Abstract
Caudal septal extension grafts stabilize the nasal base and set nasal tip position. The airway should be carefully evaluated for signs of severe septal deviation, perforation, nasal valve obstruction, or turbinate hypertrophy. There are seven subtypes of grafts available depending on the patient’s nasal deformity. The most commonly used grafts are the superiorly based end-to-end and rectangular-shaped. It is imperative that the surgeon counsel the patient regarding possible outcomes, which include a horizontal, upper lip crease with smiling and stiffness of the nasal tip. Proper, aesthetic nasal proportions and patient’s desires should always be kept in mind when using these techniques.
26 Ancillary Maneuvers in Rhinoplasty: Septal Extension Grafts
Key Points
Caudal septal extension grafts stabilize the nasal base and set nasal tip position.
There are seven subtypes of grafts available depending on the patient’s existing nasal deformity.
Regardless of the chosen technique, care should be taken to avoid obstructing the nasal airway.
26.1 Preoperative Steps
On profile view, the tip projection and rotation, alar–columellar relationship, and premaxilla must be carefully evaluated.
Whether via anterior rhinoscopy and/or rigid endoscope, the septum should be visualized and examined for severe deviation, septal perforation, nasal valve blockage, or turbinate hypertrophy.
The caudal septum should be straight and in a midline position; caudal septal deviations must be corrected prior to placing a caudal septal extension graft.
There must be sufficient vestibular skin available to position the caudal septal extension graft.
The patient should be advised that graft placement will make the tip stiff and have less recoil; additionally, the upper lip may become rigid or develop a horizontal crease.
26.2 Operative Steps
See Video 26.1.
26.2.1 Incisions and Dissection
After sterile preparation and positioning, the nose is infiltrated with 1% lidocaine with 1:100,000 epinephrine.
Attention is directed to the posteroinferior septum whereupon a segment of cartilage is removed while preserving at least a 1.5 cm L-strut of native septum; if the caudal septum is deviated, bilateral splinting spreader grafts can be used to straighten the caudal septum.
An external rhinoplasty approach is then initiated carefully exposing the lower lateral cartilages, caudal septum, and middle vault.
26.2.2 Graft Selection and Placement
Most grafts are designed as a right-angle triangle with the longer margin oriented superiorly to control tip position and prevent over-rotation of the tip.
There are seven subtypes of grafts if the standard, right-angle triangle is not suitable for the patient.
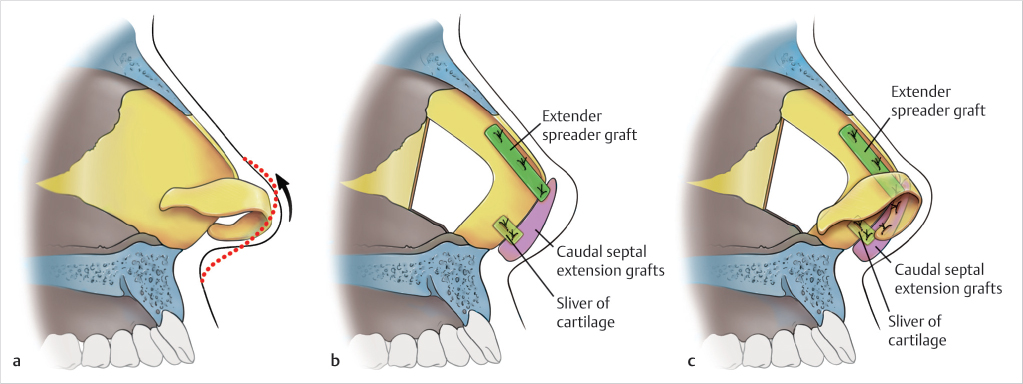
Superiorly Based End-to-End Caudal Septal Extension Graft (Fig. 26.1)
It is the most commonly used type of extension graft.
This graft will support the nasal base with minimal effect on the upper lip.
It is less likely to create stiffness in the upper lip.
This graft does not extend to the nasal spine and should be used in conjunction with a medial crural footplate suture and a nasolabial angle plumping graft.
Softer cartilage with attached soft tissue should be used for the plumping graft and can be secured transcutaneously if needed.
(Reproduced with permission from Rohrich R, Adams W, Ahmad J, et al, eds. Dallas Rhinoplasty. 3rd ed. Thieme; 2014.)
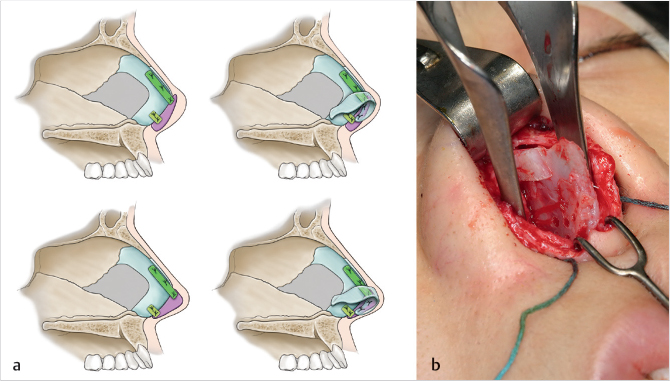
Rectangular-Shaped Caudal Septal Extension Graft (Fig. 26.2a, b)
Used for significant increases in tip projection as the graft should extend beyond the anterior septal angle.
Helps support a weak base.
Ethnic populations (i.e., Asians), congenital defects, and secondary rhinoplasty patients are ideal candidates.
Avoid tacking to nasal spine to minimize effect on upper lip.
Can be used to open the nasolabial angle.
May create stiffness in the upper lip.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


