Summary
Platelet-rich plasma (PRP) and microneedling are generally well-tolerated procedures with low rates of adverse events, though a limited number of severe and potentially avoidable complications have been reported.
PRP treatments employ the direct delivery of growth factors for use in facial rejuvenation, recovery after facial surgery, and wound healing, including the treatment of alopecia and facial volumization. Adverse events are generally mild, infrequent, and include transient pain during injection and shortly thereafter, injection site erythema, swelling, bruising, pruritus, postinflammatory hyperpigmentation, and skin dryness. Rare but severe reported complications include a systemic allergic reaction and irreversible blindness following periocular PRP injection.
Microneedling, also known as percutaneous collagen induction therapy, involves repeatedly puncturing the skin with fine needles in order to induce endogenous production of collagen, and is employed for treatment of acne vulgaris, scars, photodamage, dyspigmentation, skin rejuvenation, hyperhidrosis, and androgenetic alopecia. Adverse events include erythema, pain, edema, scalp pruritus, and fine superficial bleeding, resolving within hours to days. Less common side effects reported include transient lymphadenopathy, telogen effluvium, acne flare-ups, milia, bruising, scabbing, flushing, oozing, transmission of blood-borne pathogens in the absence of universal precautions, and local and systemic hypersensitivity reactions.
Complications can often be circumvented by appropriate patient and region selection, proper technique, and strict adherence to good clinical practice and universal precautions. An in-depth understanding of these issues is essential to ensure safe use and maximize outcomes.
13 Complications of Platelet-Rich Plasma and Microneedling
13.1 Platelet-Rich Plasma—An Introduction
Platelet-based treatments, commonly referred to collectively as platelet-rich plasma (PRP), employ the direct delivery of growth factors for use in facial rejuvenation, recovery after facial surgery and wound healing. 1 Autologous PRP-based aesthetic treatments allow the surgeon to deliver a functional wound healing response to a targeted area or, in the absence of a wound, to stimulate the production of viable blood vessels, fat cells, and collagen deposits that appear to persist over time. 2 In facial plastic surgery, common indications for PRP include the treatment of alopecia and facial volumization including the treatment of superficial rhytids, depressed scars, and deep nasolabial folds. PRP has also been described for wound healing in facelifts, facial implants and lateral osteotomies. The most common growth factors concentrated in these preparations include platelet-derived growth factor, transforming growth factor-beta, vascular endothelial growth factor, epidermal growth factor, and insulin-like growth factor. 1 These growth factors are chemotactic for monocytes, fibroblasts, stem cells, endothelial cells, and osteoblasts and mitogenic for fibroblasts, smooth muscle cells, osteoblasts, endothelial cells, and keratinocytes. 1
Autologous PRP can be prepared expediently and at point-of-care by a wide range of manual or fully automated protocols which typically begin with collection of peripheral blood in a vacuum-sealed collection tube with an anticoagulant, followed by multiple centrifugation steps with or without a separator gel in order to isolate a platelet-rich fraction, which is injected using a 30-gauge needle into the dermis, subdermis, or preperiosteal plane as needed. 3
For a given PRP preparation and protocol, the surgeon should consider the fibrin density, leukocyte content, and degree of standardization of the procedure. 4 PRP, can be subcategorized as one of four types: pure PRP, leukocyte-enriched PRP, pure platelet-rich fibrin, or leukocyte-enriched platelet-rich fibrin. 4 The inclusion of leukocytes in PRP is controversial—while leukocytes produce vascular endothelial growth factor, important for the promotion of angiogenesis, they are also associated with the production of matrix metalloproteinases, which are known to have catabolic effects on extracellular matrix proteins including collagen. 4 , 5 , 6 , 7 The fibrin network may protect growth factors from proteolysis, serve as a more robust scaffolding structure for wound repair, and facilitate longer persistence and resistance to washout of platelet products at the site of injection. 2
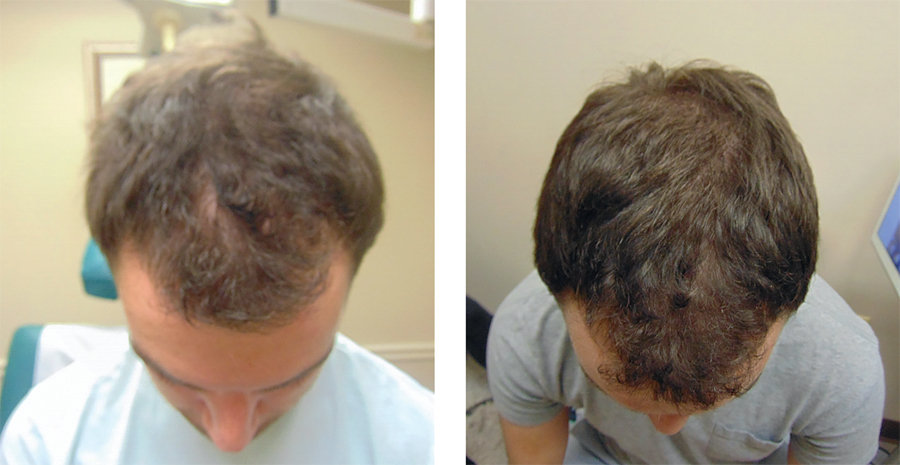
Applications of PRP include treatment of alopecia with subcutaneous or intradermal scalp injections (Fig. 13.1). 8 Acne scars or depressed scars are treated with subcision followed immediately by subdermal injection of PRP (Fig. 13.2). 3 Fine rhytids are injected intradermally. Deeper folds and volume deficient areas are injected at the dermal-subdermal border. 3 Areas requiring significant volume augmentation may be injected into deep fat (mid-face) or preperiosteally (suborbital hollows). 3 Surgical applications of PRP include augmented autologous fat transfer, in which PRP is mixed with fat (generally in a 1:2–3 ratio) just before fat injection; rhinoplasty, in which PRP is injected along the lateral osteotomy site; and rhytidectomy, in which PRP is placed in a thin layer over the flap bed before closure. 3

PRP allows for volume restoration without substantial inconvenience to the patient, and is minimally invasive with a negligible associated recovery time. Few complications related to PRP material have been described and more often can be attributed to poor patient or region selection, injection technique, or failure to follow good clinical practice and universal precautions. 9 , 10 An in-depth understanding of these issues is essential to ensure safe use and maximize outcomes.
13.2 Platelet-Rich Plasma—Avoiding, Identifying, and Managing Complications
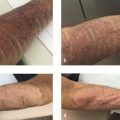
Adverse events secondary to PRP are mild, infrequent, and include transient pain during injection and shortly thereafter, injection site erythema, swelling, bruising, pruritus, postinflammatory hyperpigmentation, and skin dryness (Fig. 13.3). 11 , 12 After treatment, intermittent application of cool compresses to the injected regions for the first few hours decreases swelling, bruising, and discomfort. 13 Massaging the region for the first several hours should be avoided as this may cause washout of the PRP. 13

While granulomas and nodularity have been reported following injection of synthetic fillers, the only reports of granulomatous sequelae from PRP occurred in two patients with either known or suspected subclinical sarcoidosis, a systemic granulomatous disease that can occur at sites of cutaneous injections. 14 , 15 As such, if sarcoidosis is suspected in patients considering PRP, further diagnostic work-up is mandatory. Though unreported for aesthetic applications, PRP injection of a tibial bone cyst has been implicated in the development of a systemic allergic reaction, thought to be predicated on a reaction to the calcium citrate anticoagulant used in preparing the injectate. 16
Multiple systematic reviews on the use of PRP for androgenetic alopecia, the most studied aesthetic application of PRP, have shown no reports of bacterial, viral, or mycobacterial infections, folliculitis, panniculitis, allergic reactions, hematoma or seroma formation. 8 , 17 However, as with any invasive procedure, good clinical practice and universal precautions are imperative. Proper labeling and handling of blood samples, processing only one patient’s blood at a time and following universal precautions are all important in ensuring patient safety.
Severe adverse events are uncommon and few have been reported. While visual complications from synthetic cosmetic fillers have been reported, PRP is not often used as a physical filler but rather for the growth factors it contains. Nevertheless a single case of irreversible blindness and cerebral infarct seen on magnetic resonance imaging (MRI) following periocular PRP skin rejuvenation treatment in the glabellar region performed by an unlicensed practitioner has been reported. The authors hypothesize that the technique employed in a region close to the supraorbital and supratrochlear arteries may have caused intra-arterial injection with retrograde flow of the platelet clot and resultant occlusion of the ophthalmic artery and regions of the middle cerebral artery. In this case, the patient presented to an ophthalmologist on the day after treatment with glabellar injection site skin necrosis, restricted ocular motility, and ophthalmic artery occlusion on dilated fundus exam. MRI demonstrated extraocular muscle ischemia, optic nerve infarction, and right frontal, parietal, and occipital lobe infarction. Thromboembolic and vascular evaluations were negative. Since the patient presented outside of the window for treatment with tissue plasminogen activator, treatment was limited to ocular massage, topical brimonidine 0.2%, topical timolol 0.5%, oral steroids, and empiric IV antibiotics for possible infectious etiology of periorbital swelling. Ocular motility returned to normal, but at one year, the patient’s vision remained no light perception. At one year, residual scarring and hard nodules were present in the right glabellar region with scar tissue. 18
Familiarity with facial vascular anatomy along with maintenance of the injection plane within an intradermal rather than subdermal plane when appropriate may reduce the risk of vascular compromise. 18 Awareness, early recognition, and urgent treatment of vascular complications are essential. To minimize the risk of vascular complications, it is pragmatic to inject the smallest possible volume capable of producing the desired effect in small and discrete aliquots, aspirate prior to each injection, avoid adulteration of PRP preparation with unapproved fillers, and employ smaller needles (30–32 gauge) with prudent technique and the judicious use of pressure. 19
13.3 Microneedling—An Introduction
Microneedling, also known as percutaneous collagen induction therapy, involves repeatedly puncturing the skin with fine needles in order to induce endogenous production of collagen, and is employed for treatment of acne vulgaris, scars, photodamage, dyspigmentation, skin rejuvenation, hyperhidrosis, and androgenetic alopecia. 20 , 21 Microneedling typically employs a roller or stamp with multiple needles, typically ranging from 0.5 to 1.5 mm in length, which pierce the stratum corneum and papillary dermis, and can be combined with PRP therapy. 21 , 22 , 23 Focused mechanical injury triggers an inflammatory and wound healing cascade, resulting in the release of growth factors and collagen deposition. 20
13.4 Microneedling—Avoiding, Identifying, and Managing Complications
In general, microneedling is associated with a low rate of adverse events, with transient erythema and postinflammatory hyperpigmentation most commonly reported. 21 , 24 Microneedling can be performed as an independent procedure or together with radiofrequency in which case it is frequently referred to as microneedling radiofrequency. Radiofrequency is also discussed in chapter 12. Radiofrequency microneedling can be performed utilizing unipolar or bipolar radiofrequency. Radiofrequency microneedling can be seen in Video 13.1. Minor complications identified by several review articles include erythema, pain, edema, scalp pruritus, and fine superficial bleeding, resolving within hours to days depending on the size of needle employed. 23 , 25 Less common side effects reported include transient lymphadenopathy, telogen effluvium, acne flare-ups, milia, bruising, scabbing, flushing, and oozing. 25 , 26 Erythema can be temporary (3–5 days) and dryness often subsides over 1 to 2 weeks. 27 , 28 In one series of 210 procedures of PRP with microneedling for alopecia, 14% of patients experienced scalp pruritus (n = 30), 1.4% transient hair shedding 4 to 6 weeks postprocedure with improvement at 6 to 8 weeks (n = 3), and 1.9% transient cervical lymphadenopathy (n = 4). 26 As with any invasive procedure, a theoretical risk of infection exists though it has not been reported, and histologic examination 24 hours posttherapy reveals an intact epidermis. 21 , 23
Contraindications to microneedling include anticoagulant medications or coagulopathy that may result in excessive bleeding; active or recurrent herpes infection/herpes labial is, which may predispose to reactivation and possible scarring after minor trauma; presence of overlying skin infection, skin cancer, warts, or solar keratoses; and a history of severe keloid tendency in which each pinprick may result in a keloid (these patients can often be identified by presence of keloids on palms of hands or soles of feet). 29
Postinflammatory hyperpigmentation (PIH), a reactive hypermelanosis of the skin that occurs when cutaneous inflammatory mediators stimulate melanocytes to increase production and transfer of melanin to surrounding keratinocytes, has infrequently been described and most often spontaneously resolves in the setting of microneedling. 30 , 31 , 32 Photoprotection after microneedling is routinely recommended to minimize the risk of PIH. A single study with inadequate postprocedure photoprotection associated with PIH observed gradual improvement in PIH in a subset of patients when subsequent strict photoprotection was subsequently implemented. 33 In general, because the natural history of PIH is to improve slowly, medical therapy is not necessary in all patients and when employed its purpose is to accelerate resolution, and may include consideration of topical hydroquinone, retinoids, azelaic acid, and/or chemical peels. 34
Two case series report a “tram track” effect following microneedling with a dermaroller, referring to papular scars in a linear pattern in the distribution of the dermaroller. 30 , 33 The authors noted a 20 to 30% improvement in these scars with 0.025% topical tretino in gel after 3 months, though no long-term follow-up is described. 33 Precautionary measures to minimize the risk of this complication include using needles sized less than 2.0 mm, adjusting the degree of pressure applied to the dermaroller when such an effect is identified, and heeding caution when microneedling over bony prominences. Although not well described in the current literature it is possible to develop scarring from radiofrequency microneedling. The scarring potentially can be due to the actual needles or the effects of the radiofrequency energy.
With current technology, it is important during a microneedling procedure to align the needles so they are perpendicular to the skin surface and not at an oblique angle. If they enter the skin on an angle this could lead to development of short track marks. These marks may be shorter but similar to the marks reported using a dermaroller. 30 , 33
Local and systemic hypersensitivity reactions have been reported twice, both with the concurrent application of topical products not approved for intradermal injection with microneedling, and in a patient with known nickel-sensitive contact dermatitis who underwent microneedling with needles composed of 8% nickel bound to surgical grade stainless steel alloy. 35 , 36 In the first case series, biopsy-proven facial granulomatous reactions and a case of systemic hypersensitivity were thought to be predicated on the introduction of immunogenic particles into the dermis that potentiated persistent delayed-type hypersensitivity reactions. 35 In this series of three patients, initial treatment with topical and oral corticosteroids was ineffective while therapy with doxycycline hydrochloride and minocycline hydrochloride led to partial or complete resolution. 35 The ineffectiveness of corticosteroids coupled with successful treatment with tetracycline antibiotics suggests a possible biofilm infection of metal particles in this case. 19 In the second series, systemic antibiotics were ineffectual, patch testing revealed reaction to nickel sulfate, and hospitalization with oral and topical corticosteroid treatment led to gradual improvement over 2 weeks. 36 It is important to avoid the application of nonapproved topical agents with microneedling and to ensure that microneedle composition does not include known allergens in patients with a history of or suspected contact dermatitis.
Two patients contracted HIV infection during a “Vampire Facial” (a combination of microneedling and topical PRP) at an unlicensed New Mexico spa; appropriately sterilized equipment would have rendered this complication otherwise impossible given the autologous nature of PRP, and highlights the need for appropriate practitioner training, good clinical practice, and universal precautions. 9 , 10
In summary, PRP, microneedling, and microneedling radiofrequency are generally minimally invasive, well-tolerated, and relatively safe procedures, with negligible associated recovery times and limited adverse event profiles. The majority of reported complications can be circumvented by appropriate patient and region selection, proper technique, and strict adherence to good clinical practice and universal precautions.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


