Summary
The concept of SMAS facelift involves a spectrum of SMAS manipulation ranging from imbrication or plication to undermining in a deep plane. We define a “SMAS facelift” as a facelift where the SMAS is advanced without extensive undermining of the SMAS (deep plane), followed by resuspension via plication or imbrication. This procedure is ideal for patients who have mild or moderate sagging of facial skin and soft tissue or for patients who may be predisposed to poor wound healing that necessitate a more limited dissection. This chapter covers the procedure in detail, as well as how to optimize outcomes and minimize complications.
17 SMAS Lift
17.1 Introduction
The facelift procedure has undergone several modifications over the past century since first explained by Hollander in 1901. 1 The various techniques differ in length and placement of the incision, the extent of undermining and dissection, and the handling of the superficial musculoaponeurotic system (SMAS). Methods include simple skin dissection, SMAS plication or imbrication, deep plane, composite, high-SMAS, extended SMAS, subperiosteal, SMASectomy, and other variations. 2 , 3 , 4 , 5 , 6 , 7 , 8 , 9
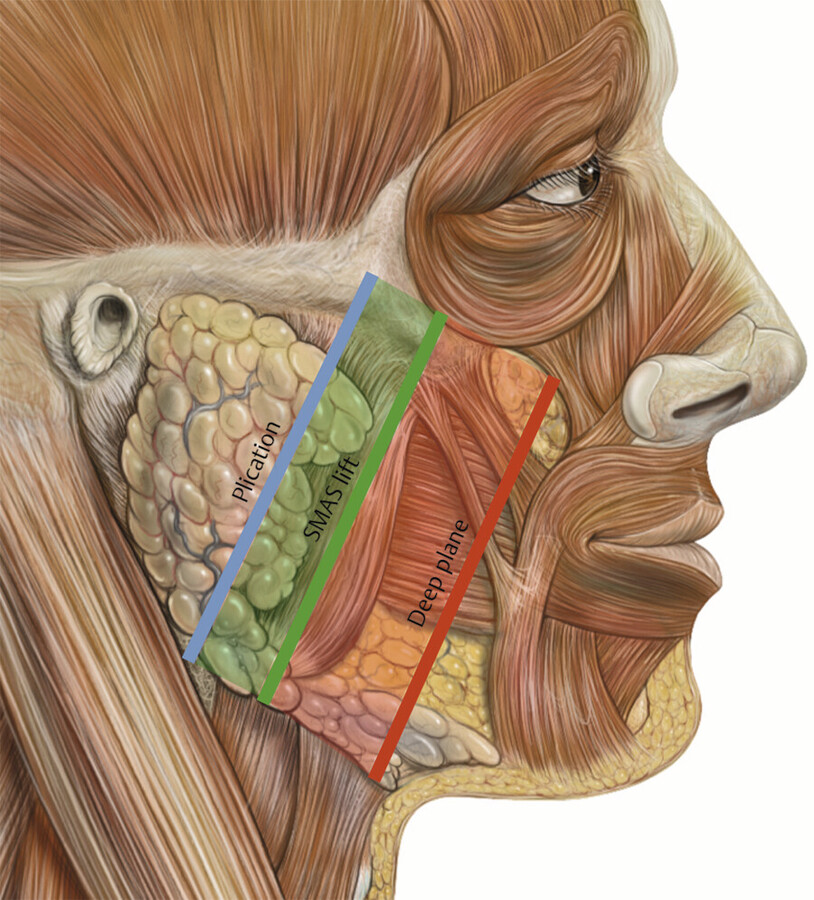
For the purposes of this chapter, it is important to define a “SMAS facelift.” Technically a SMAS facelift involves a spectrum of SMAS manipulation that ranges from imbrication or plication to a deep plane dissection (Fig. 17.1). We define a “SMAS facelift” as a procedure without any significant undermining (> 3 cm) of the SMAS followed by resuspension of the SMAS via plication or imbrication.
17.2 Indications and Patient Selection
Although there are many variations of the facelift procedure, the goals remain the same. These include removing excess fat and repositioning tissue to achieve a more youthful, yet natural lift. The author’s technique involves the removal of any excess cervical fat, repositioning the SMAS and platysma, and removing excess cervical and facial skin. Ideal candidates are those in good health with good vascularity who exhibit a loss of skin elasticity, sagging of cheek tissues and cervical platysma, and who may also have excess neck fat. Patients who enjoy average weight, an aesthetic facial bony contour, and high posteriorly positioned hyoid bone are usually better candidates than those who have thin tissues, are overweight, or who have a low-anteriorly placed hyoid.
Patients should be psychologically stable, possess realistic expectations, and demonstrate comprehension of the limitations of the facelift procedure. In the author’s practice, the details are usually discussed on three occasions prior to surgery: initial consultation, preoperative instructional visit 2 to 3 weeks prior, and the day of surgery. Patients must also understand that no surgical rejuvenation procedure can remove facial asymmetries, improve the general facial deflation that occurs with aging, halt aging, remove wrinkles, or facial expression lines, or restore the deteriorated condition of skin. Other techniques, not included with the facelift procedure, might be considered or needed to address facial atrophy, wrinkles, skin deterioration, asymmetries, and/or future aging.
In the author’s practice, the average facelift candidate typically undergoes a deep plane facelift. Our SMAS facelift is selected for those patients needing minimal tissue repositioning or those with a potentially compromised vascular supply. Certainly, patients with minimal-to-moderate tissue sagging do not need extensive skin undermining or extensive sub-SMAS undermining. Patients with a history of excessive smoking or medical conditions such as lupus, rheumatoid arthritis, or scleroderma are not generally good candidates for facelift procedures due to a compromised vascular supply. However, in select patients with a remote past history of smoking (minimal current social smoking of 3–4 cigarettes/d) or those with very mild cases of collagen vascular disease may be candidates for minimal skin undermining facelift-type procedures. The SMAS facelift can be done with minimal skin undermining and excellent tissue movement via SMAS repositioning.
17.3 Surgical Technique
17.3.1 Procedure Details
We have found that intravenous sedation provides excellent and safe anesthesia with a quicker gentler emergence for facelift patients. Although general anesthesia is commonly used throughout the United States, we have found it to be unnecessary. Our sedation is carried out in a state-licensed facility that must comply with safety guidelines. All emergency equipment, proper personnel, and appropriate emergency medications are available. In our facility, the patient is administered diazepam 20 mg orally, dimenhydrinate 200 mg orally, and prednisone 40 mg orally 1 hour prior to surgery. The patient is also administered an oral antibiotic. It may take an hour or slightly longer for the diazepam to have full effect. During this time, the patient is marked for incisions and injection of local anesthetic (Fig. 17.2, Fig. 17.3).
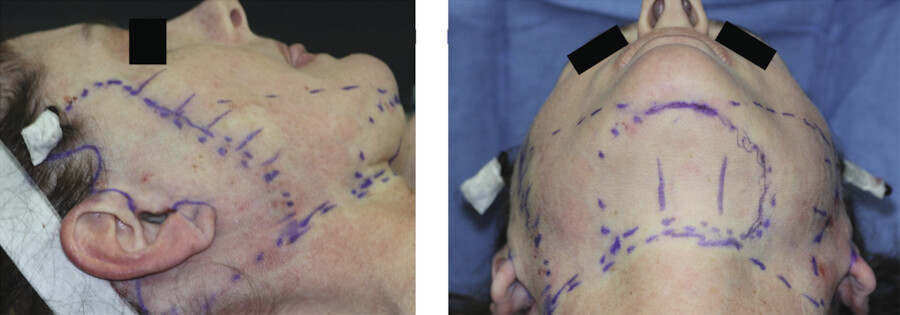
The senior author believes in preserving the temporal sideburn at the level of the superior portion of the ear. Therefore, a horizontal mark is usually placed in this location to prevent the repositioning of hair to a point superior to the cephalic portion of the ear. The resulting incision may then be reused in future facial rejuvenation procedures without the elevation of the sideburn area and loss of temporal hair. Instead of shaving the patient’s hair, parted segments of temporal hair on either side of the incision are twisted and wrapped with paper tape. The mark is continued in the preauricular groove found just in front of the curvature of the auricle. In female patients, a posttragal mark (1–2 mm behind the tragus) is incorporated to hide the scar. In male patients, the incisional mark is usually carried in front of the tragus in a preauricular crease. The author usually leaves an area of non-hair-bearing skin between the tragus and sideburn in male patients. The mark then curves around the earlobe. Postauricularly, the incisional mark is carried slightly up on the posterior surface of the ear parallel to the postauricular sulcus. Some surgeons stop the incision low in the postauricular sulcus. However, the resulting bunching (even if only temporary) can be somewhat disconcerting to patients in the early postoperative period. The continuation of the postauricular incision along the posterior hairline allows for removal of excess skin and the lessening of bunching. The extent of skin undermining is marked approximately 5 cm from the incision site, circumferentially around the ear.
Local anesthesia is carried out with 1% xylocaine and 0.25% bupivacaine with 1:150,000 epinephrine along the incision lines and the borders of the areas to be undermined. A tumescent mixture of 0.3% xylocaine with 1:600,000 epinephrine is injected in the areas to be undermined. Intravenous sedation can be very helpful during the injection of local anesthesia. It is usually delayed until the oral diazepam has been fully absorbed. Intravenous sedation by the anesthetist or anesthesiologist usually makes the patient totally unaware of the application of local anesthetic.
After local anesthesia has been administered, about 10 minutes are allowed to pass in order to allow the epinephrine to take full effect for hemostasis. The skin should be noticeably blanched, which allows you to determine if additional local anesthetic is needed in certain areas. However, patients with thick skin may not have as much noticeable blanching.
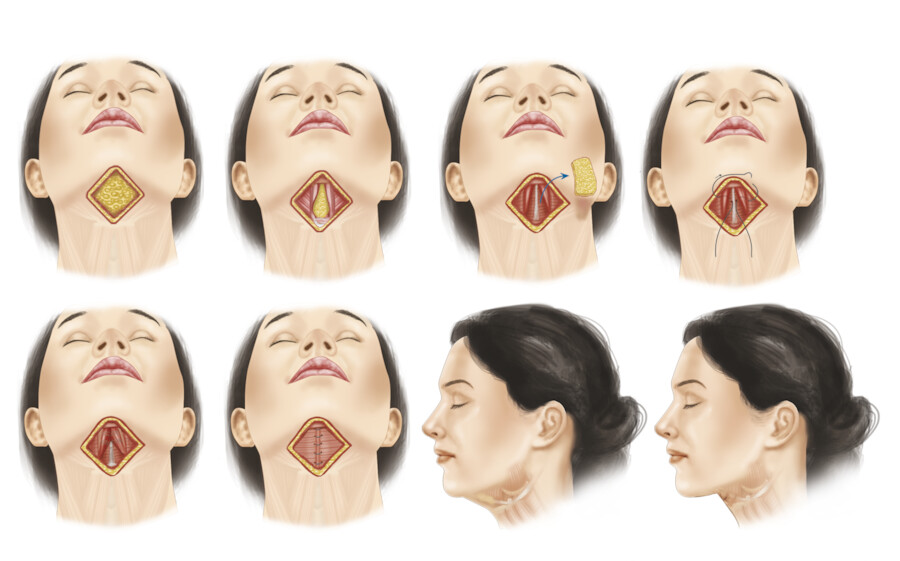
The submental area is addressed first with cervicofacial liposuction and platysmaplasty as indicated. 10 , 11 Patients with a significantly obtuse cervicomental angle may benefit from a SMMS (submental muscular medialization and suspension) procedure for more dramatic results. SMMS is performed by excising the fat overlying the mylohyoid fascia, then suturing the anterior digastric muscles to the mylohyoid fascia in the midline to prevent a cobra deformity. The platysma muscle is then sutured to the digastric muscles in the midline (Fig. 17.4). 12 , 13 , 14
Attention is then turned to performing the SMAS facelift. A #15 blade is used to make the incisions in the preoperative periauricular markings. The incision is carried through the dermis and is beveled across the direction of the hair follicles in the hair-bearing horizontal temporal incision and the posterior hairline skin. This maneuver allows the hair to grow through the incision line.
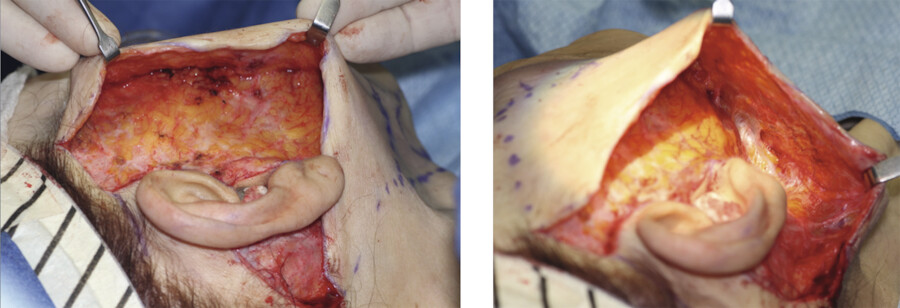
The skin is then undermined using facelift scissors beginning at the tragus, leaving as much subdermal tissue as possible attached to the deep tissue (Fig. 17.5). A thin tragal flap minimizes tragal contracture during the postoperative healing phase. The remainder of the facial skin is then fully undermined in a supraSMAS (subdermal) layer to a point averaging 5 cm from the incision, following the preoperative marking plan (Fig. 17.6). Care is taken to avoid damaging the subdermal vascular plexus. Countertraction is provided by the assistant. Hemostasis is achieved with bipolar cautery under direct visualization. The extent of skin undermining is generally limited to around 4 to 5 cm. This preserves the vascular supply in most patients.

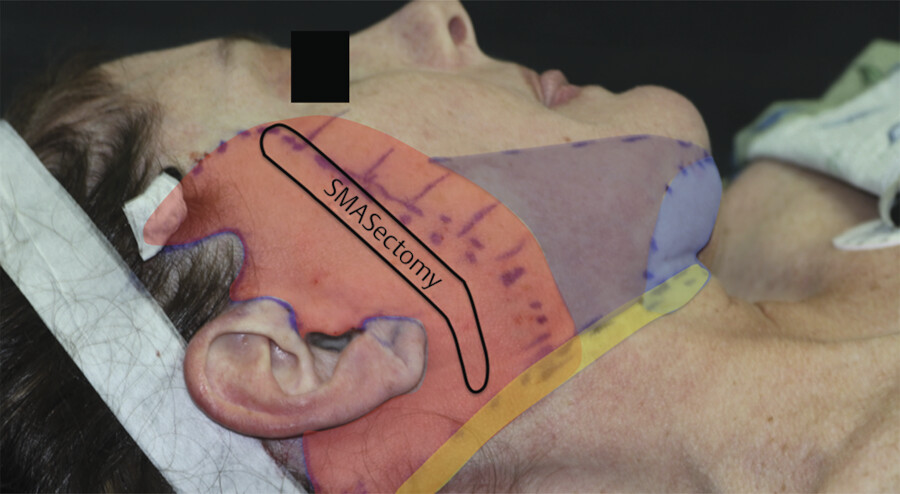
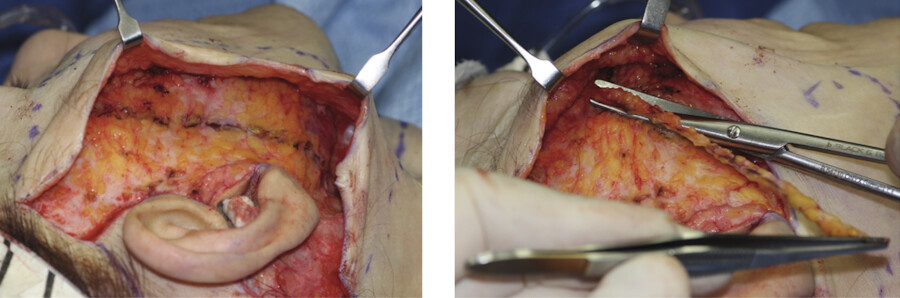
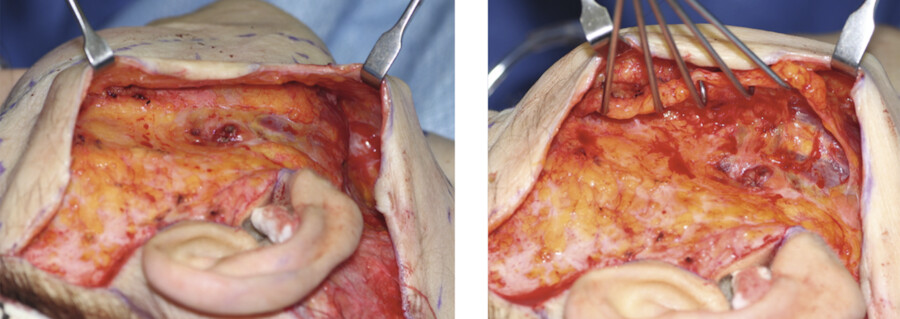
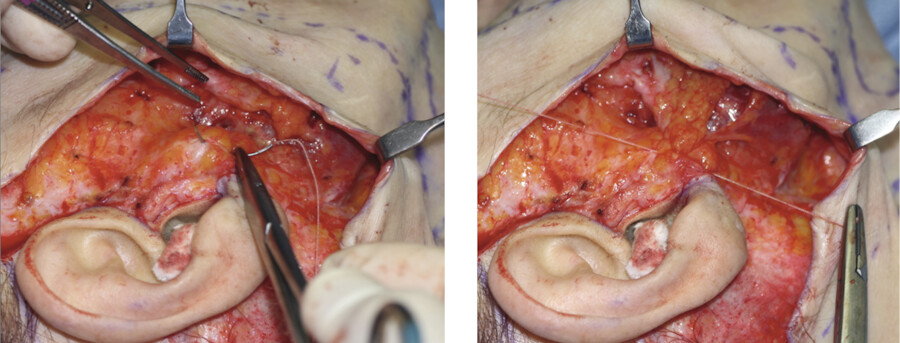
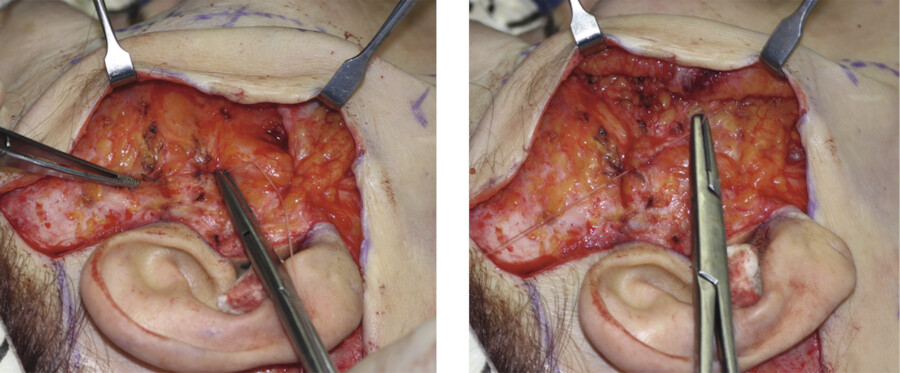
With the skin flap adequately elevated, SMA Sectomy is performed (Fig. 17.7). A 1-cm-wide strip of SMAS is excised in from the preauricular area down to infraauricular fascia. The SMAS can then be grasped and pulled ensuring adequate mobility and repositioning of the tissues. Undermining of the SMAS about 2 cm will allow further mobilization and repositioning of the SMAS for optimal results (Fig. 17.8). Anchoring sutures of 2–0 Mersilene are used to anchor the SMAS in two positions. The first suture is placed in the strong preauricular fascia directly at the tragal–lobule juncture (Fig. 17.9). The second is placed through the posterior periosteum of the zygomatic arch (Fig. 17.10). Then sutures of either 2–0 polydioxanone (PDS) or 2–0 Vicryl are placed in the region superior to the arch suture and between the two Mersilene sutures. The placement of these sutures may be continued inferiorly into the mastoid region if cervical SMAS movement is possible. The SMAS suspension will elevate the jowl, neck, and nasolabial fold. The extent of nasolabial fold and mid-cheek improvement is dependent upon the extent of SMAS undermining.
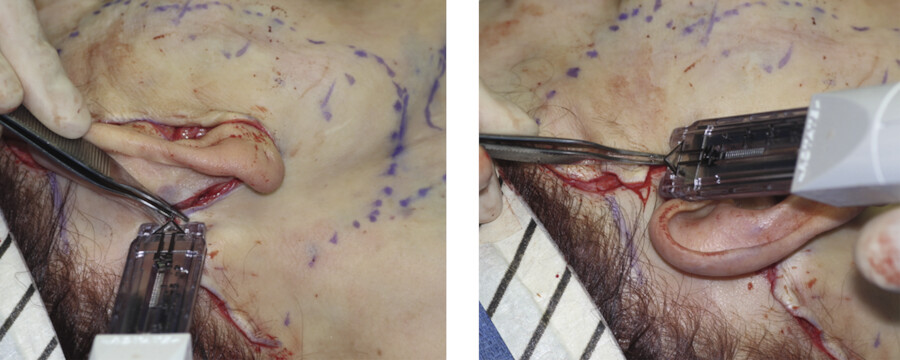
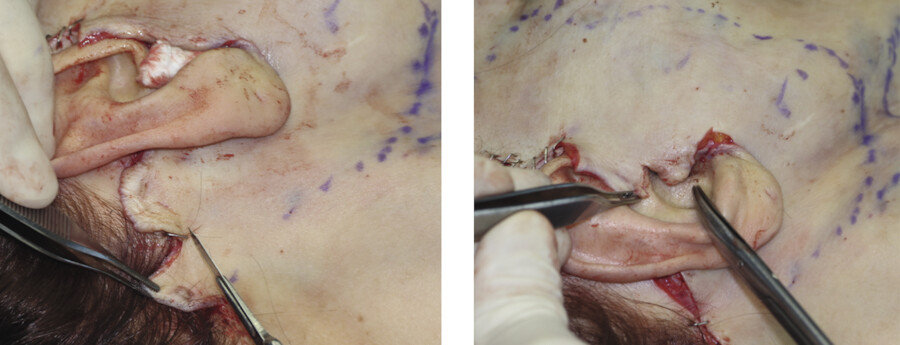
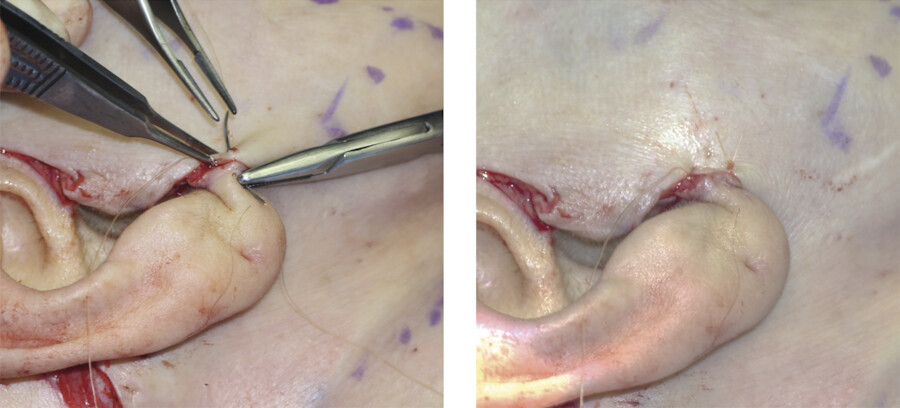
The skin is draped in a posterior–superior vector and secured at the highest postauricular point with an interrupted 2–0 nylon or surgical staple (Fig. 17.11). This is followed by a second securing suture or staple at the junction of the horizontal temporal incision and the superior extent of the preauricular incision. The redundant skin is then resected in a manner creating minimal skin tension (Fig. 17.12). If any dimpling or bunching of skin is noted, further undermining can be performed. The neotragal skin is left redundant to avoid forward displacement of the tragus by skin contracture. The earlobe is placed in a position that is about ½ to ¾ cm superior to the position where it naturally lies in the unrepaired state (Fig. 17.13). This overcorrection helps prevent the lobe from stretching too far inferiorly during the natural healing process, thus preventing the pixie earlobe deformity. The skin along the postauricular occipital hair is reapproximated with the surgical staples. The skin edges in the non-hair-bearing postauricular areas are approximated with 5–0 plain gut suture in a running interlocking fashion, using 5–0 Monocryl for additional deep support as necessary. The postauricular closure, above the posterior portion of the earlobe and below the level of the hairline, is performed in a manner that leaves 1 cm gaps between sutures, thus aiding any fluid drainage. A size 7 round JP drain is placed posterior to the incision on the right within the hair-bearing scalp and tunneled under the neck to the left. The preauricular and tragal skin is closed using 5–0 plain gut in a running interlocking fashion. The hair-bearing temporal scalp incision is closed with staples. The submental incision may be closed with 5–0 plain gut suture in a running interlocking fashion.
Any collected blood is expressed from under the flaps via the postauricular closure gaps. A dressing is then applied with 4 × 4 gauze pads and a Kerlix gauze wrap that applies only very gentle pressure over the preauricular area, lower face, and neck. Lastly, a light elastic wrap is placed over the dressing using Coban self-adherent wrap. The elastic wrap is removed 4 hours after placement.
The patient is evaluated prior to discharge and again the following day. The remaining dressing is removed and the incisions are cleaned with hydrogen peroxide and dressed with Vaseline®. The JP drain is removed if output is less than 30 mL. The patient is instructed to keep the head of the bed elevated 30 degrees, avoid strenuous activities, not bend over, and not turn his or her head (Fig. 17.14).

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


