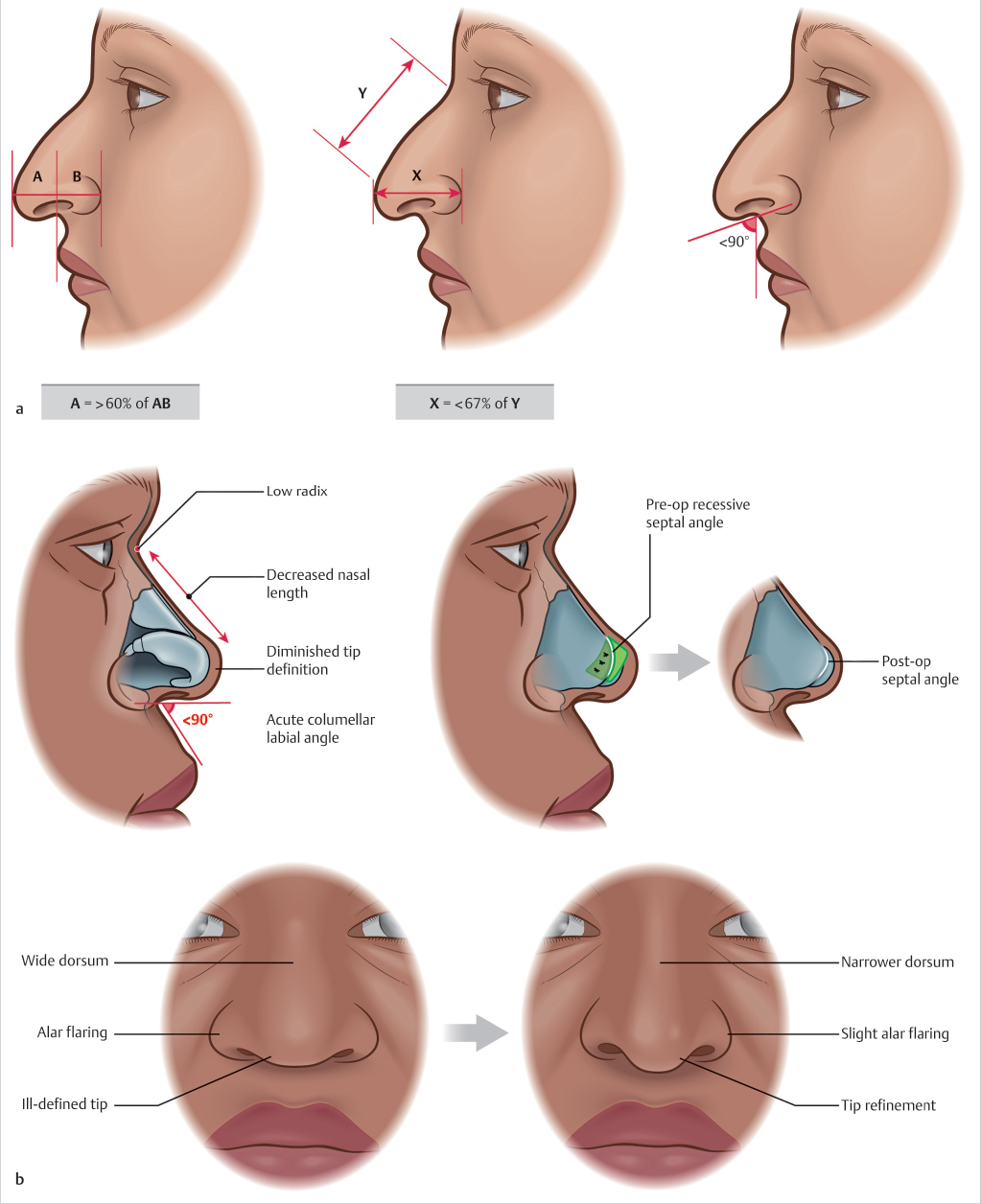
Fig. 20.1 (a) Middle Eastern nasofacial morphology. (b) African American nasofacial morphology. 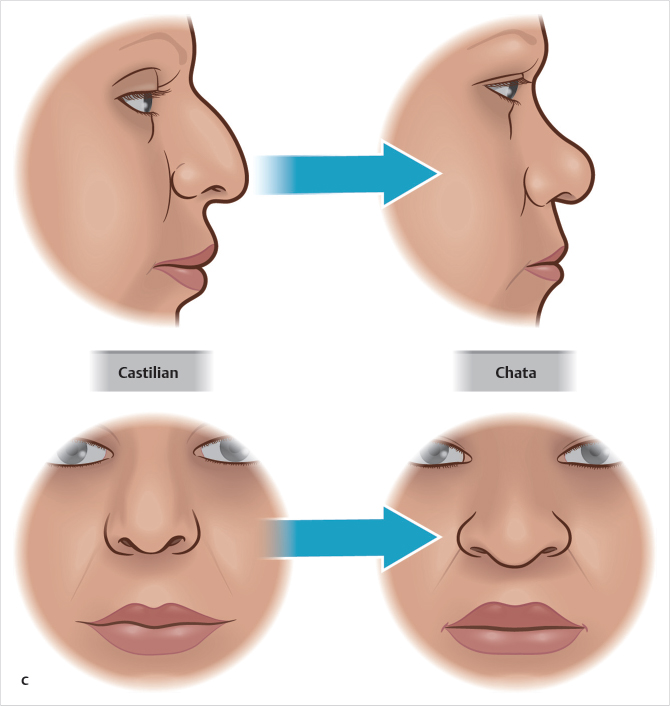
Fig. 20.1 (Continued). (c) Hispanic nasofacial morphology.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


