Fractures of the zygomaticomaxillary complex and zygomatic arch are common athletic injuries. Fracture displacement can lead to midfacial retrusion and widening, causing noticeable deformity. Associated signs and symptoms include hypoesthesia of the infraorbital nerve distribution, trismus, and subjective malocclusion. Operative treatment is indicated in cases of significant displacement or functional disturbance. The approach and details of osteosynthesis are catered to the specific characteristics of the fracture. Technology, such as virtual surgical planning, intraoperative navigation, and intraoperative imaging, has the potential to improve accuracy of treating challenging fractures.
Key points
- •
The zygomaticomaxillary complex (ZMC) is a tetrapod structure, with articulations at the zygomaticofrontal buttress, zygomaticomaxillary buttress, infraorbital rim, zygomatic arch, and zygomaticosphenoid suture.
- •
Displaced zygomaticomaxillary fractures cause midfacial flattening and widening.
- •
The zygomatic arch is difficult to visualize directly, and ZMC fractures are often treated with open reduction via minimal access incisions.
- •
The decision to perform one-, two-, three-, or four-point fixation of the zygomaticomaxillary complex depends on individual fracture characteristics.
- •
Reduction of the zygomatic bone to the greater wing of the sphenoid should be checked in all but single-point approaches, because it provides the most sensitive evaluation of three-dimensional reduction of the ZMC with the skull base.
Introduction
Fractures of the zygomaticomaxillary complex (ZMC) are common injuries, representing up to 25% of facial fractures. In athletes, ZMC fractures can result from low- or high-velocity midfacial trauma. Helmets have reduced the incidence of injury, but ZMC fracture is still common in baseball, basketball, and sports with a predisposition to falls from moderate heights, such as horseback riding, , among others.
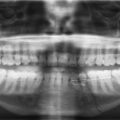
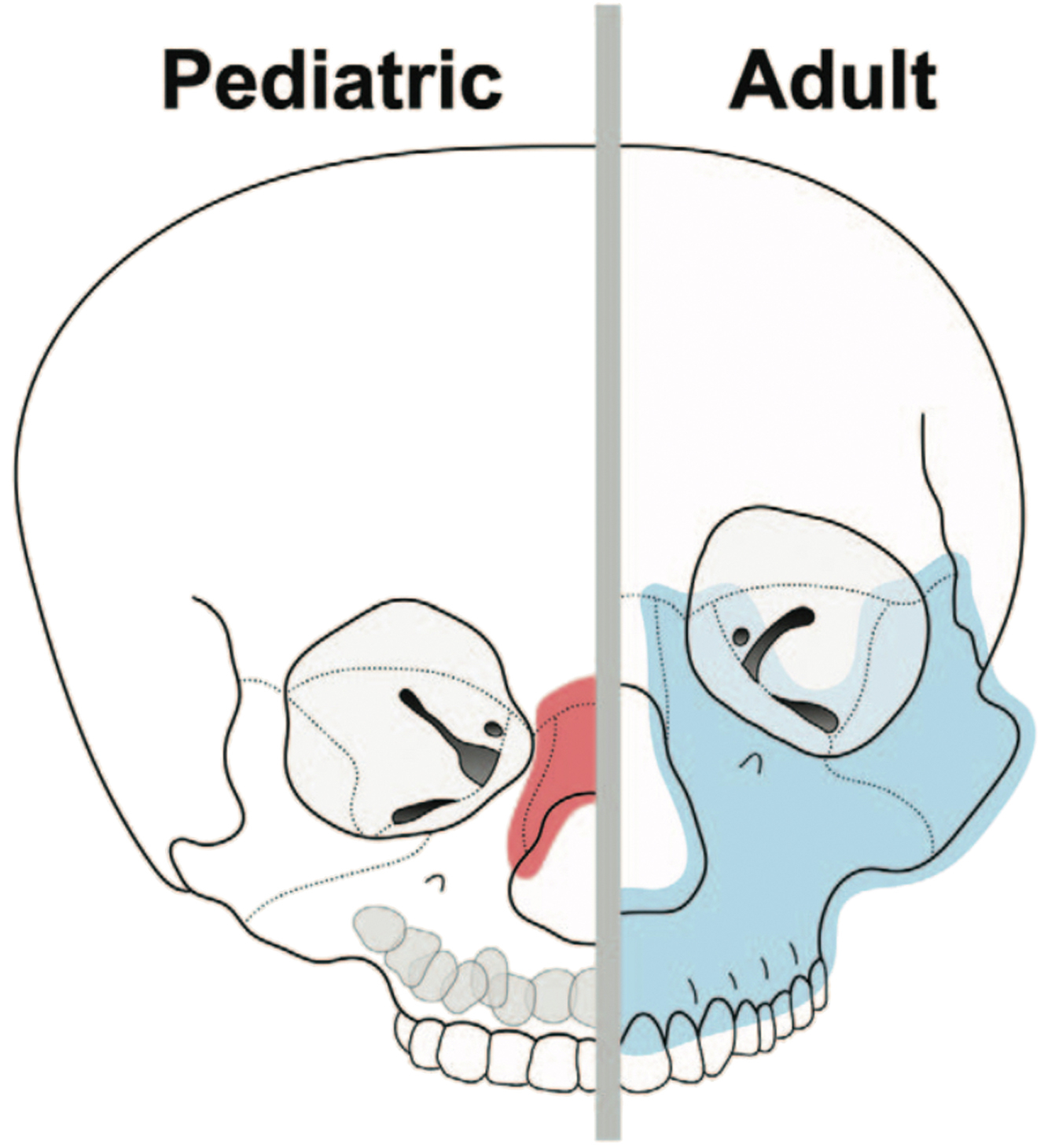
The midface undergoes a substantial increase in size and ossification during the adolescent growth phase. Children have a greater cranial-to-facial proportion, more flexible skeletal suture lines, unerupted dentition, and thicker overlying soft tissue, making midfacial fractures less common in young athletes than in late adolescents and adults ( Fig. 1 ). Fractures of the zygoma are about 70% less common in pediatric patients than in adults, and are uncommon before development of the globe pneumatization of the maxillary sinus is complete, about age 7. The mechanism of injury, advances in protective equipment, and the age of typical athletes make ZMC fractures less common in athletes than in the general population, accounting for 4% to 8% of facial fractures sustained in sports. , ,
Anatomy
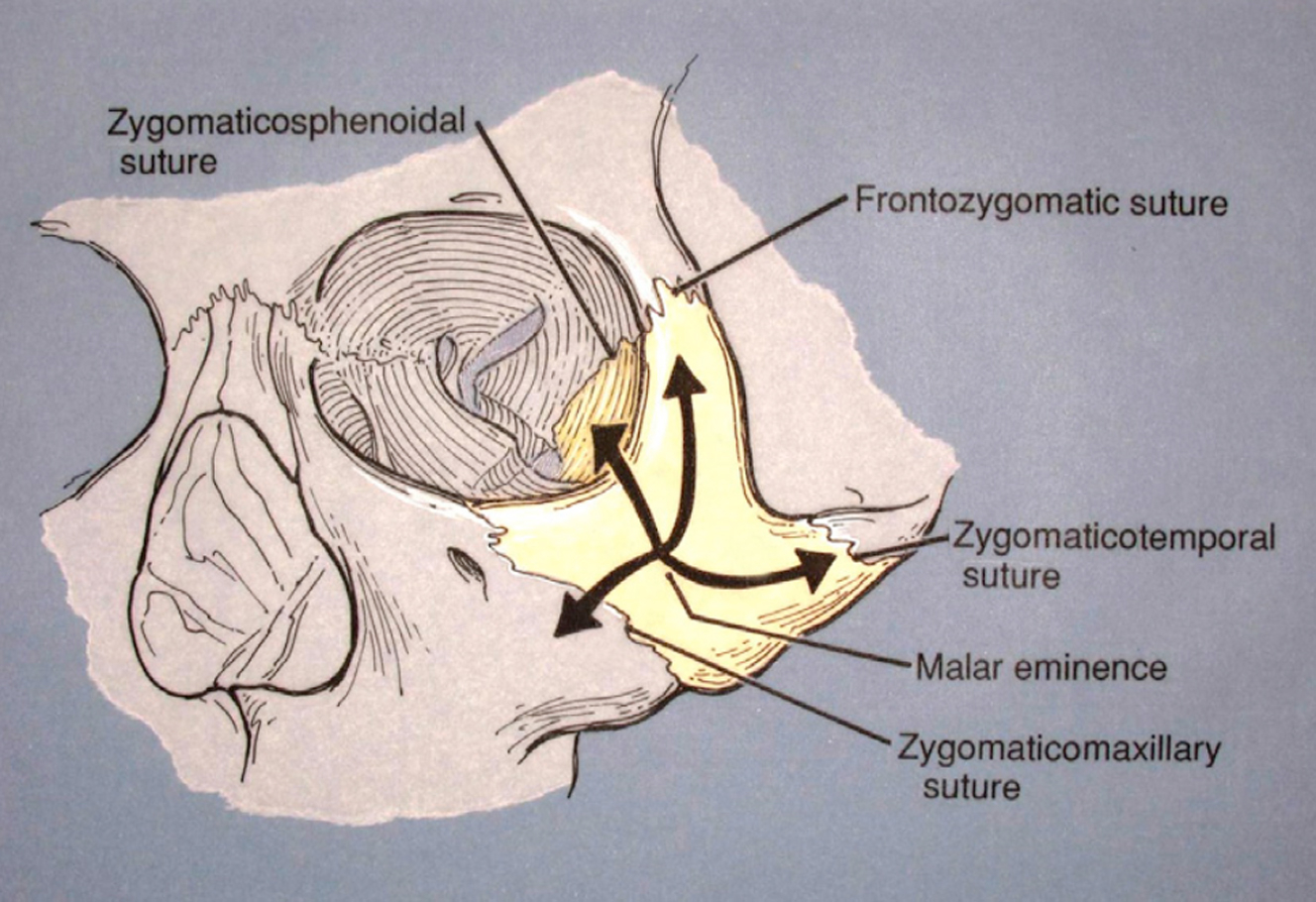
The zygoma is a tetrapod cornerstone of the midface, representing the intersection of vertical, transverse, and sagittal facial buttresses ( Fig. 2 ). The ZMC can fracture at any of these five articulations.
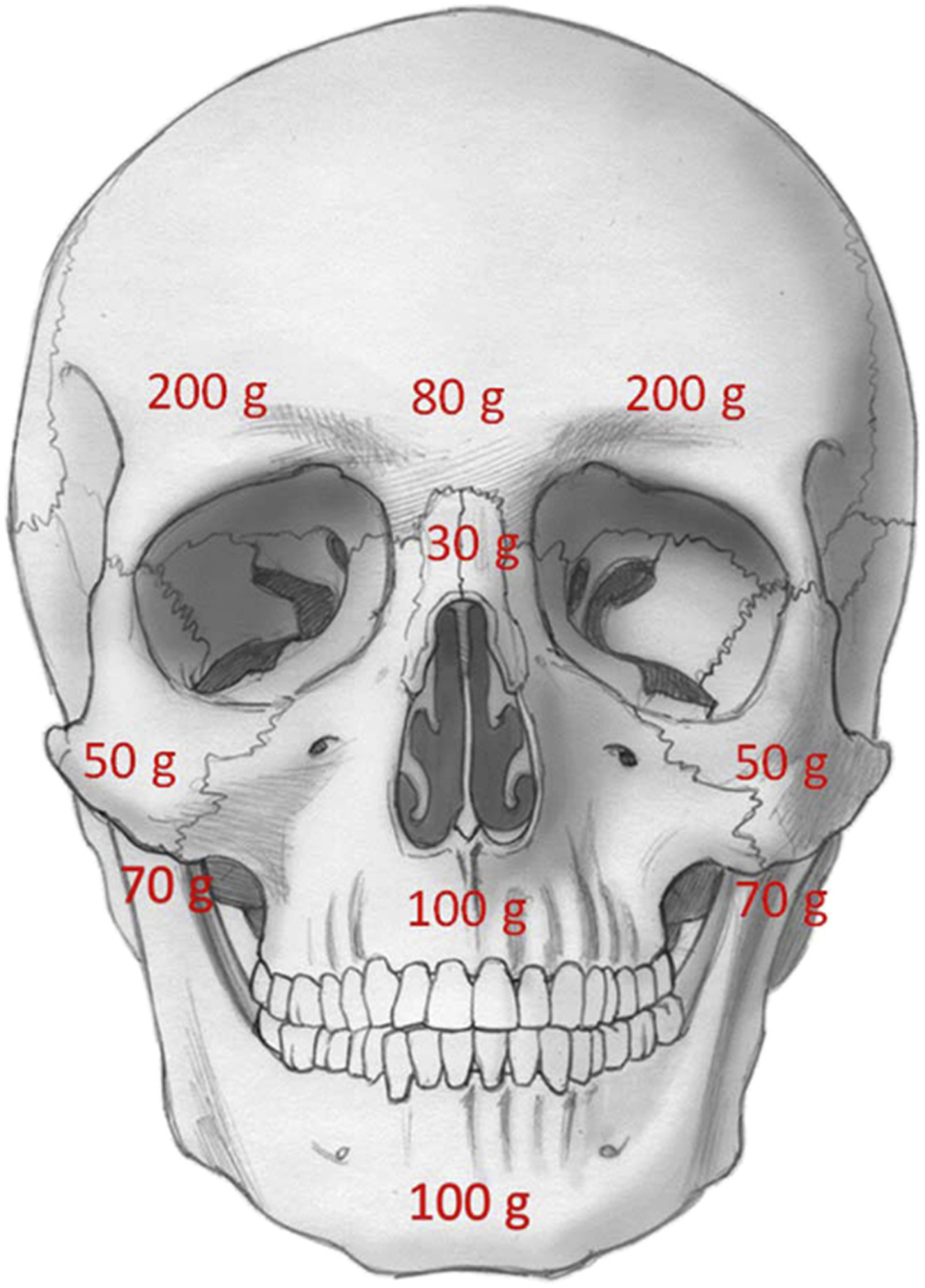
Fracture of the ZMC requires less force than most surrounding bones ( Fig. 3 ). The zygoma tends to become impacted, medially rotated, and inferiorly displaced, which leads to widening and flattening of the midface. ,
Isolated fractures of the zygomatic arch should be distinguished from those of the ZMC. The zygomatic arch typically bows inward, which may create a palpable or visible depression under the thin skin of the lateral midface.
The muscles of mastication pass from the temporal fossa and zygomatic arch to insert onto the mandible. Depressed fractures of the zygomatic arch or ZMC can cause trismus through impingement of the arch on the coronoid process of the mandible, adhesions between the arch and coronoid process, or direct injury to the muscles of mastication. ,
The superomedial portion of the zygoma creates the lateral 40% of the orbital floor. This portion of the zygoma is thin and prone to buckling with an anterior or lateral impact. For this reason, many ZMC fractures are accompanied by fractures of the orbital floor.
Evaluation
History
A complete medical history should be obtained, focusing on mechanism of trauma, comorbidities, and symptoms ( Table 1 ). High-energy athletic injuries, loss of consciousness, or the presence of spinal pain or peripheral neurologic symptoms necessitate a full trauma work-up. In children, zygomatic and orbital fractures have a higher likelihood of accompanying cervical spine injury. , Baseline visual changes should be identified. Recent use of nonsteroidal anti-inflammatory agents or anticoagulants may warrant discussion of the risk of perioperative bleeding. ,
| Skeletal detormities | Ocular/ophthalmic symptoms | Sensory impairment | Oral symptoms | Nasal symptoms |
|---|---|---|---|---|
|
|
|
|
|
Physical Examination
A more accurate assessment is conducted after edema subsides, about 5 to 7 days post-trauma. Malar retrusion accompanies most operative fractures. Step-offs may be palpable or visible along the buttresses. Pseudoptosis, vertical dystopia, inferior displacement of the lateral canthus, or increased scleral show may be more subtle signs of displacement.
Infraorbital hypoesthesia is often present, extending onto the upper lip and dentate maxilla. Trismus can represent an operative indication; approximately 4.5 cm of interincisal opening is necessary for full function. Subjective malocclusion may occur secondary to altered sensation in the region of the maxillary premolars and molars.
Signs of orbital trauma should be evaluated (see Table 1 ). Subconjunctival hemorrhage is a sensitive indicator of orbital fracture. , , With concomitant orbital floor fractures, emergencies, such as entrapment, superior orbital fissure syndrome, orbital apex syndrome, and retrobulbar hematoma, must be ruled out. Concomitant major ocular or blinding injuries may be present in about 10% of patients; thus, consideration should be given for ophthalmologic evaluation in all ZMC fractures. ,
Radiographic Evaluation
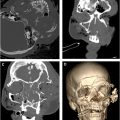
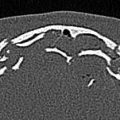
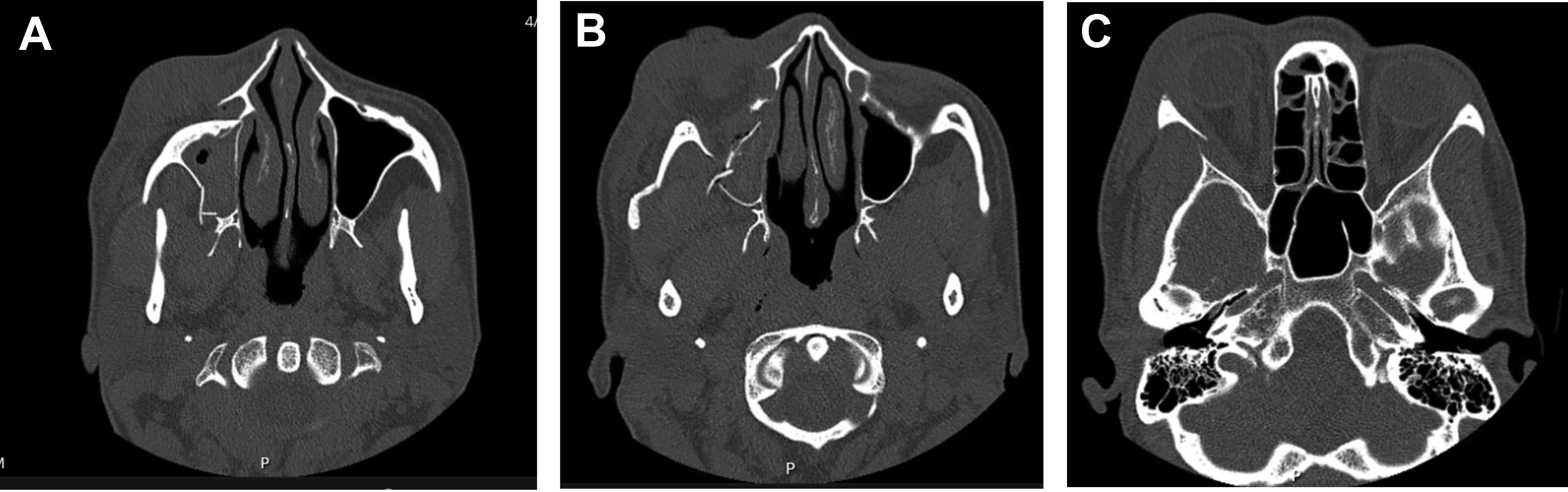
Maxillofacial computed tomography (CT) with thin cuts (0.625–1.0 mm) is the gold standard in evaluating for zygomaticomaxillary fractures. , In children, low-dose radiation protocols can limit exposure to ionizing radiation. Fracture lines and displacement are evaluated. On axial imaging, alignment of the zygomaticosphenoid buttress, infraorbital rim, and zygomatic arch is assessed ( Fig. 4 ). The zygomaticosphenoid buttress provides sagittal and transverse support to the zygoma and is a sensitive indicator of fracture displacement. , Retropositioning of the malar eminence is assessed on axial and three-dimensional imaging. Coronal and sagittal imaging are best to examine fractures and displacement of the zygomaticofrontal and zygomaticomaxillary buttresses. The degree of comminution should be noted, because this influences the number of points of fixation needed.
Operative management
Virtual Surgical Planning
Preoperative virtual surgical planning (VSP) allows identification and reduction of individual fracture segments. Reduction is based on a mirror image of the uninjured contralateral side. In bilateral injuries or baseline deformity, a representative normative scan matched to the age and gender of the patient is used. Stereolithographic models are three-dimensional printed, modeling the fractured skeleton for better conceptualization, or simulating the reduced ZMC to prebend osteosynthesis plates. Custom implants are fabricated to guide the proper skeletal reduction. VSP session data are combined with intraoperative navigation to compare the preoperative plan with operative execution. , ,
Timing and expense are barriers to widespread adoption. Commercial fabrication of custom-printed osteosynthesis plates currently takes approximately 2 weeks from the time of CT data submission. For acute trauma, timing is often not prompt enough to make VSP application practical, particularly for all but the most complex zygomaticomaxillary cases. With technologic advances and institutional sourcing, VSP may be more commonly used in the future.
Timing
Allowing time for facial edema to subside improves the precision of evaluating operative indications, while facilitating access through concealed incisions. However, by 2 to 3 weeks postinjury, fractures begin to heal, particularly in younger athletes, making accurate reduction more challenging. Most surgeons prefer to operate at 1 to 2 weeks postinjury.
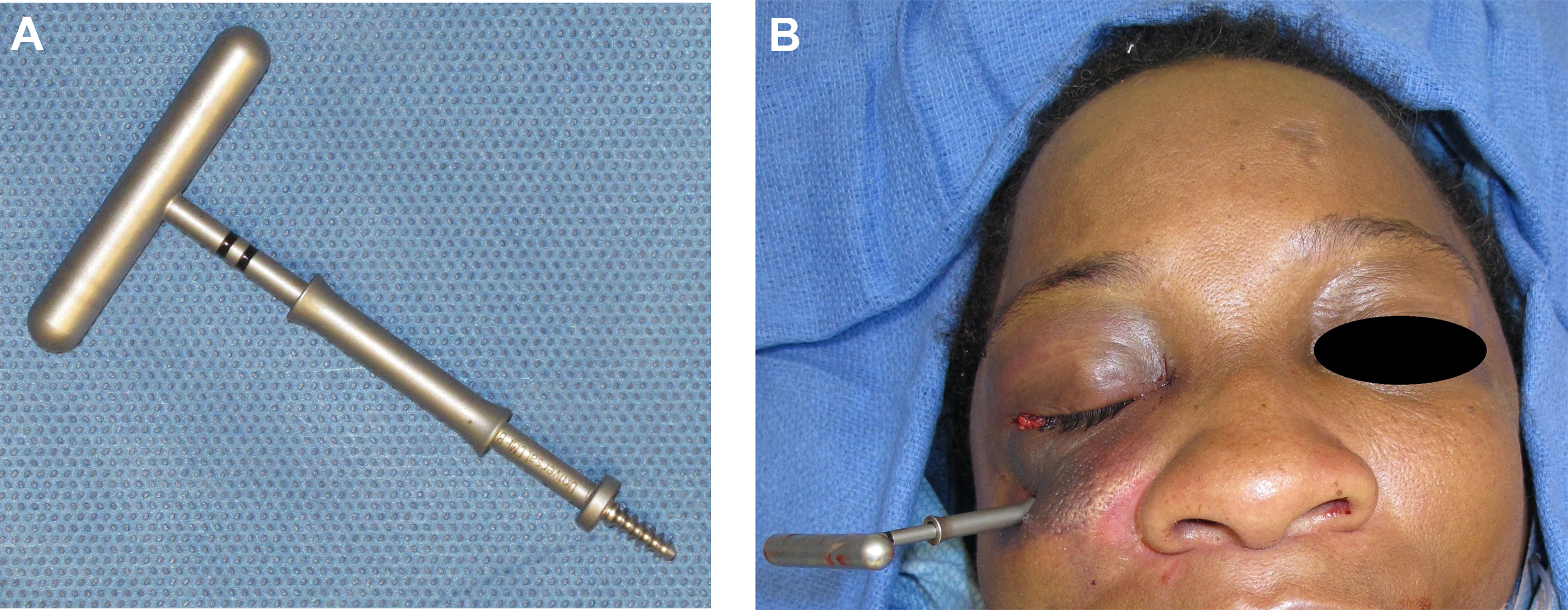
Closed Reduction
Closed reduction has limited indications because of the difficulty of accessing the deep aspect of the midface in the absence of incisions. For isolated zygomatic arch fractures, a bone hook is placed percutaneously over the arch, and a laterally directed force applied to achieve reduction. Similarly, a bone hook, threaded reduction tool ( Fig. 5 A), or screw is applied to the body of the zygoma, and reducing forces applied percutaneously using these tools to reduce ZMC fractures. Many fractures demonstrate inadequate stability or too significant a degree of displacement to be appropriate for these methods. The presence of a fracture along the zygomaticofrontal buttress is predictive of failure of closed reduction, and displacement at this location is an indication for open reduction with internal fixation. Because of the risk of concomitant orbital fracture, forced duction should be completed after closed ZMC reduction to assess for entrapment caused by fracture reduction.