The initial evaluation of maxillofacial trauma in athletes should first focus on the management of life-threatening injuries that require emergent care. Airway, breathing, and circulation are the 3 areas to be addressed first and foremost, as set forth by Advanced Trauma Life Support (ATLS) guidelines. Following the stabilization of the patient, a thorough physical examination and systematic review of any relevant imaging studies are imperative to ensure that injuries are not missed. Ultimately, management by the facial plastic surgeon should balance the goals of facial trauma restoration with the overall needs of the patient.
Key points
- •
Following Advanced Trauma Life Support (ATLS) guidelines is paramount in the management of patients with facial trauma.
- •
Establishing and maintaining a safe airway precedes all other interventions. Facial trauma specifically can create tenuous airways requiring multiple modalities or techniques for the management.
- •
A thorough head and neck examination, including a neurologic and ophthalmologic examination, can provide insight into underlying maxillofacial fractures.
- •
Nasal injuries are the most common facial injuries across all sports. Epistaxis management includes pressure, packing, and ultimately ligation or embolization.
- •
Computed tomography is the gold standard for the radiographic evaluation of maxillofacial trauma.
Introduction
In the United States (US), each year, more than 400,000 emergency room visits are related to facial injuries, up to 30% of which may be sports-related. The National Youth Sports Foundation for the Prevention of Athletics Injuries in the US estimates that athletes have a 10% chance of sustaining maxillofacial injury during each sports season. , These injuries are complex, and although rarely life-threatening, can affect the functionality or cosmesis of the face.
Previous studies have shown that 11% to 40% of all sports-related injuries involve the face. These injuries may be related to falls, interplayer contacts, and impacts from sporting equipment. In the US, sports-specific patterns of injury in adults are not well established; among the pediatric population, more than 43% of facial trauma is attributed to baseball or softball. Throughout the world, cultural and socioeconomic differences contribute to the variability of trends in sports popularity and resultant sports-related injuries. As such, most injuries occur from soccer in Italy and France, basketball in Japan, soccer in South Korea, ice hockey in Finland, and skiing in Austria and Switzerland.
Soft tissue injuries, as well as facial bone fractures, occur frequently in athletes with the nasal bone, mandible, and zygoma being the most common subsites. Nasal bone fractures account for up to 50% of all sports-related fractures, whereas zygomaticomaxillary complex (ZMC) and mandibular fractures each account for another 10%. The type of sport can also influence maxillofacial fracture patterns which was illustrated in a German study of 3596 patients showing that ball sport accidents lead to significantly more midface fractures than mandibular fractures.
Prompt evaluation by a facial plastic surgeon can allow for the early recognition of maxillofacial trauma that may require emergent intervention. Early surgical intervention, when indicated, has been demonstrated to improve esthetic and functional outcomes. The ultimate goal of the facial trauma surgeon is the restoration of the face and its functions to the preinjury state.
Primary survey
Approximately 25% to 30% of trauma-related deaths can be prevented by using a systematic approach to evaluating the patient. The goal of the initial trauma assessment is to recognize life-threatening injuries and establish an organized treatment plan to aggressively manage urgent issues. When considering patients with trauma as a whole, injuries are missed in up to 65% of patients. For this reason, following the stabilization of the patient, the trauma team should perform serial examination to avoid missing injuries.
On arrival, a history of the patient’s mechanism of injury, vital signs, and interventions provided in the field should be clearly communicated from the emergency medical services (EMS) team to the receiving hospital care team. The mechanism of injury can provide clues into different patterns of facial fractures and insight into other underlying injuries that may not be immediately recognized. For example, high-velocity motor vehicle collisions more commonly cause complex and multifocal fractures than falls, fights, or sports-related injuries. , ,
Following the transfer of the patient to the trauma bay bed, the usual sequence of events includes the primary survey, the stabilization of the patient, the secondary survey, and the establishment of a definitive care plan. The most common system to describe a patient’s status is the Glasgow Coma Scale (GCS). Patients with a GCS score between 3 and 8 require urgent management, generally including endotracheal intubation. Ensuring airway protection may still be indicated in patients with GCS score greater than 8 in the case of maxillofacial trauma causing airway compromise.
The primary survey is based on the “ABCDEs” of trauma as described by the American College of Surgeons Advanced Trauma Life Support: Airway, Breathing, Circulation, Disability, and Exposure. , , We will focus our discussion on the first 3 and how they pertain to patients with maxillofacial trauma.
“A” for airway assessment and management
Assessing the Airway
Determining airway patency is of utmost importance, especially in patients with head and neck injuries or maxillofacial trauma. Poor systemic oxygen delivery can lead to loss of consciousness, end-organ failure, and ultimately death. An easy way to quickly determine airway adequacy is by assessing a patient’s ability to respond to questions. , A patient that is lying flat and able to speak with normal vocal projection and without too frequent of breaks in speech to catch their breath likely has a patent airway.
The thyroid cartilage should be assessed for midline positioning and irregularities that suggest a fracture. Crepitus felt in the neck or air bubbles emerging from a neck wound may result from a tracheal injury. Maxillofacial trauma can contribute to airway obstruction from bleeding, posterior mobility of the maxilla to the nasopharynx, prolapse of the tongue to the posterior oropharynx in mandibular fractures, or displaced dentition, and other foreign bodies. Not surprisingly, it has been previously shown that complex fractures are more commonly associated with airway compromise and the need for tracheostomy. Other potential causes of airway obstruction include emesis, lingual edema, and traumatic brain injury.
Signs and symptoms of airway obstruction include
- •
Agitation or use of accessory respiratory muscles
- •
A need to preferentially sit upright
- •
Rapid shallow breaths
- •
Hypoxia demonstrated on pulse oximetry
- •
Cyanosis suggesting hypercarbia
- •
Stridor
- •
Deviated laryngotracheal framework
- •
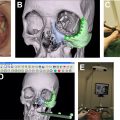
Options for securing the airway are discussed below and summarized in Fig. 1
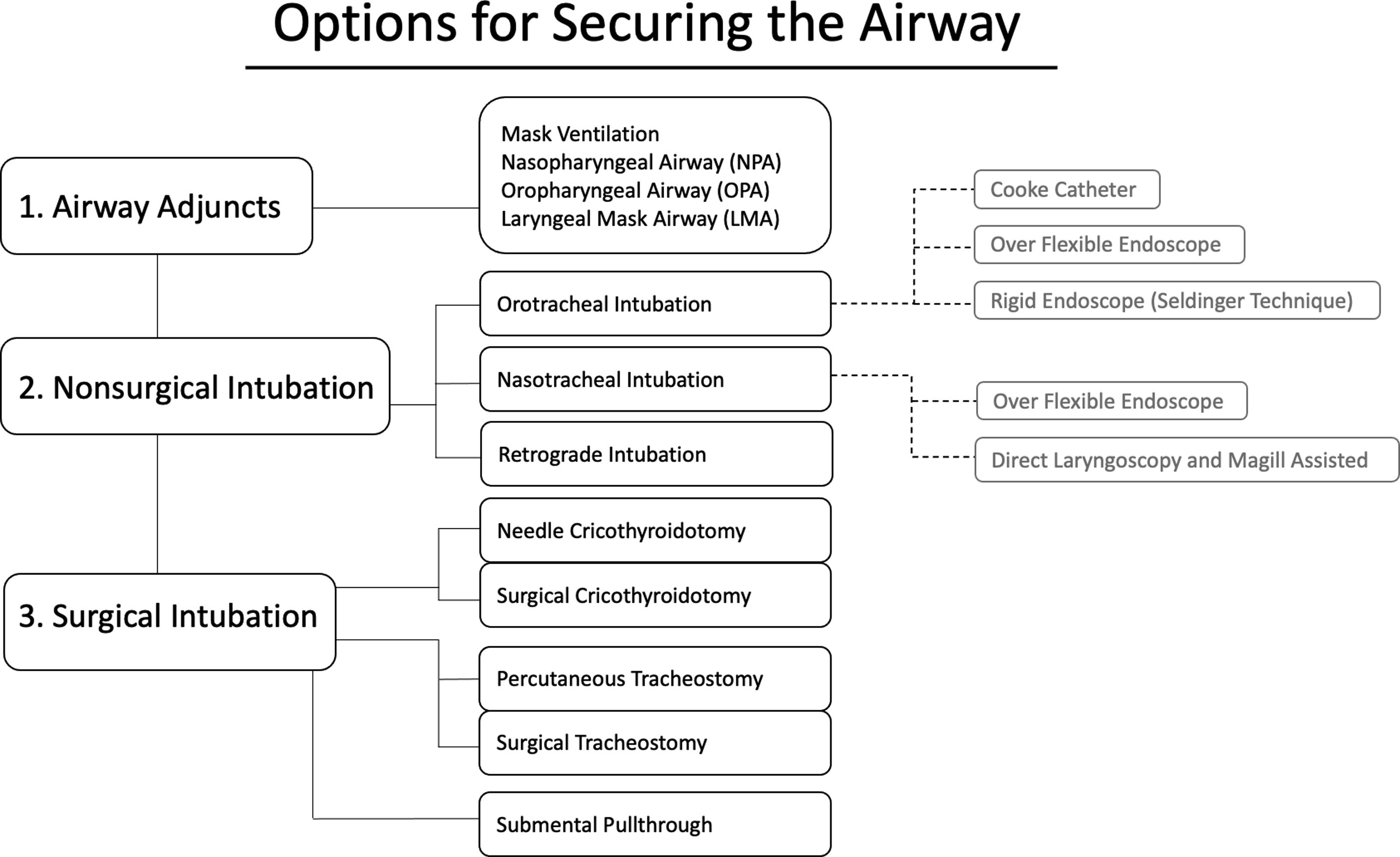
Fig. 1
Multiple tools and methods exist for establishing a safe and secure airway in patients with maxillofacial trauma. The decision on which technique to use depends on individual patient circumstances, available resources, existing injuries, other contraindications for certain techniques, and practitioner comfort and preference.
Nonsurgical Airway Management
Initially, patients are provided with supplemental oxygen via mask or nasal cannula. Placement of a nasopharyngeal (NPA) or oropharyngeal (OPA) airway is a quick adjunct to bypass an enlarged tongue. If more airway support is required, the bag valve mask is an essential tool because it provides positive pressure ventilation and can even act as a definitive airway if used correctly.
Escalation of airway management then moves to intubation. A greater number of facial fractures and more complex fracture patterns both confer an increased risk of cervical spine injury. If a cervical collar must be removed to establish a definitive airway, another team member should manually stabilize the head and neck. The jaw thrust and chin lift are 2 maneuvers that can assist in safely opening the oral airway without compromising the spine.
In brief, orotracheal intubation typically involves direct or video laryngoscopy followed by the placement of an endotracheal tube (ETT). Appropriate positioning of the tube can be confirmed by the visualization of the tube passing through the vocal folds, end-tidal carbon dioxide using capnography, and bilateral auscultation for even respiratory sounds. Once the positioning is confirmed, the tube should be properly secured.
When standard orotracheal intubation is difficult, other options exist before obtaining a surgical airway. A small diameter elastic bougie can pass through the glottis more easily. An ETT is then passed over the bougie into position. Rescue airway devices including the laryngeal mask airway (LMA) or fiberoptic intubation are alternatives. Nasotracheal intubation using a fiberoptic scope is a good option for patients with a potentially difficult airway ( Fig. 2 ) who must maintain spontaneous ventilation. This method is occasionally contraindicated in the case of midface and skull-base trauma because of the risk of brain injury or cerebrospinal fluid leak.

Retrograde intubation may be considered when a flexible scope is not available or bleeding makes scope visualization difficult. A thin guide wire is passed through the cricothyroid membrane and aimed cephalad, passing through the glottis into the oral cavity. A flexible ETT can then be passed over the guide until its tip is engaged at the laryngeal inlet. While applying axial pressure over the ETT tip to hold it in place, the guide is removed and the ETT is then advanced distally into the trachea.
The Surgical Airway
In certain cases, intubation may not be possible and obtaining a surgical airway may be necessary. One of the fastest means of obtaining an airway is with a cricothyroidotomy. This involves an incision through the cricothyroid membrane, followed by the dilation of the tract to accommodate a small ETT. A needle cricothyroidotomy is also an option; however, this is only a temporizing measure. A needle cricothyroidotomy can facilitate translaryngeal jet ventilation for approximately 30 minutes, with hypercarbia noted beyond that time.
Tracheostomy is preferentially performed in children to avoid injury to the cricoid cartilage during a cricothyroidotomy. For practitioners with advanced training in airway management, expeditious awake tracheostomy may be an option even in an unstable patient.
The surgical plan itself can dictate subsequent airway management after securing the airway at the time of presentation. For mandibulomaxillary fixation (MMF), nasotracheal intubation or tracheostomy is often indicated; however, orotracheal tube may be routed behind the dentition still allowing for MMF. Alternatively, a submental pull-through involving tunneling an oral ETT through the floor of the mouth and submental soft tissues may also be a viable option. Lastly, as part of a multidisciplinary trauma team, it is prudent to consider tracheostomy for patients with polytrauma who may require prolonged intubation.
“B” for breathing
Once the airway has been secured, the patient should be assessed for adequate gas exchange to prevent hypoxemia and hypercarbia. Head injuries may affect respiratory drive, whereas spinal injuries above the levels of C3 to C5 may impact the phrenic nerves and subsequently the movements of the diaphragm. As a result, the neck and chest should be fully exposed to allow for adequate inspection and palpation with special attention to tracheal deviation, neck injuries, rib fractures, chest wall emphysema, and use of accessory muscles such as supraclavicular retractions.
Thoracic injuries including flail chest, hemothorax, and pneumothorax can also result in inadequate ventilation. If these injuries are suspected, a chest radiograph should be obtained promptly as needle decompression or chest tube placement may be necessary, especially in the case of a tension pneumothorax.
“C” for circulation
Hemorrhage accounts for 30% to 40% of preventable deaths in patients with trauma. Resuscitation starts with establishing intravenous access with at least 2 large-bore intravenous catheters. Patients can initially receive crystalloid solutions; however, a blood transfusion may still be needed. Administration of blood products has the added benefit of repleting the circulatory system’s oxygen-carrying capacity. Response to fluid resuscitation is assessed by monitoring the patient’s vital signs, mental status, urinary output, and acid–base laboratories.
The head and neck anatomy is well vascularized, and soft tissue injuries in this area can lead to significant bleeding. Up to 4.5% of patients with maxillofacial trauma experience life-threatening hemorrhage and subsequent hemorrhagic shock. Scalp lacerations may be missed if the patient is hypovolemic, but when recognized can be quickly stabilized with Raney clips, staples, or sutures. In the case of oral bleeding from mandibular fractures, bridle wires or arch bars can temporize the bleeding.
Epistaxis Management
In a review of 312 patients, Buchanan and colleagues found a 4% incidence of epistaxis across all facial fractures and an 11% incidence among midface fractures. Nasal injuries are the most common facial injury across all sports, and both nasal bone fractures and isolated mucosal trauma can be associated with epistaxis. Initial epistaxis management includes applying firm digital pressure over bilateral nasal ala and tilting the head forward to prevent OPA rundown, which can induce further anxiety, coughing, and emesis. Oxymetazoline ( Afrin ) is a topical decongestant that binds alpha-adrenergic receptors causing vasoconstriction and can be sprayed directly into the nares. Absorbable packing materials such as Nasopore and nonabsorbable packing materials such as Merocel can be used as adjuncts when digital pressure does not sufficiently control nasal bleeding.
Formal packing such as Rhino Rocket can be used to control massive bleeding from posterior and anterior sources. Traditional packing for posterior epistaxis involves using a Foley catheter balloon to tamponade the bleed at the level of the choanae/nasopharynx. Occasionally, surgical exploration and ligation, or embolization by interventional radiology may be needed for offending vessels that are difficult to control with packing.
Secondary survey
Once the primary survey is completed and any life-threatening conditions are adequately managed, the secondary assessment is undertaken with a subjective and objective examination of the patient. A history of the incident and brief medical history should be obtained from the patient or from family members, friends, or witnesses. The objective portion of the assessment includes a thorough head and neck examination; determination of neurologic status; and examination of the chest, abdomen, and extremities.
Neurologic Examination
If the patient exhibits altered mentation, neurologic deficits, seizure activity, or brief loss of consciousness, a computed tomography (CT) scan of the head is required to assess intracranial injury.
The neurologic examination includes assessment for pupillary asymmetries, cranial nerve (CN) deficits, and any localizing signs. Deficits of CN I (olfactory) suggest injury to the cribriform plate. An ocular examination involves the assessment of vision mediated by CN II (optic), and movement of the orbit which is controlled by CN III (oculomotor), CN IV (trochlear), and CN VI (abducens). Discrepancies between bilateral facial sensations may suggest injuries to the branches of CN V (trigeminal).
Similarly, injury to CN VII (facial) would cause facial asymmetry. In an obtunded patient, a sternal rub may elicit a grimace revealing the dynamic facial function. As a general principle, suspected injuries to the branches of the facial nerve proximal to a vertical line drawn from the lateral canthus may benefit from surgical exploration, whereas injuries distal to this line are more likely to spontaneously recover function due to arborization. The gag reflex can be used as a surrogate for CN IX (glossopharyngeal) and CN X (vagus) function. Checking strength with shrugging the shoulders and turning the head would elicit an injury to CN XI (spinal accessory), and asymmetry of tongue protrusion would suggest injury to CN XII (hypoglossal).
Orbital Examination
Examination of the orbit is crucial. Up to 40% of orbital blowout fractures may be associated with ocular injury, ranging from minor to major. A preliminary ocular examination should evaluate pupil reactivity, globe position, visual acuity, range of extraocular movements for the evidence of entrapment, chemosis (swelling of the conjunctiva), and hyphema (blood within the anterior chamber). If any serious injury is suspected, the eyes should be protected adequately until a formal examination can be performed by an ophthalmologist, because any increased pressure onto an already compromised eye can lead to permanent vision changes.
Examination for Facial Fractures and Lacerations
Starting at the apex of the scalp, the maxillofacial skeleton should be thoroughly and systematically inspected. Battle sign (ecchymoses over the mastoid), raccoon eyes (ecchymoses around the orbits), hemotympanum, and persistent clear or red-tinged rhinorrhea concerning cerebrospinal fluid leak are all signs of fractures of the skull base.
Asymmetries and swelling of portions of the face may provide clues to underlying facial fractures. These should be further assessed with palpation for step-offs or crepitus along the frontal bones; supraorbital, lateral, and inferior orbital rims; the nasal bones; malar prominences; zygomatic arches; the maxilla; and the mandible. Figs. 3–5 depict an illustrative case.