Summary
Upper and lower blepharoplasty are among the most popular and safe surgical procedures. Blepharoplasty is performed for both cosmetic and functional indications in a wide variety of ages. Although the incidence of complications is low, complications can and do occur. The avoidance of complications involves an optimal assessment of the patients underlying anatomy and the selection of appropriate blepharoplasty and ancillary procedures.
19 Blepharoplasty
19.1 Introduction
Blepharoplasty is one of the most common cosmetic procedures performed in the United States. 1 Although it may be considered one of the least invasive cosmetic surgeries, it is not without complications. These complications can range from mild issues that resolve spontaneously to devastating and permanent damage to associated structures. In this chapter, blepharoplasty-related complications and their recognition and management will be presented. In addition, preventative measures will be discussed in order to minimize the incidence of these complications.
19.2 Patient Evaluation
A thorough preoperative patient evaluation is an important first step to limit the risk of postoperative complications. For example, systemic diseases such as thyroid disease should be investigated as it can affect eyelid position and eyelid edema. 2 In addition, ocular, facial, and skin abnormalities such as dry eyes, narrow chamber angles, facial nerve dysfunction, blepharitis, eczema, rosacea, blepharospasm, and visual acuity/visual field are among the issues that should be noted and documented.
Identifying abnormal and undesirable periorbital anatomical characteristics in the patient is necessary in order to choose the appropriate surgical technique. When preparing for an upper blepharoplasty, various anatomical attributes should be assessed. For example, the amount of skin, symmetry of eyelid creases, the amount and location of protruding fat, presence of orbital hollowing, blepharoptosis, lid position, and position of the lacrimal gland and eyebrow all need to be noted. These findings should be discussed with the patient preoperatively and adjunct procedures offered as necessary. If these undesirable periorbital anatomical characteristics are undiagnosed, the surgical results may be suboptimal.
In the examination of the lower eyelid, the amount and location of fat pseudoherniation, excess skin, the presence of tear trough deformity, the presence of a negative vector midface or midface deficiency, and malar bags/festoons should be noted. These findings may determine the type of surgery performed. Patients with negative vector and midface deficiency should be educated on the limitations of surgery and outcome due to their anatomical features. The lower eyelid support should be assessed. If laxity is noted, a horizontal shortening or other tightening procedure may be necessary at the time of the blepharoplasty to prevent postoperative lid malposition.
19.3 Common Postoperative Problems: Their Avoidance and Correction
19.3.1 Upper Eyelid Blepharoplasty Complications
Brow Ptosis
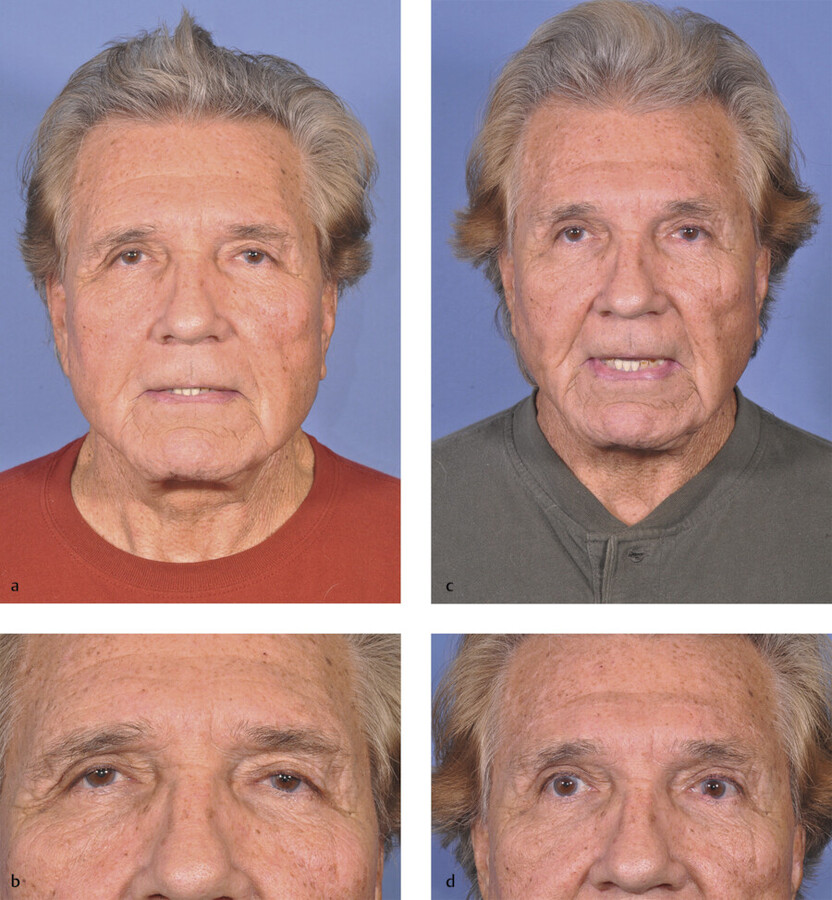
The preoperative recognition of a ptotic brow is essential for a satisfactory upper blepharoplasty result. The patient may require a brow lift instead of, or in addition to, an upper blepharoplasty procedure. It is observed that when the upper eyelid skin is removed, the distance between the eyebrow and the eyelid margin is shortened. Consequently, an uncorrected brow ptosis may be more noticeable after surgery, resulting in a seemingly less effective blepharoplasty. 3 Therefore, when brow ptosis is noted, patients should be advised on procedures available to reposition the eyebrow prior to or at the same time as an upper blepharoplasty (Fig. 19.1).
Blepharoptosis
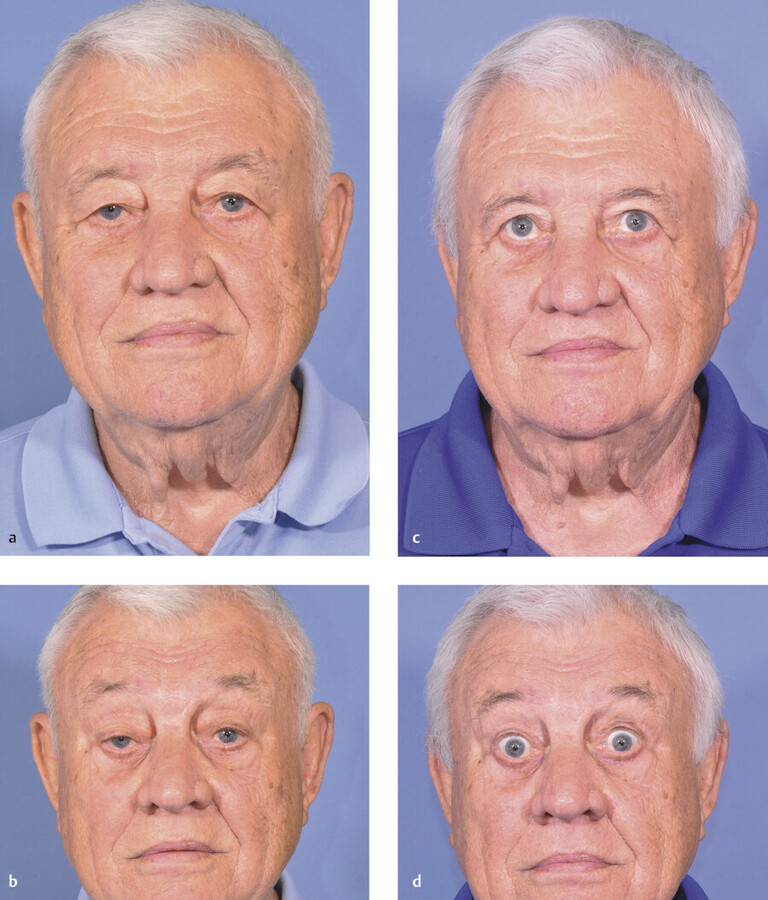
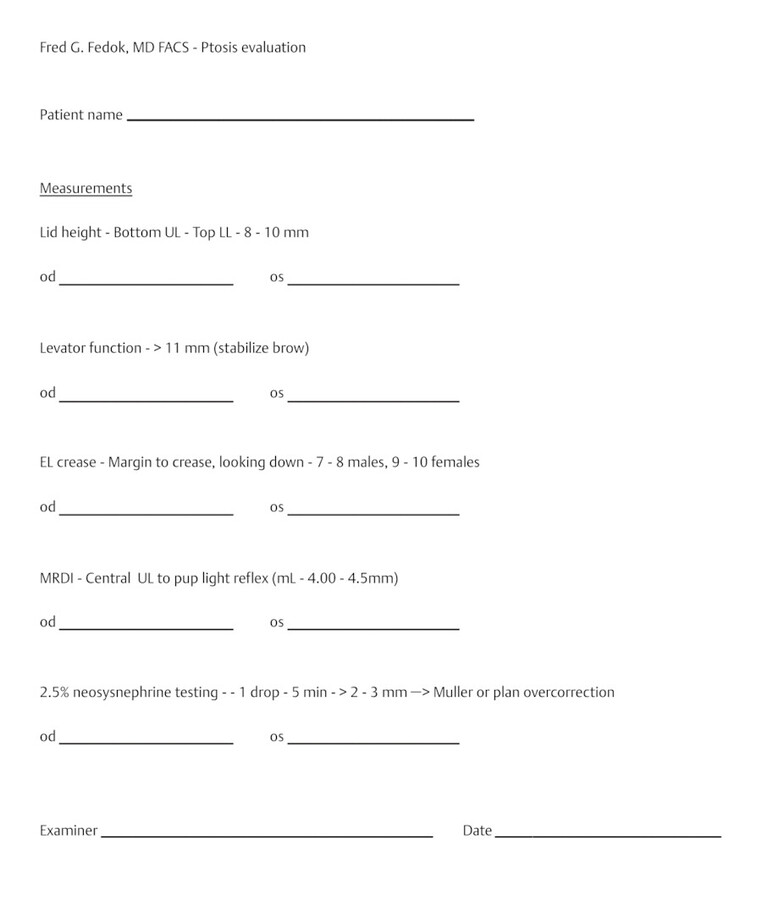
If upper eyelid ptosis is noted preoperatively, it should be evaluated and documented with specific measurements. This includes assessing the height of palpebral fissure, the distance between the upper eyelid margin to the corneal light reflex (MRD1) and levator muscle function. These findings should be discussed with the patient and if clinically significant, a ptosis repair procedure should be considered to be performed at the same time as upper blepharoplasty. The documented findings may also be helpful to secure insurance coverage of the procedure (Fig. 19.2, Fig. 19.3). A transient postoperative blepharoptosis can also be seen soon after blepharoplasty surgery and is thought to be caused by edema, diminished levator or Müeller muscle function, or hematoma formation. 4 , 5 , 6 This transient phenomenon usually resolves spontaneously. On the other hand, if postoperative ptosis persists for more than 3 to 6 months, an inadvertent disinsertion of the levator aponeurosis may have occurred during resection of the orbicularis muscle or preaponeurotic fat. 3 In order to correct this problem, a secondary levator advancement procedure may be needed. To avoid this particular complication, it is important to recognize that the levator muscle is immediately posterior to the central fat pad and a prudent dissection should be performed during blepharoplasty surgery.
Persistent Dermatochalasis
Inadequate removal of excess upper eyelid skin will result in persistent dermatochalasis. Although this may be considered a suboptimal result, it behooves the surgeon to maintain a conservative approach in removing excess skin in upper blepharoplasty as lagophthalmos from overly aggressive skin excision may be difficult to correct. It is, therefore, best to educate patients on the importance of conservative skin excision and that in this situation less is better. Patients should also be instructed that later additional skin removal as an in-office procedure, if needed, is always a possibility without a compromise of the final cosmetic result.
To assess how much skin can be safely removed during upper blepharoplasty, the “pinch” technique may be considered as a safe and effective method to be used during preoperative marking. First, the patient is placed in an upright position. Planning markings are made with a surgical marking pen. The inferior aspect of the proposed eyelid incisions is marked first. At the central portion of the eyelid, this marking and subsequent incision is usually placed at or just inferior to the supratarsal crease, or 8 to 10 mm from the ciliary margin. Medially, this incision is carried to the level of the puncta, but no further medially to avoid webbing of the incision. Laterally, in females, the incision is commonly carried to approximately 1 cm over the orbital rim and usually placed in a lateral eyelid crease. In males, the lateral extent of the incision is planned to terminate with only a minimal crossing onto the lateral orbital rim.
In marking the skin, one must verify that eye closure will be complete with the amount of skin excised, and hence, there should be a certain conservatism during the planned marking of the skin (Fig. 19.4). The excess eyelid skin is grasped with smooth forceps. The tines of the forceps are adjusted to approximate the amount of skin to be removed while maintaining the lower tine of the forceps on the planned inferior incision and gently pinching the skin. This is repeated at several positions along the eyelid to determine some of the points for the placement of the upper eyelid incision. 7 While holding the excess skin between the forceps’ tines, the eyelid should be observed to still be able to be closed. The incisions should be planned to be limited to the thinner upper eyelid skin and to not extend into the thicker infrabrow skin. Often the thinner eyelid skin that can be removed has a different color and texture than the surrounding skin. The position of the brow should also be noted and should not be disturbed by this process. The amount of skin between these superior and inferior incisions varies between patients. Even in the same patient it can vary between the left and right eyes. It is important to avoid excess skin excision as this can cause lagophthalmos and problems with dryness. Note that when the eyes are closed, there should be complete closure of the eyelids. The lateral aspect of the incision should be designed along a diagonal (parallel to the crow’s feet) so that lateral hooding is reduced during skin excision.

Scarring
Significant postoperative scarring of the upper eyelid skin is unusual after blepharoplasty as the overlying skin is very thin and heals very fast compared to other parts of the body. Darker pigmented skin types, however, are more prone to pigmentary changes and hypertrophy after surgical procedures. Therefore, the use of current CO2 laser technology for making skin incisions on darker pigmented skin such as Asian and Black patients should be avoided. 8 In addition, extending the incision lateral to the orbital rim should be minimized in these patients to avoid the creation of a noticeable scar.
Once an incision is made, a meticulous closure is crucial. Similarly, removing the sutures in a timely fashion, usually in about 3 to 7 days, and using a nonreactive suture, such as polypropylene, are important in minimizing chances of scarring and granuloma formation.
Lagophthalmos
Lagophthalmos can occur after upper eyelid blepharoplasty because of several reasons. It occurs most commonly after the removal of too much upper eyelid skin. As a general guideline, the amount of remaining intact skin after blepharoplasty excision should be anticipated during surgical marking as noted previously. It is recommended that at least 20 mm of skin should be retained between the inferior aspect of the eyebrow and the lid margin to prevent lagophthalmos. If it is recognized that too much skin has been removed at the time of surgery, the excised skin can be immediately sutured back in place as a skin graft. Alternatively, if excessive excision is of lesser concern during the surgery, the removed skin may be stored in saline gauze and refrigerated. If considering this there are some associated risks that should be carefully considered. (Considering the risks the first editor does not use this technique.) This can be used 1 to 2 weeks after surgery if needed. 9
Lagophthalmos can also be seen without excessive removal of skin. Postoperative middle lamellar cicatrix formation may occur when the orbital septum is inadvertently included during levator aponeurosis advancement, eyelid crease formation, or wound closure. 9 The resolution of this type of lagophthalmos may require the surgical lysing of adhesions between the orbicularis muscle, the septum, and levator aponeurosis.
Minor degrees of lagophthalmos will usually resolve over a few weeks as edema subsides and orbicularis function recovers. In the meantime, the ocular surface should be protected by advising eye lubricants and ointments while closely monitoring patients. Taping the eyelids at night may also help prevent excessive drying related to the lagophthalmos. If this is ineffective, a consultation with a cornea specialist may be warranted. If lagophthalmos does not improve with time, additional surgery, including skin grafts or other procedures, may be required.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


