Abstract
The initial consultation is an integral component when deciding if a patient is suitable for surgery. The patient should identify their top three nasal aesthetic and/or functional concerns and record them precisely. The surgeon’s goals and patient’s expectations must be aligned. Caution should be taken in any patients that exhibit unrealistic expectations or signs of underlying psychosocial issues.
14 The Rhinoplasty Consult
Key Points
A comprehensive and systematic nasofacial analysis is the most critical initial step in establishing goals and formulating a precise surgical plan for aesthetic nasal surgery.
Setting realistic expectations with the patient is critical in achieving high postoperative patient satisfaction.
14.1 Preoperative Planning
14.1.1 Defining Rhinoplasty Goals
Have the patient list their top three nasal aesthetic and/or functional concerns and record them precisely.
14.1.2 Focused Nasal History
The patient should be asked about a history of allergic or inflammatory disorders such as hay fever, asthma, rhinitis, and sinusitis.
Patients with long-standing allergic rhinitis typically have nasal obstruction due to inferior turbinate hypertrophy.
Prior nasal trauma and operations including rhinoplasty, septal reconstruction/septoplasty, and sinus surgery should be noted and, when possible, prior operative reports should be reviewed.
A review of smoking status, alcohol consumption, and use of illicit drugs, particularly cocaine, is essential as these behaviors can affect outcomes.
Medications and dietary supplements such as acetylsalicylic acid, nonsteroidal anti-inflammatory drugs, and fish oil should be reviewed as they can increase bleeding and ecchymosis.
14.1.3 Nasofacial Proportions and Systematic Nasal Analysis
See Table 14.1.
“10–7–5” Nasal Analysis
On the front view, evaluation should include 10 key areas: Facial proportions, skin type/quality, symmetry/nasal deviation, dorsal aesthetic lines, bony vault, midvault, nasal tip, alar rims, alar base, and upper lip.
Facial proportions: Evaluation of the patient should include static and dynamic views to identify possible dynamic changes of the nose and upper lip while smiling. Examples of application of nasofacial analysis are the facial golden proportions (three similar distances: trichion-to-eye, nose-to-chin, and eye-to-mouth) and ratios (equivalent horizontal thirds: hairline-to-brows, brows-to-nasal base, and nasal base-to-menton; vertical fifths: limits adjacent to the most lateral projection of the head, the lateral canthi, and the medial canthi).
Skin type/quality: Skin thickness can be a major factor affecting rhinoplasty outcomes. Thin skin may show reconstructed nasal frame imperfections; however, nasal shape definition is more easily achieved. A thicker skin can camouflage minor imperfections, but reduces the surface contour definition due to prolonged edema and inflammation that can lead to scaring and unfavorable aesthetics. Nasal skin is thickest at the radix and nasal tip and thinner at the rhinion and columella.
Symmetry/nasal deviation—three basic types: Caudal septal deviations (septal tilt, C-shaped and S-shaped), concave dorsal deformities (C-shaped, reverse C-shaped), and concave/convex dorsal deformities (S-shaped with bony pyramid deviation).
Dorsal aesthetic lines: Dorsal aesthetic lines were defined as originating on the supraorbital ridges, traversing medially along the glabellar area, converging at the medial canthal ligaments, diverging at the keystone area, and ending at the nasal tip. Dorsal aesthetic lines width should match either the interphiltral distance or the tip-defining points width. Male dorsum is wider and straighter, with less concavity at the superciliary ridges compared with women.
Bony vault: The bony vault is composed of three distinct structures, the paired nasal bones and the perpendicular plate of the ethmoid. Bony vault width, symmetry, and length of nasal bones are analyzed in frontal view. Bony base width should be 70 to 80% of the alar base, typically equal to the intercanthal distance.
Midvault: The cartilaginous midvault includes the paired upper lateral cartilages and the cartilaginous septum. The keystone area represents a triangular region, union of the six distinct anatomical structures between the bony vault and the cartilaginous midvault. Midvault width and deformities like the inverted-V or saddle-nose are identified.
Nasal tip: The normal tip configuration (triangular and well-defined) should be distinguished from the bulbous tip (rounded and ill-defined) and the boxy tip (square and wide). Anatomically, the nasal tip has an angle of divergence of 30 degrees, the domal arc a width of 4 mm or less, and a distance between the tip-defining points of 5 to 6 mm. It can be broad and less defined in men. The boxy tip may result of an increased angle of divergence (>30 degrees), a widened domal arc (>4 mm), or a combination of the two.
Alar rims: The alar rim’s ideal shape resembles a gull in flight. Alar rim deformities, such as retraction, notching, collapse, and asymmetry, are common problems in rhinoplasty patients.
Alar base: Alar base width ideally approximates the intercanthal distance, one-fifth of the face width, or 70% of nasal height. Alar base surgery is performed to address excessive width of the nasal base, alar flaring, large nostril size, and alar base or nostril asymmetries.
Upper lip: Ideal upper lip position is considered 1 to 2 mm of gingival show on maximum smile (slightly less in males). A hyperactive depressor septi muscle is associated with a deformity during animation (particularly with smiling) characterized by a drooping nasal tip, shortened upper lip, and a transverse crease in the midphiltral area. Resection and release/transposition techniques were proposed to correct this deformity and enhance the tip–lip relationship.
The profile view includes 7 areas: Nasofrontal angle and radix, nasal length, dorsum and supratip, tip projection (Fig. 14.1), tip rotation, alar–columellar relationship, periapical hypoplasia, and lip–chin relationship.
Nasofrontal angle and radix: Two lines tangent to the glabella and to the nasal dorsum, intersecting at nasion, define the nasofrontal angle. The nasofrontal angle (radix) should lie between the superior lash line and the supratarsal crease, with the nasion approximately 15 mm anterior to the medial canthus. The ideal nasofrontal angle varies by gender, with 130 degrees considered acceptable in White men versus 134 degrees in women.
Nasal length, dorsum, and supratip: The ideal nasal length (nasofrontal angle to the tip-defining points) is equivalent to two-thirds of midfacial height, the stomion-to-menton distance, or to chin vertical. The nasal dorsum should be smooth, with a slight supratip break in women, roughly 2 to 3 mm above the tip-defining points. In male patients, the dorsum should follow a line drawn from the radix to the tip-defining points, while in women, it should be along a parallel line approximately 2 mm more posterior. The nasal dorsum should be smooth, with a slight supratip break in women, roughly 2 to 3 mm above the tip-defining points. In male patients, the dorsum should follow a line drawn from the radix to the tip-defining points, while in women, it should be along a parallel line approximately 2 mm more posterior. A supratip break is accomplished through creating tip-defining points with good projection and reducing the dorsum to the desired effect.
Tip projection: Projection is considered ideal when 50 to 60% of the tip lies anterior to a vertical line adjacent to the upper lip or represents 0.67 times the ideal nasal length.
Tip rotation: Tip rotation is determined by the nasolabial angle and should equal approximately 90 to 95 degrees in men and 95 to 100–110 degrees in women.
Alar–columellar relationship: The ideal alar–columellar relationship is 2 to 3 mm of columellar show in the lateral view. Excess columellar show is associated with a hanging columella or a retracted ala.
Periapical hypoplasia: Skeletal (maxillary) or soft tissue deficiency may produce periapical hypoplasia. Augmentation of the pyriform aperture can decrease the apparent size of the nose, increase the nasal tip and base projection, and widen the nasolabial angle.
Lip–chin relationship: Chin projecting surface should lie approximately at (preferred in men) or up to 3 mm posterior (in women) to a vertical line drawn from the half-distance point of the ideal nasal length and tangential to the upper lip vermilion anterior-most point.
Use the base view to assess 5 areas: Nasal projection (Fig. 14.2), nostril shape/symmetry, columella symmetry/width, alar base, and alar flaring (Fig. 14.3).
Nasal projection: On basal view, the nose should create an equilateral triangle with a columella-to-lobule ratio of 2:1.
Nostril shape/symmetry: The nostrils should be symmetric and have a teardrop shape with a long axis extending from the base to apex. The ideal nostril–tip relationship should be approximately 2:1.
Columella symmetry/width: The ideal columella requires a smooth concave shape bridging the nasal tip and nasolabial junction. Primary (intrinsic) deformities of columella originate from malpositioned medial crura or excessive soft tissue. Most commonly, a widened or asymmetric columella results from premature or excessive medial crura flaring.
Alar base and flaring: Proper assessment of nasal base width requires a clear distinction between the width of the alar base and the degree of alar flare. Ideal nasal width approximates the intercanthal distance (normal, 31–33 mm). Alar flare is defined as the greatest width of the ala, whose convexity should not exceed 2 to 3 mm lateral to the alar–facial crease.
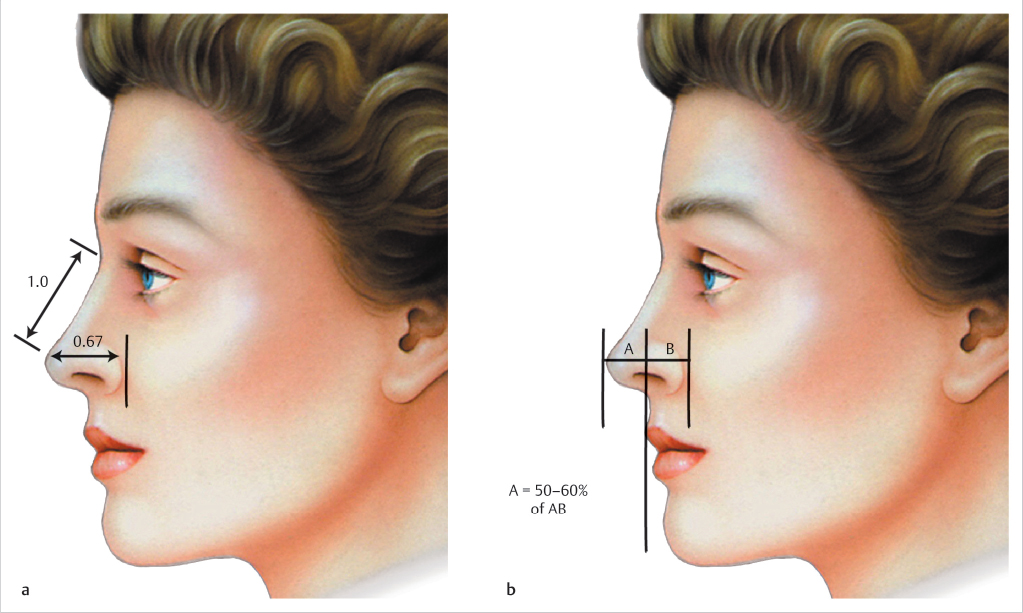
Fig. 14.1 (a, b) Ideal nasal projection on the lateral view. About 50 to 60% of the tip should lie anterior to a vertical line drawn adjacent to the most projecting part of the upper lip and can also be measured as 0.67 times the ideal nasal length. (Reproduced with permission from Rohrich R, Adams W, Ahmad J, eds. Dallas Rhinoplasty: Nasal Surgery by the Masters. 1st ed. Thieme; 2014.) 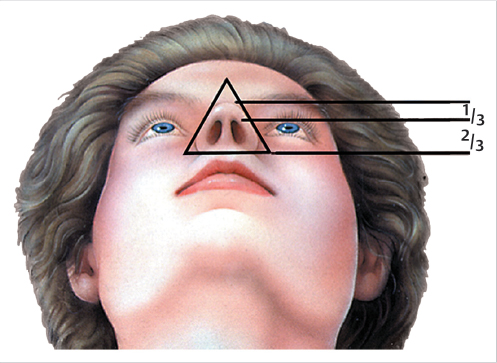
Fig. 14.2 Ideal nostril–tip relationship should be approximately 2:1 on the basal view. (Reproduced with permission from Rohrich R, Adams W, Ahmad J, eds. Dallas Rhinoplasty: Nasal Surgery by the Masters. 1st ed. Thieme; 2014.) 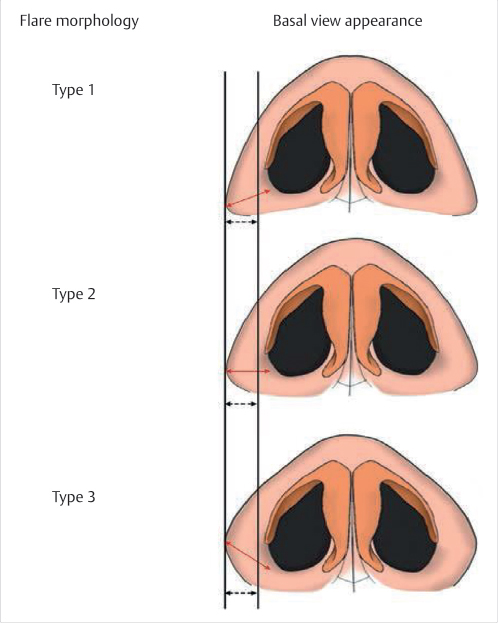
Fig. 14.3 Classification of alar flare.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


