Summary
In this chapter we present how to safely perform hair transplantation and how to prevent complications, as well as how to treat the most frequent complications. There are two main techniques for donor hair harvesting: (1) Follicular unit transplantation (FUT) which refers to horizontal donor ellipse harvesting, subsequently carefully separating the individual follicular units and then transplanting them. (2) Follicular unit extraction (FUE) in which each individual follicular unit is harvested one by one using a 0.8 to 1.0 mm punch by manual, motorized, or robotic means. Then the actual transplantation is done in the same fashion with either method, one by one. Our personal preference is FUT, that is, the horizontal donor ellipse (Strip). We have described step by step how we do this safely. Unfavorable results are generally due to poor planning and execution of the procedure. The most frequent are: too low or too straight design for the front hairline, grafts that are too large giving a plug-like appearance, scarring alopecia due to tight closure of the donor ellipse or overharvesting with FUE, and poor hair growth. All of them can be avoided by proper planning and technique. We have given our recommendations of how to consistently obtain natural looking results, avoid complications, and how to treat them.
18 Hair Transplantation
18.1 Introduction
Hair is an important component of facial aesthetics in both males and females. The hairline helps adorn and frame the face as well as assist in establishing facial proportions. Having good hair density provides youthful appearance, and the lack of it makes us look older. We will describe here our preferred technique in hair transplantation and how to prevent and treat most complications.
We must give credit to Norman Orentreich 1 as we learned so much from him. In the late 1950s he introduced and popularized the punch grafts (hair plugs) and described what we know as the donor “dominance concept” which is key for hair transplantation: The genetics of hair is at the roots of each individual hair follicle, the hair roots harvested from the donor area (occipital and temporal areas) and transplanted to the areas of baldness will continue to grow hair for as long as it was going to do so in the donor area. This is key and very important as hair in the donor areas is the most durable hair we have.
Male pattern baldness and female pattern alopecia is an inherited trait and therefore generally caused by the genes of each individual person. This makes the hair roots sensitive to dehydrotestosterone (DHT), resulting in hair loss when this hormone is present. In males, it typically starts in adolescence and progresses as we age. In females, it varies, tends to be more gradual and starts usually in the third or fourth decades of life.
Most men who lose their hair, do so primarily on the top of the head and not on the temporal and occipital areas. In women, it tends to be more generalized with less loss in the lower occipital and temporal areas. To date we have no method for creating new hair; all current techniques for hair restoration involve redistributing the patient’s existing hair. Therefore, candidates for hair transplantation are limited to those who have a favorable ratio of donor hair density relative to the size of the area to be transplanted. Several centers worldwide are working on tissue engineering in an attempt to clone hair follicles or culture and multiply hair follicles in the laboratory setting. When this is successful, we will be able to treat patients with limited donor hair and will need only harvest a sample of their hair follicles.
Male pattern baldness is a progressive condition. The rate of hair loss may slow down after an individual is about 40 to 50 years of age, but it never stops completely. Thus, the preoperative plan must ensure a natural-looking result both short and long term.
As with any other elective procedure, make sure the patient is low risk when scheduling. If any doubts about their health, get clearance from their primary care physician. Make sure he or she is not taking anticoagulants, and if they are, make sure it is safe to discontinue them. The treatment of any medical problems should be optimized prior to any elective hair procedure. For example: If they have hypertension, it should be under control; if diabetic, make sure it is well controlled, etc.
18.2 Current Hair Transplantation Technique
First we should mention that there are two main techniques for donor hair harvesting:
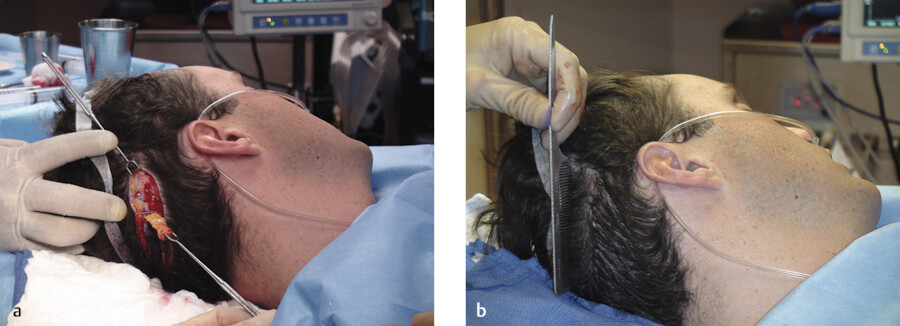
Donor strip: This is often referred to in the hair transplantation literature as follicular unit transplantation (FUT). A horizontal donor ellipse is taken from the occipital scalp and often part of the temporal areas. The resulting donor site is then closed primarily. Out of the harvested ellipse, careful dissection under magnification is done to separate the individual hair follicles to subsequently transplant them individually.
Follicular unit extraction (FUE) requires that a large area or the entire scalp is shaved and with a 0.8 to 1.0 mm in diameter punch, the follicular units are harvested one by one. This can be done manually, using motorized equipment, or with robotics. Subsequently, the follicular units are transplanted.
Here we will share with you our personal technique based on over 30 years of experience in which donor strip harvesting (FUT) was almost invariably used. We will also show how to minimize these complications and how to correct them. 2 , 3 , 4 , 5 , 6 , 7 , 8 , 9 , 10 , 11
In addition, we will share with you our thoughts on FUE and how to prevent complications when doing the FUE technique.
When performing hair transplantation, we must think and plan long term. Even on young patients, we should plan on a mature hairline design, with some degree of frontotemporal recession. There is no magic measurement as to the distance from the eyebrows to the hairline, which varies depending on the craniofacial proportions. Sometimes 5 to 6 cm is fine, other times 8 to 10 cm. The main objective is to mimic a natural, mature hairline.
The hairline should also be slightly irregular without rows or lines, we want a no line hairline. In addition, only single hair grafts should be used at the hairline.
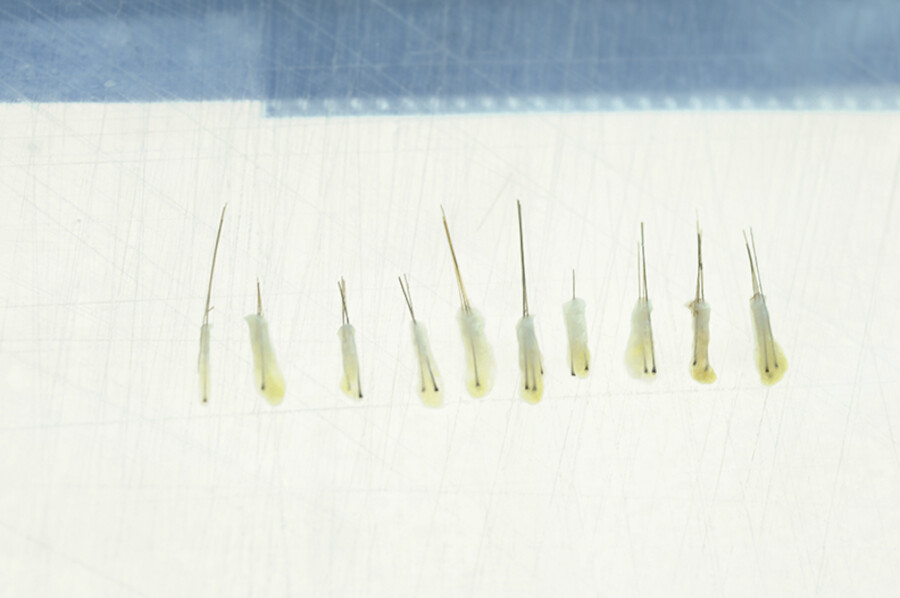
By doing the donor strip technique under 3.5-loupe magnification, incising parallel to the hair follicles and closing primarily without tension, we are able to have almost invariable, minimally detectable scarring. Once we harvest the donor strip, by using background lighting and magnification we can see each hair root well from top to bottom and thus we are able to keep at least 95% intact as we dissect them, this way increasing the viability and growth of the hair grafts. Some patients have limited donor hair, so we don’t want any to go waste.
We prefer having the patient in the supine position, under IV sedation with midazolam (Versed, Dormicum), fentanyl (Sublimaze), and occipital and supraorbital nerve blocks with 0.5% bupivacaine (Marcaine) with epinephrine 1:200,000. Other surgeons use a combination of local anesthesia and mild oral sedation rather than IV sedation. If the patient is a small child, of course general anesthesia may be better. We generally do these cases in our AAAASF facility (Video 18.1).
Once the area is locally well anesthetized, we use tumescence infiltration along the donor ellipse. This provides hemostasis and we also feel it assists in the graft dissection.
Our tumescence solution consists of 120 mL of normal saline with 20 mL of 2% plain Xylocaine plus 1 mL of epinephrine 1:1,000 plus 40 mg of triamcinolone (Kenalog). The same solution is used to infiltrate both the donor and the recipient area. By adding Kenalog we have found significantly less postoperative pain, and significantly less postoperative edema.
The occipital/temporal area is generally where the hair is the thickest and the most permanent (Fig. 18.1, Fig. 18.2, Fig. 18.3, Fig. 18.4, Fig. 18.5, Fig. 18.6, Fig. 18.7, Fig. 18.8).





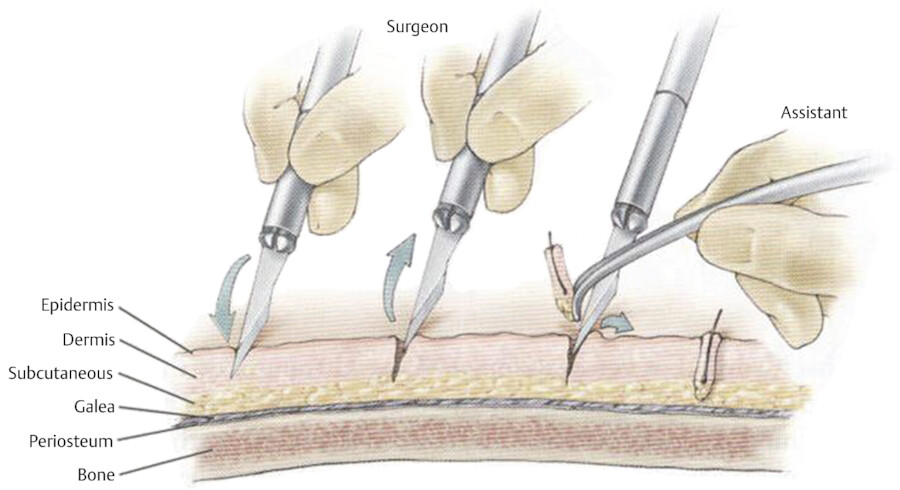
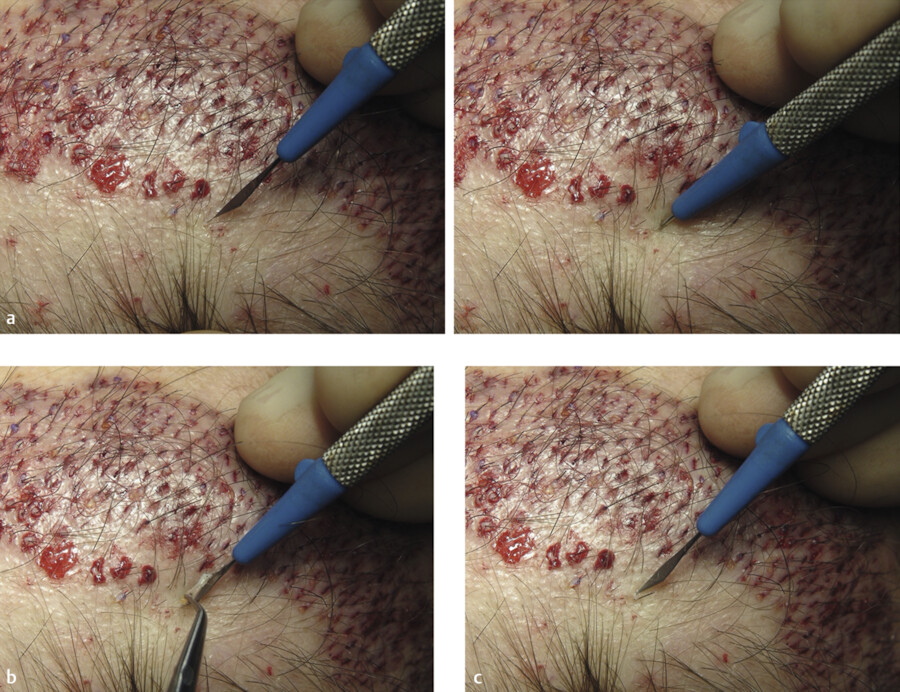
It is best to place the grafts at about 5 mm from each other initially, beginning at the front hairline and proceeding posteriorly.
As fibrinogen turns into fibrin (15–20 min later), the grafts become more secure in place. Then we go back anteriorly between the previously inserted grafts, getting them about 2.5 mm apart. If you try to pack them densely too soon, they often “Pop Out” which is very frustrating and time consuming as you would have to reinsert them.
Again, as fibrinogen turns into fibrin we go back time and time again to place more grafts in between, getting them closer and closer to each other until we are about 1 to 1.5 mm between grafts (Fig. 18.9, Fig. 18.10, Fig. 18.11, Fig. 18.12).



The donor site sutures (3–0 Prolene) are removed in the 10th postoperative day.
The hair begins to grow at 3 to 4 months and looks good at 6 months. It takes 12 months for the ultimate result.
Here is an example of the results that we can predictably obtain with today’s technology.
The hair transplantation procedure works every time. By handling the grafts gently and atraumatically, up to 90% of the grafts should grow good healthy hair. In addition, the number of hair grafts done will impact the result. In patients who want as much density as possible, assuming they have plenty of donor hair we can do the procedure several times. We prefer to wait a year between sessions, so we can see what we accomplished the first time, and let the scalp recover completely. A year later or any time thereafter we can go over the area again grafting in between the previous grafts, further increasing the hair density (Fig. 18.13a–k).

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


