Abstract
The approach to the crooked nose is determined by thoughtful analysis of the face in its entirety, including all of the components of the nasal structure and function. Attention to correction of deviated nasal bones, septum, dorsum, and base, as well as associated turbinate hypertrophy is critical to successful outcomes.
19 The Crooked Nose
Key Points
A deviated nose is almost invariably associated with some degree of nasal dysfunction.
Circumspect examination of the entire face, the external nasal frame, and internal nasal structures is crucial in avoiding residual or persistent deviations, which may be multifaceted.
The intersecting point of the eyebrows should not be used for judging the nose alignment since often this is altered by the patients differentially to place the deviated nose in the center of the eyebrows.
19.1 Preoperative Steps
19.1.1 Analysis
A detailed patient history including nasal trauma, prior surgery, airway complaints, and allergies is obtained.
Thorough preoperative analysis is performed, including the external nose and face, oral or nasal breathing, overall symmetry, occlusal plane canting, nose alignment with other facial structures, chin position, intercanthal midline, palatal arch, and facial nerve function.
The nose is observed zone by zone for deviated structures, including the nasal bones, anterior septum, and upper and lower cartilages with basilar and overhead views. The presence of nasal valve incompetence, internal septal deviation, turbinate hypertrophy, synechia, perforation, spurs, contact points, ulceration, and polyps is assessed.
Examination is repeated after vasoconstriction of the nasal mucosa using phenylephrine or ephedrine sulfate.
Review of a computed tomography scan may be performed in patients reporting frequent sinus headaches, infections, or migraine headaches to detect underlying sinusitis, concha bullosa, septa bullosa, and contact points.
19.2 Operative Steps
See Video 19.1.
19.2.1 Correction of Deviated Nasal Bones
Onlay Grafting
Under general anesthesia, the face is prepped and nasal vasoconstriction achieved.
An intercartilaginous incision is made or an open approach is used and the target nasal bone is exposed. The periosteum is elevated in limited fashion.
A septal or conchal cartilage graft in the form of a single or double layer is gently crushed. Depending on the degree of the nasal bone shift, diced cartilage or a layer of soft tissue, such as dermis or fascia graft, is applied in the subperiosteal plane and molded in place.
The incision is repaired loosely to allow for drainage.
Unilateral Out-fracture
Through a small vestibular incision at the pyriform aperture, the periosteum is elevated using a Joseph’s periosteal elevator.
A low-to-low osteotomy is made and the nasal bone is out-fractured.
A spreader graft is placed via a 3-mm incision in the mucoperichondrium immediately caudal to the junction of the upper lateral cartilage and the septum anteroposteriorly. A septal elevator is used to create a pocket and the graft is inserted between the septum and the upper lateral cartilage.
A piece of folded Adaptic or Surgicel saturated in Bacitracin ointment is placed between the nasal bone and the septum and kept in place for at least 1 week. The patient is maintained on systemic antibiotics during this period.
19.2.2 Correction of Deviated Septum
An open technique is employed with concomitant rhinoplasty, or an L-shaped (Killian) incision is used for a closed approach.
Mucoperichondrium of the left side of the septum is elevated beginning with the caudal septal angle.
Once the correct, glistening, greyish cartilage plane is exposed, the blunt end of a periosteal elevator is used to raise the mucoperichondrial flap posteriorly, cephalically, and caudally.
An L-shaped incision is carried through the quadrangular cartilage using the sharp end of a septal elevator, leaving at least a 15 mm wide L-strut anteriorly and 10 mm caudally.
The caudal portion of the septal cartilage is gently separated from the maxillary crest of the vomer bone using the sharp end of the septal elevator. Cartilage is separated from the perpendicular plate of the ethmoid bone in similar fashion and subsequently removed.
Deviated portions of the vomer bone and perpendicular plate are removed as extensively as necessary to eliminate the internal deviations and the spur posteriorly.
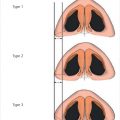
Any midvault deviation is the consequence of septal deviation and five out of six classes of septal deviations described by the senior author could be involved in nasal deviations.
Septal Tilt (Fig. 19.1)
The septal tilt is corrected initially by removing the posterocaudal portion of the septum, leaving an L-strut septum anteriorly and caudally.
It is crucial to disengage the dislodged caudal and posterior portions of the retained L-strut from the vomerine groove and anterior nasal spine.
Overlapping redundant caudal portions of the septal cartilage are removed to provide a “swinging door” type free movement of this cartilage.
The anterior nasal spine is palpated between the right thumb and index finger to ensure it is in midline position. If it is deviated, a greenstick fracture is performed to allow repositioning.
The septum is repositioned and fixed to the periosteum of the anterior nasal spine using a figure-of-eight 5–0 PDS suture.
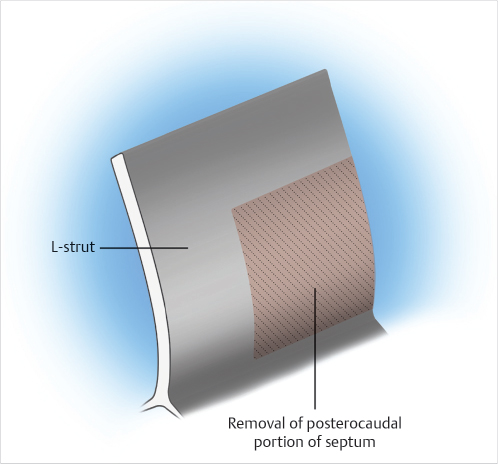
Fig. 19.1 Septal tilt.
Correction of Anteroposterior C-Shaped Deviation (Fig. 19.2)
Resection of the posterocaudal portion of the septum is performed as described previously. Osteotomy of the anterior nasal spine and residual vomer plate is often necessary in order to reposition this structure in the midline.
Release of tension by removal of the posterior and caudal portion of the cartilage and creation of a swinging door-type movement will often eliminate the C-shaped cartilage deformity.
Otherwise, cephalocaudal-oriented scoring of the concave surface of the L-shaped frame is performed, although this is seldom necessary.
Bilateral extramucosal stents are placed and fixed in position with a through-and-through suture to mold the cartilage during healing. These are left in place for at least 2, preferably 3, weeks.
Anterior deviation of the nose is corrected by separation of the upper lateral cartilages from the septum, osteotomy, repositioning of the frame, differential trimming of the upper lateral cartilages, and placement of spreader grafts, often without scoring.
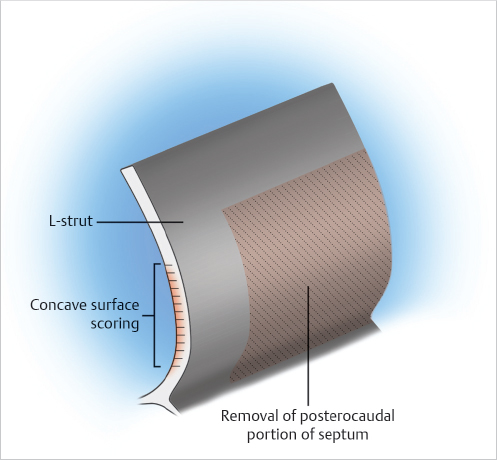
Fig. 19.2 Correction of anteroposterior C-shaped deviation.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


