Summary
Thread lifts have been available since 2002. Some of the complications related to these procedures were due to the use of nonabsorbable sutures for these procedures. More recently absorbable sutures have been used. This has been associated with a lower complication rate. The more frequent complications include bruising and puckering. Mild to moderate puckering is usually self-limited. Severe puckering is usually technique dependent. This may need to be treated with partial or complete removal of the thread. Although uncommon, infections have occurred requiring antibiotic therapy.
16 Thread Lift
16.1 Introduction
Threadlifting, or suture suspension, has emerged as a minimally invasive option for facial rejuvenation in patients who are looking for affordable options without downtime. 1 , 2 Although other such modalities such as neurotoxins, injectable fillers, lasers, and energy devices remain popular, they may not lift or reposition the underlying ptotic tissues. 1 , 3 , 4 Thread lifts can be used to reposition ptotic tissues. With threadlifts, recovery time is usually short, large incisions are avoided, 5 and general anesthesia is not needed 4
Traditionally, threadlifting involves passing threads underneath the skin surface to lift the tissue. Threads are placed along a planned trajectory, pulled to lift the skin, secured and trimmed at the entry point. 6 , 7 Threadlifting for facial rejuvenation was introduced by Sulamanidze and colleagues in 2002. 8 These authors used bidirectional, nonabsorbable barbed suture thread (APTOS) to lift ptotic facial tissues. APTOS threads were manufactured with nonabsorbable polypropylene and designed for use in freely mobile tissue. The threads also had barbs cut at an angle and organized so they faced the midline in a bidirectional manner (Fig. 16.1). 9

Modifications of these original sutures have since been introduced, 10 each with specific features and techniques for insertion. 11 Longer than APTOS threads, bidirectional threads were made of nonresorbable polypropylene with dents to create slant edges and sharp ends to hold tissue firmly. 9 , 12 Contour threads (Surgical Specialties, Corp., Reading, PA) were nonabsorbable polypropylene unidirectional threads with barbs in a helical design like DNA. The Contour thread could be fixed at the proximal end to the deep temporal fascia or other nonmobile structure. These threads received FDA clearance for midface suspension in 2005. 9
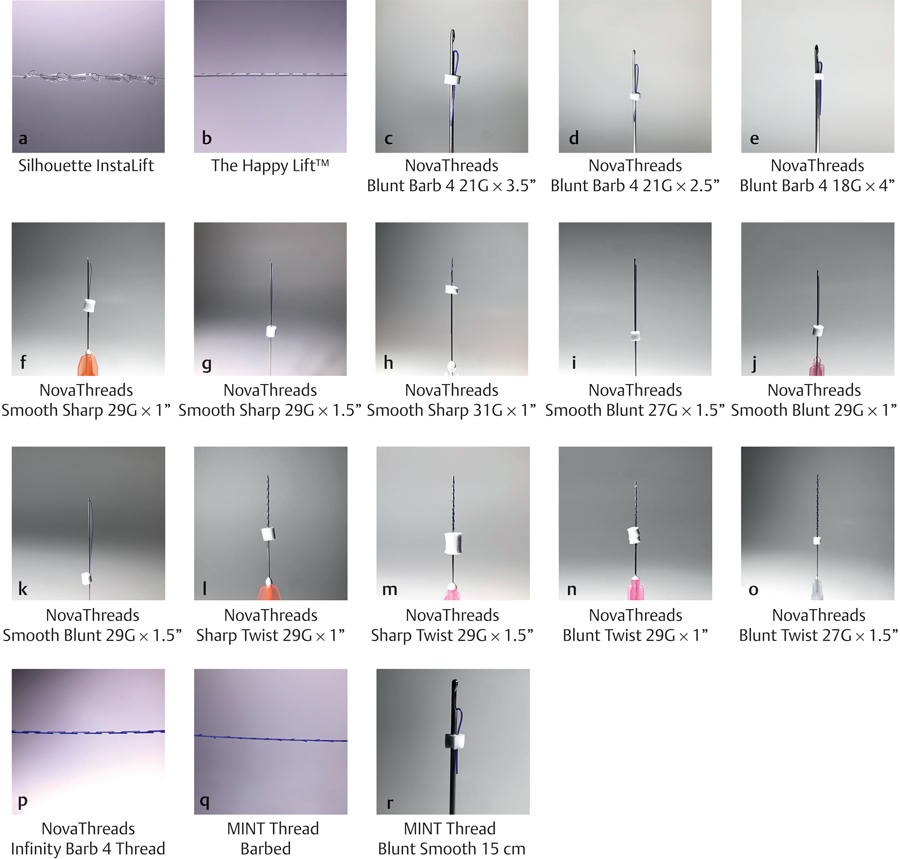
Silhouette Soft threads (Sinclair Pharma, London, United Kingdom) consist of poly-L-lactic acid (PLLA), a biocompatible and biodegradable polymer used in biomedical and pharmaceutical applications. 10 This absorbable suture has bidirectional cones designed to lift the eyebrows and reposition the cheek, lower jaw, and neck. The cones are made of absorbable poly lactide/glycolidecopolymer (PLGA). 13 The Silhouette InstaLift is an absorbable suspension suture with cones oriented bidirectionally along the suture. 14 Sutures and cones are made with PLGA and PLLA. The Happy Lift™ (Promoitalia International S.r.l, Naples, Italy) is an absorbable, monofilament suspension thread made of caprolactone and polylactic acid. 15
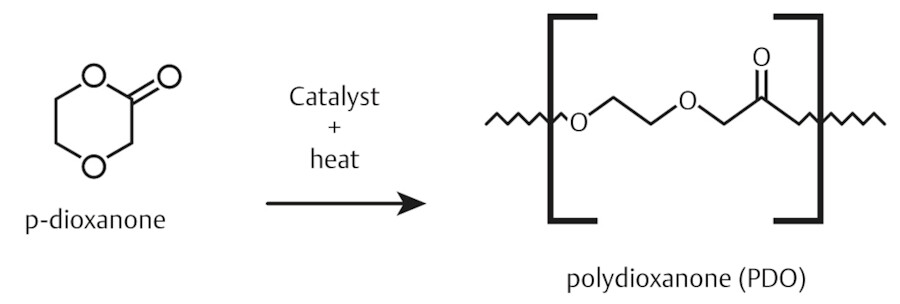
The major paradigm shift in threads occurred with the introduction of dissolvable materials expected to completely dissolve within 6 to 24 months. The materials used for these threads worldwide include polydioxanone (PDO), polycaprolactone (PCL), and poly-L-lactic acid/polyglycolic acid (PLLA/PLGA). Currently in the United States, the only two approved types of dissolvable threads are PDO and PLLA/PLGA, although it is anticipated that PCL will enter the market in the near future.
The most popular type of threads used in the United States and worldwide is PDO, and thus the rest of this discussion will focus on this type. PDO is a synthetic monofilament polymer and can be used as a lifting suture to suspend ptotic tissues of the face or body, or both (Fig. 16.2). PDO sutures are more pliable than their polypropylene counterparts and have more strength than other absorbable sutures. 16 Knotless PDO threads lift tissue with barbs, cogs, or molds, which adhere to tissues when the thread is inserted. This creates tension in the thread that lifts the skin tissues. The effect increases over time as collagen forms around the threads, cogs, and barbs. 2 , 12
PDO threads (NovaThreads Inc., Miami, FL) are the subject of a case report of a patient presenting with sagging jowls after injection of fillers into her perioral area. 17 Fillers were used simultaneously in areas of volume and bony deficiency to enhance the result achieved by the threads because the lifting procedure may reveal volume deficits that can be corrected with dermal fillers. The procedure was well tolerated with only transient mild swelling at the insertion points (Fig. 16.3).
PDO threads have been used extensively for aesthetic applications in Korea. The thread resembles a V-shape, with half of the thread residing outside the needle and the rest inside the caliber. The needle or caliber is inserted, and then removed, causing the thread to be fixed inside the skin without anchorage or knots. 18
PDO threads are completely absorbed within 8 months after insertion with minimal foreign-body reaction. 11
Reported novel uses of PDO threads include hair stimulation and treatment of hyperdynamic muscle movements with subsequent improvement of rhytids. 19 , 20
16.2 Complications
When discussing complications of threads it is important to discern between dissolvable threads and nondissolvable threads. In general, the complications associated with nondissolvable threads are far more frequent and problematic than their dissolvable counterparts. It is important to understand and recognize the complications of permanent threads as the predecessors of today’s modern and higher tech dissolvable threads.
Threadlifting with permanent threads may be accompanied by a variety of complications which include:
Infection, rippling and puckering, asymmetry, granuloma formation, thread loss, and thread breakage. 7
Nerve damage and hematoma formation. 2
Chronic pain, hypersensitivity, palpability, and sensory impairment. 21
Erythema, ecchymosis, facial asymmetry, thread migration, skin dimpling, and scar formation. 1 , 18 , 22 , 23
Wu and colleagues 12 treated cheeks and jowls with APTOS threads and reported thread migration (7.8%), infections and granuloma (4.9%), palpable thread ends with pain (10.8%), and dimpling with irregular wavy skin (4.9%) caused by superficial placement of threads. Threads had to be removed in all these patients. Wu and colleagues also performed WOFFLES thread lifts of the midface and jowls with results similar to those of a traditional face lift. Reported complications include knot palpability or knot exposure in the scalp, small granuloma and dimpling at the insertion point. Exposed knots were removed and the thread was cut even with the skin; dimpling was resolved by secondary skin release.
Contour threads have been evaluated as the primary procedure in four studies, 1 , 6 , 24 , 25 as well as in combination with other procedures. Efficacy was variable and unpredictable, 9 while reported complications included:
Bruising, swelling, and pinching. 24
Skin dimpling and visible knots. 6
Swelling, ecchymosis, infection, thread extrusion, palpable threads, contour irregularity, and recurrent laxity. 25
Intractable pain, dimpling, visible and palpable thread, thread extrusion, paresthesia, and foreign body reaction. 1
Contour threads lost FDA approval due to numerous postoperative complications. 7
De Benito and colleagues studied Silhouette Soft threads over a mean follow-up time of 18 months. 26 Results were reported as “good, with high patient satisfaction.” Complications reported were moderate pain in the temporal area, visible dermal pinching, temporal hematoma, asymmetry, and palpable sutures.
Lorenc and colleagues 14 described how to prevent and treat complications associated with the Silhouette InstaLift in detail. Swelling due to lidocaine injection is common and resolves within several days. Prior to the procedure, patients are advised to discontinue medically unnecessary supplements that may increase bruising (e.g., vitamin E, garlic, ginger, ginkgo). Hypersensitivity, though rare, may be treated with steroids. Irregularity and cellulitis after placement of Silhouette InstaLift sutures is possible and was recently observed and treated by the author.
This chapter describes in detail the complications associated with PDO thread lifting and how to prevent and treat them.
16.3 PDO Threads
Complications of PDO threads have been reported 1 , 3 , 11 , 17 , 18 , 19 , 22 , 23 , 27 , 28 , 29 , 30 , 31 , 32 , 33 and are summarized in Table 16.1.
An early study 1 (Table 16.1) using barbed suture lifting in 29 patients showed that adverse events occurred in 69%, and early recurrence of skin laxity was noted in 45% of patients. Suh and colleagues 18 in their 31-patient study reported that 27 patients (87%) were satisfied with their PDO results while 4 patients (13%) were not satisfied. Complications included bruising (93.5%), mild postprocedure swelling (90.3%), and mild asymmetry (6.5%). These adverse events resolved within 2 weeks without treatment.
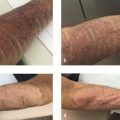
A case of mycobacterium infection after PDO thread-lift insertion has been reported by Shin and coworkers. 27 The thread-lift procedure was performed in a nonmedical cosmetic beauty salon 6 weeks before the patient presented to a hospital with itchy erythematous plaques on both cheeks. The patient had received 1 week of antibiotic therapy without improvement. Numerous cultures and stains to identify the infecting organism were negative until nontuberculous mycobacterium infection became apparent using reverse transcriptase-polymerase chain reaction, and the use of an erm gene polymerase chain reaction restriction fragment length polymorphism kit revealed the presence of Mycobacterium massiliense. The cutaneous lesion was significantly improved after 2 months of treatment with clarithromycin and amikacin. Triamcinolone intralesional injections at each visit helped to decrease the lesion size.
Kang and colleagues, 22 in treating glabellar and forehead wrinkles in Korean patients, reported skin ulceration in two patients and thread extrusion in one patient, both events attributed to inserting the threads too superficially. Resolution was achieved by removing the threads.
Karimi and Reivitis 17 reported mild swelling in the lower face which resolved without intervention 7 days later.
Yeo and coworkers28 reported early complications from absorbable anchoring sutures after PDO thread lifts for facial rejuvenation in 144 patients. The average follow-up time was 11.1 weeks (range 0–52 wk). Complications developed in 11.1% of patients. These events were thread exposure, dimples, alopecia, undercorrection, asymmetry, and parotid gland injury. Thread exposure was noted in five patients. In two cases the thread was removed because it was palpable 1 month after thread lifting. In the other three patients the thread was removed at 2 months. Thread exposure was attributed to migration of the thread to a superficial layer followed by an inflammation reaction. Dimpling developed in three cases. One appeared after 5 days and was resolved by lightly retouching the entire area. In another case dimpling appeared at 3 weeks and disappeared 3 months after cannula dissection of the dimple.
Alopecia was noted in three patients and resolved after 5 months. This complication did not occur after widening the anchor gap. Alopecia was attributed to ischemia due to tension in the anchoring process. Undercorrection developed in two cases at 1 month and in one case at 6 months. Asymmetry was noted in one patient at 4 months. The authors suggest that an additional thread lift should be performed only after swelling from the initial lift has subsided.
Parotid gland injury occurred in one patient. When antibiotic therapy relieved symptoms only temporarily, ultrasonography at 3 months showed that the thread had passed through the parotid gland. The condition resolved 5 months later after observation and conservative treatment (i.e., retouching or widening the anchoring gap). Lawson and colleagues 34 recommend that to avoid this dangerous complication, thread lifting should be performed “carefully at the inferior side of the parotid gland and from the posterior side of the masseter to the mandible angle because they are tightly attached to superficial facial fascia and parotidomasseteric fascia.”
Kim and coworkers, 29 in their 22-patient, 7-month study, reported transient edema and erythema. Yarak and colleagues 30 treated mild-to-moderate sagging of the middle and lower face in six patients. All patients experienced pain of moderate intensity at the insertion point immediately after the procedure and two patients reported ecchymosis.
Lee and colleagues, 31 in their 35-patient study reported mild swelling, bruising, and skin dimpling after PDO thread lift, all of which resolved without surgical intervention. One patient experienced asymmetry which was corrected with a repeat procedure.
Ali 32 reported outcomes of patients treated with PDO threads for facial rejuvenation over a 2-year period. Among 21 patients treated with PDO alone, one patient experienced thread breakage, which the author attributed to technique during the procedure. Specifically, the subcutaneous plane was missed during thread insertion and penetrated the superficial dermis, and then attempted to redirect into the subcutaneous plane. As a result, the thread was broken and had to be withdrawn.
Unal and colleagues 23 studied 38 patients treated with bidirectional barbed PDO cog threads (DongWon Medical Co. Ltd, Bucheon, Korea) for facial rejuvenation. After insertion of the threads, they prevented migration by tying threads in the same entry point to each other and burying the remaining threads into subcutaneous tissue using an 18-gauge needle. This technique did not allow the threads to float freely in the subcutaneous tissue. 35 Patients were given topical and oral antibiotics for 5 days. Although reported outcomes were good to excellent in all patients, infection developed in two patients and a granuloma appeared in two other patients, all within 1 month after the procedure. The infections were treated with additional ciprofloxacin. For granulomas, intralesional triamcinolone acetonide 10 mg/mL was injected.
Ahn and colleagues 33 reported a case of cellulitis in a woman presenting with a 3-month history of persistent, multiple inflamed palpable masses in both cheeks. The patient had undergone three courses of acupoint embedding therapy with use of PDO threads during the last 2 years. After combination antibiotic therapy failed to reduce the inflammation, excisional biopsy revealed the presence of threads which were removed. Tenderness and swelling in both cheeks resolved in 2 weeks.
In their 160-patient study, Bertossi and colleagues 11 treated deep nasolabial folds with or without midface ptosis and jowls in patients whose soft tissue thickness was sufficient to conceal the inserted threads. Reported complications included superficial displacement of the barbed threads into the dermis, erythema, skin dimpling, infection, and temporary facial stiffness for an overall complication rate of 34%. Superficial displacement of barbed threads into the dermis occurred 1 month postoperatively and required suture removal. The patient was instructed to massage the treated area three times daily for 6 days before the threads were surgically extracted in a direction opposite that of placement. The authors suggested that this complication may have been due to their insertion technique. Erythema resolved without treatment and was absent 1 month postoperatively. Patients resolved skin dimpling by lightly massaging the treated area daily for several days or weeks. Infection required removal of the sutures by the same procedure used to remove displaced sutures. Facial stiffness resolved spontaneously in both patients within 7 to 15 weeks.
Kang and coworkers 19 reported the use of wedge-shaped PDO threads for the treatment of deep static glabellar and forehead wrinkles in 33 Korean patients. Three patients (9.1%) experienced procedure-induced complications resulting from too superficial insertion of the PDO threads. Two patients experienced skin ulcerations and thread extrusion was noted in another patient, both complications attributed to excessively superficial insertion of the PDO threads. Complications were resolved in all cases by removing the thread.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


