Abstract
Alar base surgery is a powerful aspect of rhinoplasty. Due to the changes imparted by maneuvers that adjust tip projection, this portion is performed as the last step of the open rhinoplasty. Alar base width and alar flare are two separate entities. Management for them can be separate or combined depending on each case. The three-dimensional nature of the alar base requires detailed analysis and consistent points of reference for marking base width and flare reductions. A systematic approach to managing increased alar base width and/or alar fare will aid in achieving consistent results.
27 Alar Base Surgery
Key Points
The alar base is the caudal-most point of the nasal ala at the alar–facial junction.
Alar base width should approximate the intercanthal distance (31–33 mm).
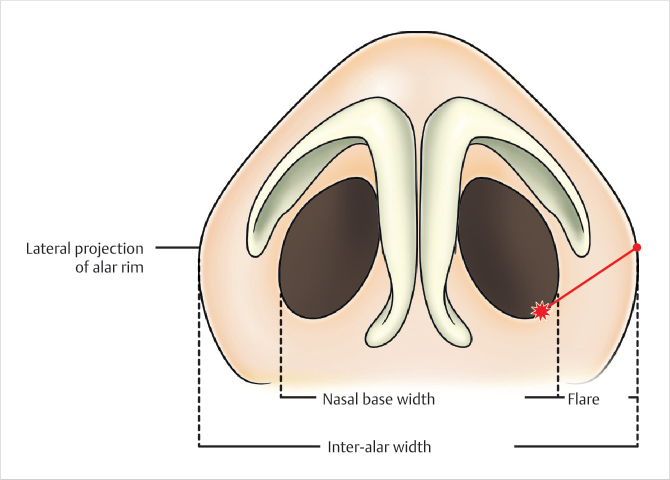
Interalar distance is the distance between the lateral-most points of the ala.
Alar flare is present when the interalar distance is greater than the alar base width (Fig. 27.1).
A larger degree of alar flaring is accepted in non-Caucasian patients.
Alar flare and alar base reduction are not mutually exclusive but represent separate anatomic entities.
27.1 Preoperative Steps
Preoperative assessment of the alar base is performed from the basal view.
Both alar base width and interalar distances are measured.
A difference greater than 2 mm between these values on each side defines alar flare.
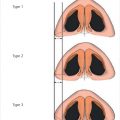
Rohrich et al describe four morphologies of alar flare depending on the location of the lateral-most point along the ala in comparison to the nasal base.
Type 1: Lateral point is close to the alar–facial groove and is inferior to the level of the sill–base junction.
Type 2: Lateral point is at the same level of the sill–base junction.
Type 3: Lateral point is superior to the level of the sill–base junction.
Type 4: This is a combination of Type 3 flare with a widened nasal base.
27.2 Operative Steps
See Video 27.1.
Changes in nasal tip projection and rotation directly influence alar base width and flare.
The decision to perform alar base and/or alar flare reduction should be made at the completion of the rhinoplasty after the transcolumellar incision has been closed.
If the indication is not clear, reduction is postponed until postsurgical swelling has subsided in 6 to 12 months.
Alar flare reduction is a powerful technique to reduce interalar distance without the scar burden associated with more aggressive techniques for alar base medialization.
The goal of flare reduction is to reduce nostril flare and improve nasal harmony.
Understanding the alar flare type aids in excision design.
The excised amount progressively increases with each type (1 through 3).
Alar flare reduction marking (Fig. 27.2):
Point 1: The lateral-most point is marked at the alar–facial groove.
Point 2: The sill–base junction is marked.
Point 3: A point 2 mm inferior to the sill–base junction is marked.
Line 1: A curved line in the alar–facial groove is made from Point 1 to Point 3.
Line 2: A curved line along the ala is made from Point 1 to Point 3 creating a final ellipse. The width of the ellipse increases with the degree of alar flare (Types 1 through 3).
If the inferior incision is made more than 1 mm above the groove, one risks having a visible scar.
The medial corner of the elliptical excision should not go beyond the sill–base junction, into the nasal sill. Incisions in this region will narrow the nasal sill and further distort the nostril size.
It is always safer to take less tissue, allowing a milder degree of alar flare, than to overresect and distort the nasal harmony.
Alar base reduction marking (Fig. 27.2):
Alar base reduction can be performed either with or without alar flare reduction.
When performed with alar flare reduction, a nostril sill excision is performed to narrow the base width.
Starting from Point 2, an elliptical excision of the nasal sill is performed in the sagittal plane to narrow the base width.
The sill–base junction should be preserved.
The sill–base junction to columellar–sill junction should be equivalent on both sides.
Surgical technique:
Infiltrate 0.25% Marcaine with 1:100,000 epinephrine at the proposed flare reduction site.
Using a #15 blade, the marked wedge is excised including the skin and subcutaneous tissue. It is important not to excise the deeper layers including the muscle.
Hemostasis is achieved with a fine tip electrocautery.
Closure is performed in one layer using simple interrupted 6–0 nylon sutures.
Deep sutures are not advised as they run a high risk of extrusion and inflammatory scarring in this area.
During closure, the first stitch should be placed where the curvature of the alar rim meets with the upper lip.
Every stitch should be meticulously placed including full-thickness bites of skin and subcutaneous tissue.

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


