Summary
Minimally invasive procedures on the face, although safe in general, are subject to complications and side effects. Some of these outcomes are unavoidable and are not related to operator error. However, a good understanding of local anatomy, within the context of where wounds are created with various interventions, can diminish the likelihood of short and long-term complications.
9 Laser Resurfacing
9.1 Introduction
Over the last 30 years many energy devices have been introduced into cosmetic medicine. One critical feature is the placement of that energy within the context of local anatomy. As one is applying the energy source, the operator should visualize where the energy is going and the immediate effect on local tissue. In energy–tissue interactions, temperature elevation is fast; however, cooling is slow, such that stacking pulses in the same area will result in a rapid local temperature increase with potentially catastrophic consequences. On the other hand, in applying a short-pulsed yellow light laser to a red area of the skin with a single pulse, only the red local targets will become hot, such that the likelihood of gross overtreatment becomes smaller. 1 , 2 Indeed, most good outcomes in skin are determined by finessing the cooling and heating of specific targets. The skin, especially facial skin, can withstand a thermal burden to a certain point, after which a threshold is breached and catastrophic consequences are sometimes observed.
Today not only does the practitioner needto be a savvy laser-and-light doctor, but also one needs to be aware of the nuances of radio frequency (RF) and ultrasound energy. To remain safe, the treating MD must remain vigilant in real-time assessment of the skin for superficial targets. For deeper targets, the operator must accurately predict where and when the heating will occur. In following sections, key points for energy–tissue interactions are provided to increase safety and minimize complications in facial skin.
9.2 Key Points for Maximizing Safety with Lasers and Other Energy Devices
Skin thickness varies across the face. The three components of the cutis are the epidermis, dermis, and fat. Epidermal thickness is fairly constant with exception of eyelid skin, where all three components are much thinner than their noneyelid counterparts. 3
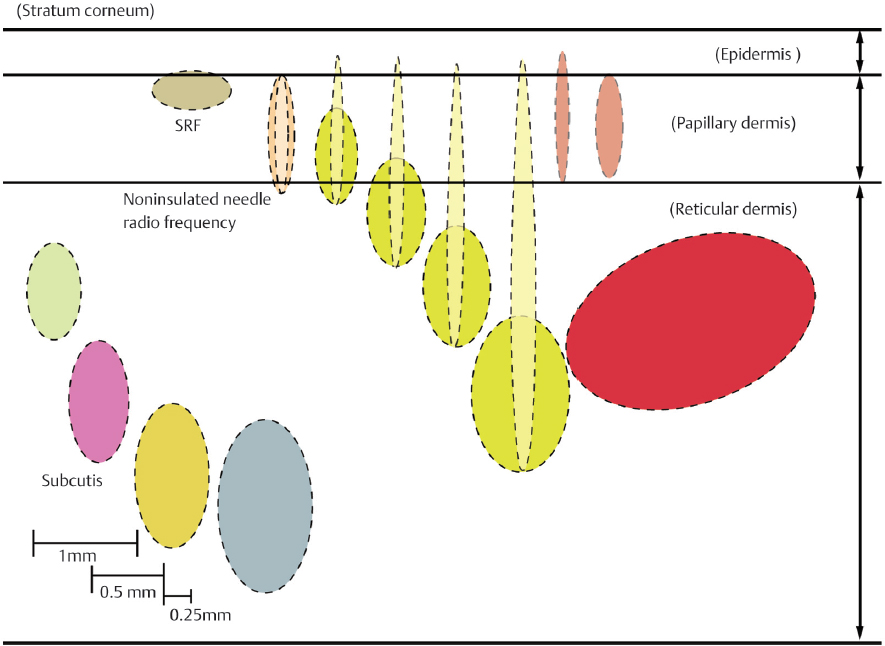
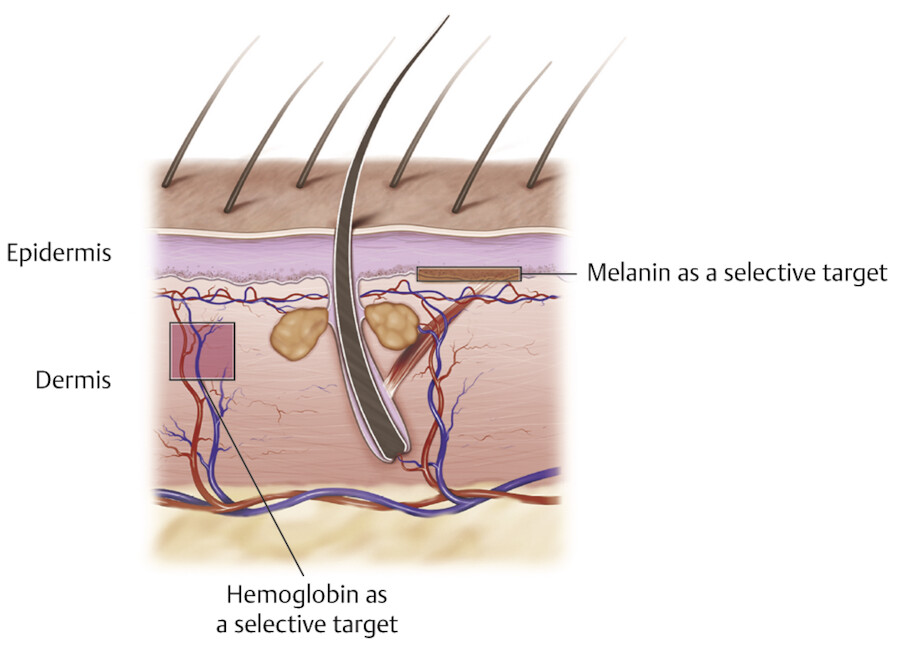
Most devices should be studied relative to where they heat (see Fig. 9.1). We can divide devices by relative depths of heating and whether they are selective or non-selective (selectivity being defined as the device preferentially targeting a small structure based on “contrast agents” such as melanin or hemoglobin) 1 , 4 (Fig. 9.2).
Most fractional devices and other surface-heating systems are not selective; rather their targeting is based on the spatial geometry of the micro beam with respect to the general skin volume. The selectivity is based also on how long the skin is exposed to the beam, and whether a broad beam (> 1 mm) or one that is fractionated is applied. 5
9.3 Key Points for Maximizing Safety with Shallower-Penetrating Lasers and Energy Devices
Visualize the wound being created.
Pay attention to the skin surface.
Use magnification if necessary to improve feedback.
Avoid bulk heating in this area.
Apply surface cooling if indicated.
9.4 Fractional Laser Systems
Most fractional lasers will only penetrate up to about 1 mm even with multiple passes such that any nerve or catastrophic vascular injury is unlikely. The main danger is in overheating of the thin skin of the lower face and preauricular regions, where lower densities and depths should be applied.
One nuance of fractional lasers is that treatment is by recipe rather than endpoints. Gross blistering or extreme immediate tissue shrinkage should alert the operator regarding potential overtreatment; however, a key point is monitoring the system display with respect to the actual placement of scans and the number of micro beams/cm2. These observations should be made within the context of surface cooling and the size of the region that is treated. Generally speaking, applying passes over large areas will result in greater tissue cooling between passes, as there is more time between consecutive passes. For example, in providing treatment for localized scarring on the cheek, where there is only a small plaque of acne scarring, if one applies four to five passes relatively quickly, there is no opportunity for the skin to cool and overheating and blistering is possible (Fig. 9.3, face blister). In general, with increasing depth and density, side effects are more likely. Also, based on surface-to-volume arguments, smaller fractional beams will cool faster than wider beams.

9.4.1 Nonablative Fractional Laser Systems
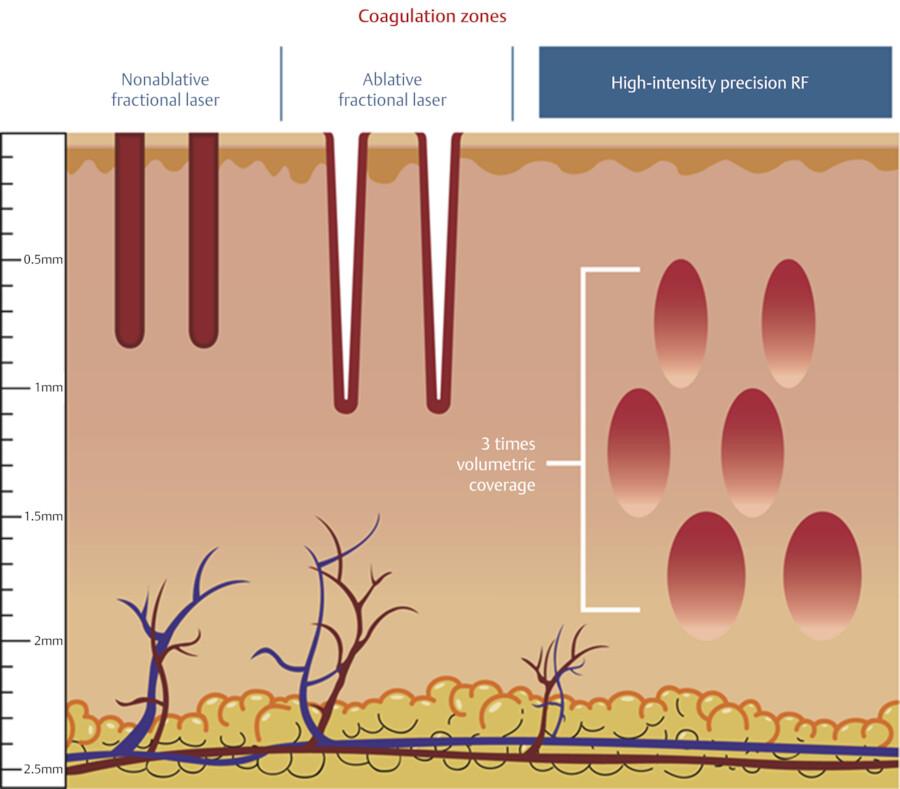
Nonablative fractional laser systems incorporate wavelengths that are poorly absorbed by water when compared to CO2 and erbium yttrium aluminum garnet (YAG) lasers. 5 Like their ablative counterparts, the main danger is laying down the scans or pulses too close together, or not allowing for cooling between scans or between stamping motions. There are also “hybrid” lasers that include both highly absorbed and weakly absorbing wavelengths. Examples include 1,550 and 1,927 nm, and 1,470 and 2,940 nm, respectfully. In areas of preexisting melasma, any superficial heating ablative or nonablative technology, whether fractional or nonfractional, can exacerbate the condition. 6
When using fractional lasers, the operator must know the nuances of the device to maintain safety. Most of these devices incorporate three settings: mJ/microbeam (which determines the microwound depth), pitch (space between the adjacent wounds which determines the density), and pulse interval between adjacent scans. The novice should employ all three parameters on the lower side and increase the settings as conditions allow. Many lasers include a percent coverage (cross-sectional coverage) as one of the parameters. These values should be interpreted cautiously, as manufacturers’ formulas vary for the determination. For example, one fractional CO2 laser is applied on the face with values as high as 70 mJ and 50% density on the graphical user interface (GUI), whereas another laser might show the same clinical endpoint with settings (on the GUI) as low as 30 mJ and 20% density. Scarring can result if the provider is not attuned to the nuances of a particular system (Fig. 9.4).

9.4.2 Microneedling and RF Pins/Needles
A number of pin and needling systems have been applied in skin facial rejuvenation. For microneedling alone (whether using a rolling device or a sewing machine-type motorized one), most devices are well tolerated, and the procedure, with or without platelet-rich plasma (PRP), tend to be free of side effects. 7 The most serious complications are associated with infusion of nonsterile topical products into the dermis. 8 Some providers apply topical products and then use the needling systems, intending to introduce these agents in the viable skin; however, for products not designed for dermal use, risks of infection and granulomatous reactions are increased. 9 A good rule is to only infuse those compounds intended for dermal use. Track marks have also been reported with microneedling devices. 10
RF fractional injuries are created by either deeper “needle” wounds (600–3,500 µm) or more superficial “pin” wounds (50–500 µm)(Fig. 9.5). There are now over 15 systems available in the United States that deploy these pins/needles into the skin. In a typical needle configuration, 25 to 49 needles are inserted over a 1 cm2 area. The needles are inserted simultaneously, reside in the skin for 50 milliseconds to 4 seconds, and depending on the setting and/or the specific device are retracted. Microwound sizes vary from very small cylinders (100 µm wide and 400 µm deep, size of “grain of sand”) to larger “grain of rice-type” geometries, depending on the pulse width, needle type, and insertion depth. 11 , 12
Concern has been expressed about fractional lasers interfering with previously placed fillers, but most filler placement has been shown to be deeper than the deepest aspects of the vertical injuries created by these devices. 13 , 14 More recently, data show that some deeper needle devices might compromise fillers, but there is only one publication 15 , 16 that suggests a clinically impactful role for deeper devices, where Weiss et al showed that deeper RF needle devices might affect superficially placed hyaluronic acid (HA) fillers. Still, on a volumetric basis, it is unlikely that the fractional device will “dissolve” fillers to a point of changing the contour of the face.
9.5 Nonfractional Ablative Treatment
Nonfractional ablative lasers now have enjoyed over 25 years of use in skin applications (Video 9.1). 17 , 18 , 19 , 20 , 21 Both erbium YAG and CO2 lasers were initially applied at total injury depths of 120 to 400 µm, depending on the application and local anatomic region. Most complications can be avoided by playing close attention to the skin surface during treatment. The CO2 laser, when applied such that total depths of injury (ablation + RTD) are less than 100 µm, is normally well tolerated, and barring infection or treating irradiated skin, the face should heal quickly, requiring less than 10 days to complete re-epithelialization. Avoidance of complications is primarily related to the depth of treatment. The areas where healing is most likely to be delayed are the lateral and lower cheeks, where the skin behaves much like neck skin (Fig. 9.6). With the CO2 laser, normally only one pass should be applied over the lateral face, lower face, and forehead, if one is to avoid hypopigmentation and texture changes, which are the most common long-term complications (Fig. 9.7). As one proceeds toward the central face, deeper heating is tolerated. Normally more than one pass of the nonfractional CO2 laser is applied only in the immediate perioral region, where the skin can tolerate a deeper injury. The role of wiping between successive passes has been explored in multiple studies, the most recent by Niamtu. 22 , 23 He found that results were similar with or without wiping, but that recovery was enhanced by not wiping between passes, presumably by allowing the denatured skin to act as a biologic dressing. Like Dr. Niamtu, we have found that perioral lines respond uniquely well to fully ablative lasers, whether CO2 and erbium YAG.

Unfortunately, performing a series of less invasive procedures (be it fractional erbium YAG or CO2 laser, non-ablative fractional resurfacing [NAFR], or microneedling) has not achieved satisfactory results, even after five to six treatments 6 to 8 weeks apart. If one examines the body of resurfacing literature over the last 25 years, data suggests that there is a threshold depth of injury for adequate wrinkle reduction in the perioral area, and that below this single treatment threshold, results are typically underwhelming, particularly for deeper perioral rhytides associated with severe solar elastosis. Outside of the deeper perioral lines, ablative fractional lasers work reasonably well (i.e., cheek lines).

For periorbital lines and forehead lines, neuromodulators are associated with a much more attractive benefit-to-risk ratio than energy-based interventions. Many patients will insist on lasers for all lines and rejuvenation, as they do not want to regularly come visit the clinic for a dose of fillers and neuromodulators. However, a frank discussion addressing the benefits and risks, and the complementary nature of devices, neuromodulators, and fillers, will often soften that stance. The mitigation of complications by lessening the risk of relying too much on any one intervention is a compelling argument to make for patients to decrease the overall facial complication rate.
Regarding the erbium YAG laser, the amount of material removed is typically directly proportional to the fluence per pass. Accordingly, one can calculate the total depth of injury by multiplying the pass number times the fluence, basing the amount of material removed by the fairly consistent value of 3 to 4 µm/J/cm2. 24 Some providers rely on bleeding as a possible endpoint for erbium YAG nonfractional applications. Our experience, however, has been that bleeding is quite variable once the beam encounters the dermis. For example, a patient with telangiectasia might have brisk bleeding, and a patient with a less red face might bleed much less at the same total depth of ablation. In some patients, particularly those prone to bleeding (i.e., on aspirin), once the dermis is encountered, bleeding can be so brisk that additional passes are compromised by the blood on the surface. Using a longer pulsed erbium YAG laser can decrease bleeding by adding a bit of coagulation. 25 Also, the application of thrombin spray after several passes can reduce bleeding and allow for additional passes.
A relatively new device on the market is a helium plasma tool (J plasma), which uses RF to excite helium gas. 26 The flow rate, RF power, and operator hand speed, all determine the amount of thermal damage to the surface. Although called a cold plasma, the reaction is thermal in nature, as energy from free electrons is transferred to the skin surface. The manufacturer claims a higher degree of safety versus CO2 lasers and other technologies, but like any thermal interaction, excessive heating has been observed (Fig. 9.8).

9.6 Key Points for Maximizing Safety in the Eye Area
The periorbital areas are particularly vulnerable to injury and one must consider the distribution of laser energy within the context of the microanatomic features of the globe and the surrounding tissue.
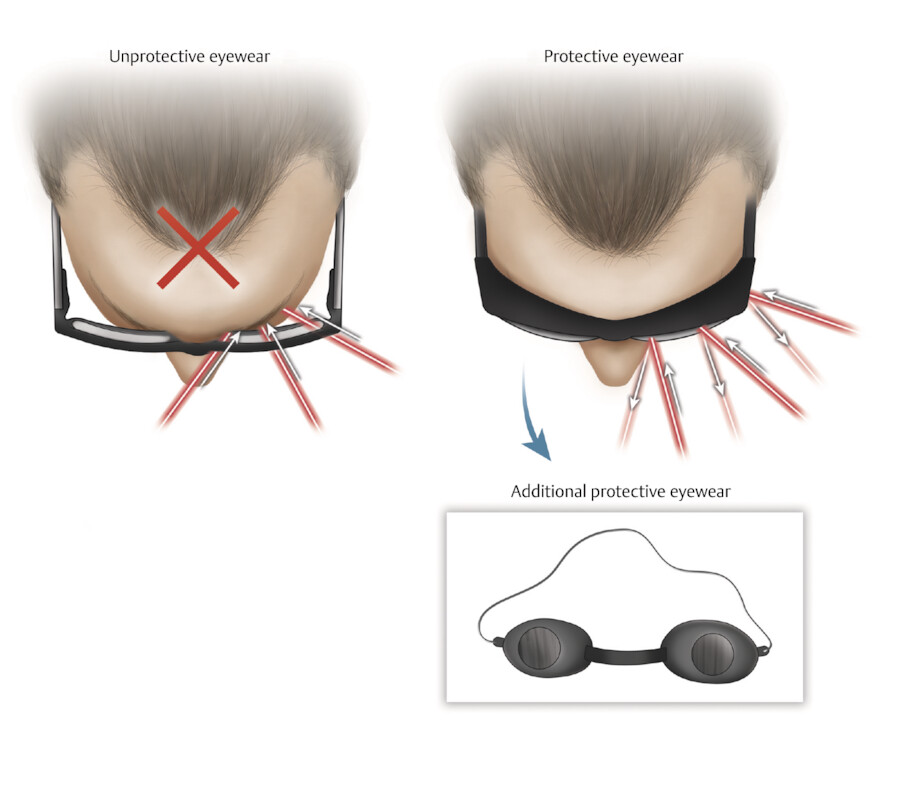
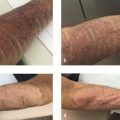
Most injuries to the eye occur when there is inadequate protection or when there is a poor understanding of the distribution of heating as a function of space and time relative to the skin surface (Fig. 9.9).
The maximum permissible exposure (MPE) is the highest power density or energy density (in W/cm2 or J/cm2) of a light source that is considered safe (i.e., which has a negligible probability for creating damage). These values tend to be smallest for 1,064 nm Q-switched lasers, where the short pulse creates a more violet impact on the retina than longer pulsed lasers.
The main eye concerns relate to exposure to visible light and near-infrared (NIR) visible light technologies. These wavelengths can penetrate quite deep and are likely to damage an unprotected retina. The injuries are usually irreversible (Fig. 9.10). On the other hand, although corneal injuries can be severe, very superficial ones can resolve on their own, and deeper ones might be corrected by corneal surgery.
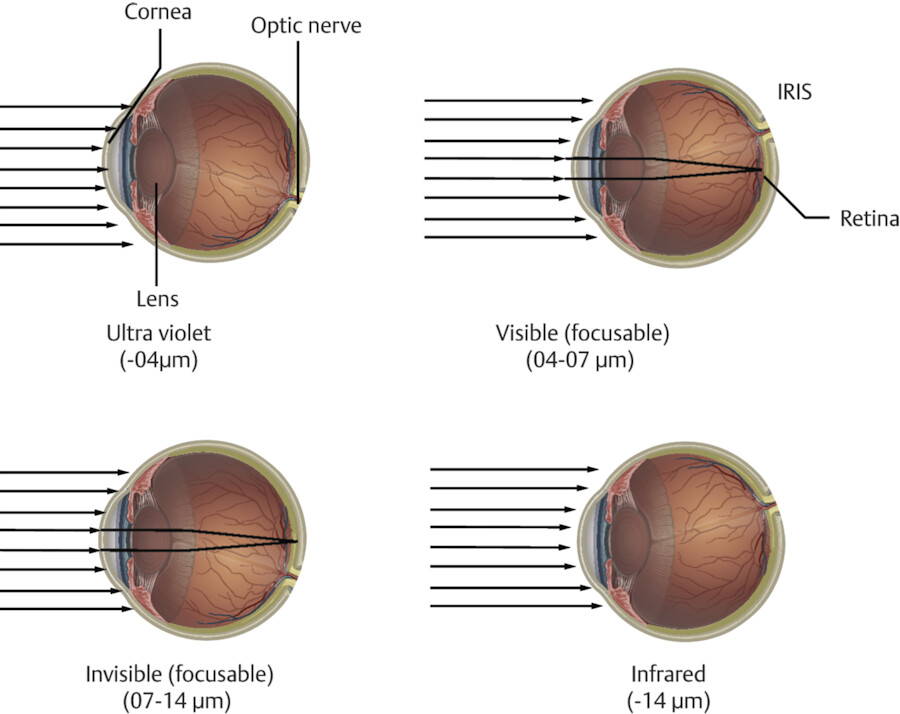
Shorter wavelengths (400–595 nm) and small spot size combinations are less likely to penetrate the thin eyelid skin. Longer wavelengths (> 755 nm) and larger spots carry a greater risk of eyelid penetration and damage to the eye’s core structures (iris, cornea, and retina). For resurfacing lasers and nonablative fractional technologies, the cornea and the lens are the eye structures most vulnerable to the beam.
A conundrum is eyeliner tattoo removal. Again, the proximity of the laser beam demands insertion of an internal shield; normally an NIR laser would be applied here, but in cases where paradoxical ink darkening is a risk, ablative lasers can be applied carefully right along the lid margin. When we use resurfacing lasers in the eye area, internal eye shields are necessary when working inside the orbit.
Also, teeth should be considered a potential target for resurfacing lasers, and there have been reports of tooth injuries with erbium YAG and CO2 lasers. 27 We normally apply wet gauze over the teeth (2 × 2 in.). A wet dental roll is an alternative.
Topical anesthetics that are more liquid in nature and are susceptible to migration across the eyelid should be avoided around the eye unless there are specifically eye safe. The pH of many of these compounds is high, and they have been implicated in corneal damage. 28 For eyelid resurfacing, particularly the upper eyelid, where it is more likely that a topical analgesic will “run” into the globe, injecting an anesthetic is preferred. We advise using 1-mL Luer lock syringe and 30-gauge needle, always maintaining the needle in a very superficial plane so that the globe is not inadvertently penetrated. The 1-mL syringe allows the operator to apply very gentle pressure so that precise placement of small volumes of anesthetic is possible. Buffered lidocaine minimizes pain greatly.
For most fractional and ablative lasers, hair is not an issue insofar as the immediate laser tissue interaction (LTI) or posttreatment sequelae, but for men, shaving on the day of treatment will minimize charring of surface hair; also a freshly shaven face enhances the absorption of topical anesthetics.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


