A dentoalveolar fracture requires thorough clinical and radiographic examination for an accurate diagnosis to guide appropriate treatment. Dentoalveolar fractures can be classified into the following 4 groups: (1) crown/root fractures, (2) luxation/displacement of teeth, (3) avulsion, and (4) alveolar fractures. Treatment can be divided into nonrigid fixation (splinting with wires and composite) and/or rigid fixation (Erich arch bars, Risdon cable wires) depending on the extent of dentoalveolar fractures. Special considerations must be made for primary teeth and mixed dentition to avoid injuring tooth buds and arising permanent dentition.
Key points
- •
Dentoalveolar fracture can be classified into the following 4 groups: (1) crown/root fractures, (2) luxation/displacement of teeth, (3) avulsion, and (4) alveolar fractures.
- •
Crown/Root fractures require thorough examination and evaluation of the viability of the tooth.
- •
Avulsion and luxation of teeth are managed through repositioning to the original position and require nonrigid fixation (splinting) for 2 weeks.
- •
Alveolar fracture requires rigid fixation (Erich arch bars, Risdon cable wires) for 4 weeks.
- •
Special considerations must be made for the pediatric population because of primary and mixed dentition phases.
Introduction
Dentoalveolar trauma is an important public health problem that has a significant physical, economic, and psychosocial burden on the individual. It has been reported that in the United States alone, the lifetime costs of bodily injuries are approximately $406 billion. Global epidemiologic studies indicate that the annual incidence of dental trauma is approximately 4.5%. The prevalence of dental injuries range from 6% to 59%, which affects one-third of the pediatric population and one-fifth of adolescents/adults sustaining a traumatic dental injury in their lifetime. Furthermore, studies have indicated that 48% of facial injuries involve the oral cavity, which increases morbidity and mortality. Owing to the variability in accessing dental resources at various hospital centers and because most patients with dentoalveolar injuries require long-term observation and follow-up, most treatments are deferred to outpatient dental care. The discrepancy of access and affordability to indicated dental services often means that patients do not present to a dentist after dentoalveolar fracture until months after an injury and many injuries remain undiagnosed. The purpose of this article is to explore clinically relevant classifications of dentoalveolar injury management and the importance of concomitant management and treatment of dentoalveolar fractures with maxillofacial fractures.
Evaluation
Initial evaluation of dentoalveolar injuries should take place within the context of a larger trauma examination. It is important to remember that intraoral evaluation is a part of the primary Advanced Trauma Life Support (ATLS) survey to ensure there are no loose debris, teeth, or massive oral hemorrhage that could lead to airway compromise. Once the patient is stabilized, formal maxillofacial examination can take place including a detailed maxillofacial examination. It is crucial to irrigate and remove debris and nonviable tissue, bone, and foreign objects to prevent aspiration risks. There are several methods for examining the oral cavity; however, the most important aspect for a clinician is consistency. The examination should be methodical to ensure facial lacerations, gross skeletal step-offs, involvement of cranial nerves, oropharynx, and dental examinations are appropriately documented.
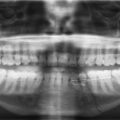
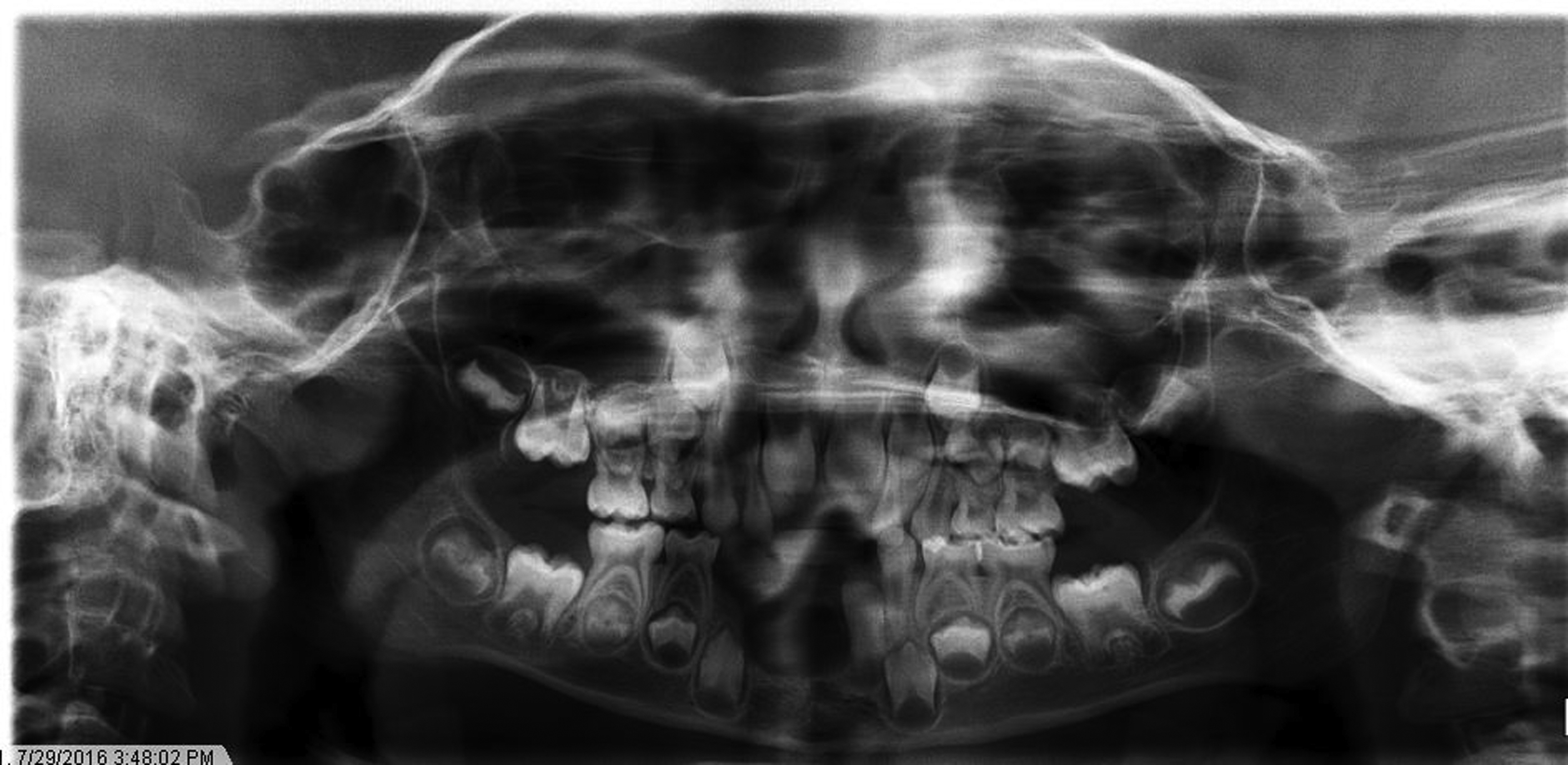
It is often easiest to begin with a soft tissue examination of the oral cavity. Oral soft tissues are highly vascularized and bleed easily, thus identifying the source of bleeding is essential to help with the remainder of the examination. The soft tissues of the gingiva, palate, lips, pharynx, and floor of mouth should be evaluated for lacerations or injuries. This is followed by a hard tissue examination, counting all the teeth in the mouth to ensure none was lost during the injury. In general, an adult can have up to 32 permanent teeth and children have 20 primary teeth. However, this can be complicated in children ages 6 to 12 years who are in the mixed dentition stage as the permanent dentition remains unerupted in the alveolus ( Fig. 1 ). If an avulsed tooth is not accounted for, a thorough review of head, neck, chest, and abdomen imaging is required to rule out aspiration, swallowing, or other displacement of the tooth.
Once the teeth are accounted for, each tooth should be visually inspected for signs of trauma, including fractured enamel, missing restorations, or gross displacement. After visual inspection, palpation of the dental arches should be completed specifically looking for the mobility of individual teeth or alveolar segments, which helps differentiate between dentoalveolar injury and more extensive trauma like mandibular fracture. Furthermore, radiographic imaging is warranted for the comprehensive diagnosis of dentoalveolar and maxillofacial fractures.
Imaging
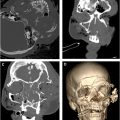
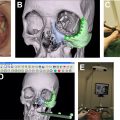
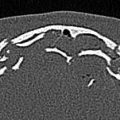
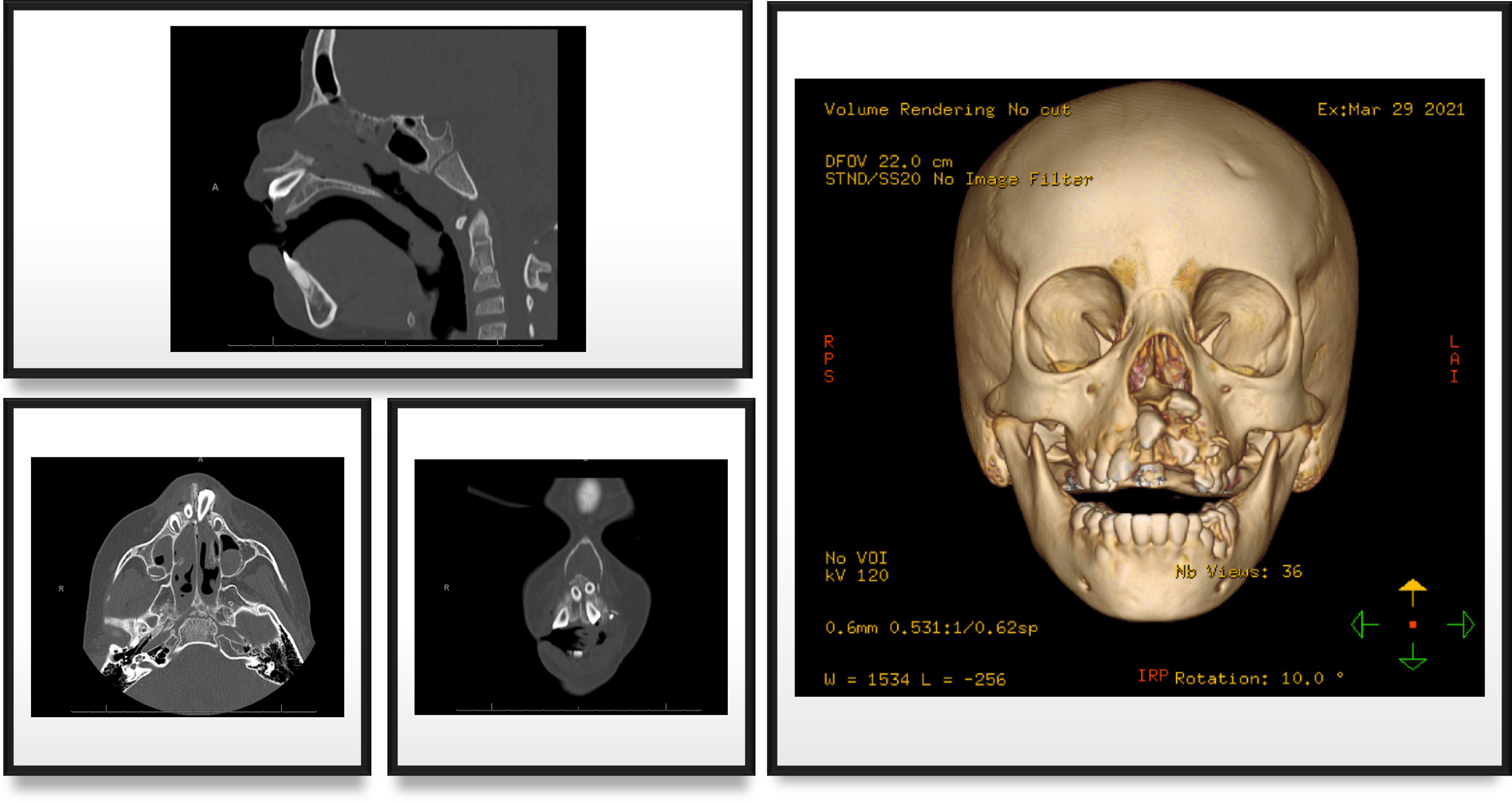
There are numerous different imaging options available for the diagnosis of dentoalveolar trauma, and the choice of imaging is largely based on the modalities available and the extent of injury. In this hospital setting, trauma patients with clinical signs of facial injury will often undergo maxillofacial computed tomography (CT) scans, which can be used to diagnose dentoalveolar trauma ( Fig. 2 ). Maxillofacial CT allows for complete visualization of skeletal and soft tissue structures, which is useful to visualize airway patency, soft tissue infection, and differentiate between isolated dentoalveolar injury and more extensive facial fractures such as maxillary and/or mandibular fractures. However, if clinical suspicion for complex facial injury is low and there are concerns for radiation exposure, dental radiographs allow excellent visualization and have less radiation. This is particularly useful in the pediatric population where the panoramic x-ray allows visualization of unerupted teeth (see Fig. 1 ).
Periapical and bitewing imaging is useful in the diagnosis of isolated dental injury or periodontal injury. They provide accurate evaluation of dental anatomy and integrity, which can facilitate dental restoring and rehabilitating. Panoramic imaging can also be useful as a screening tool for evaluation of the entire dentition in one clear image. Although both these images are clinically most accurate at a low cost and low radiation exposure, they are only available in outpatient dental clinics and not the emergency room. It is important to refer these patients to dentists after discharge for further evaluation and treatment.
Lastly, photographic documentation can be very useful in cases of facial and dentoalveolar trauma. Photos allow for monitoring of soft tissue healing as well as changes in tooth coloration, which may indicate pulp necrosis and affect long-term treatment planning.
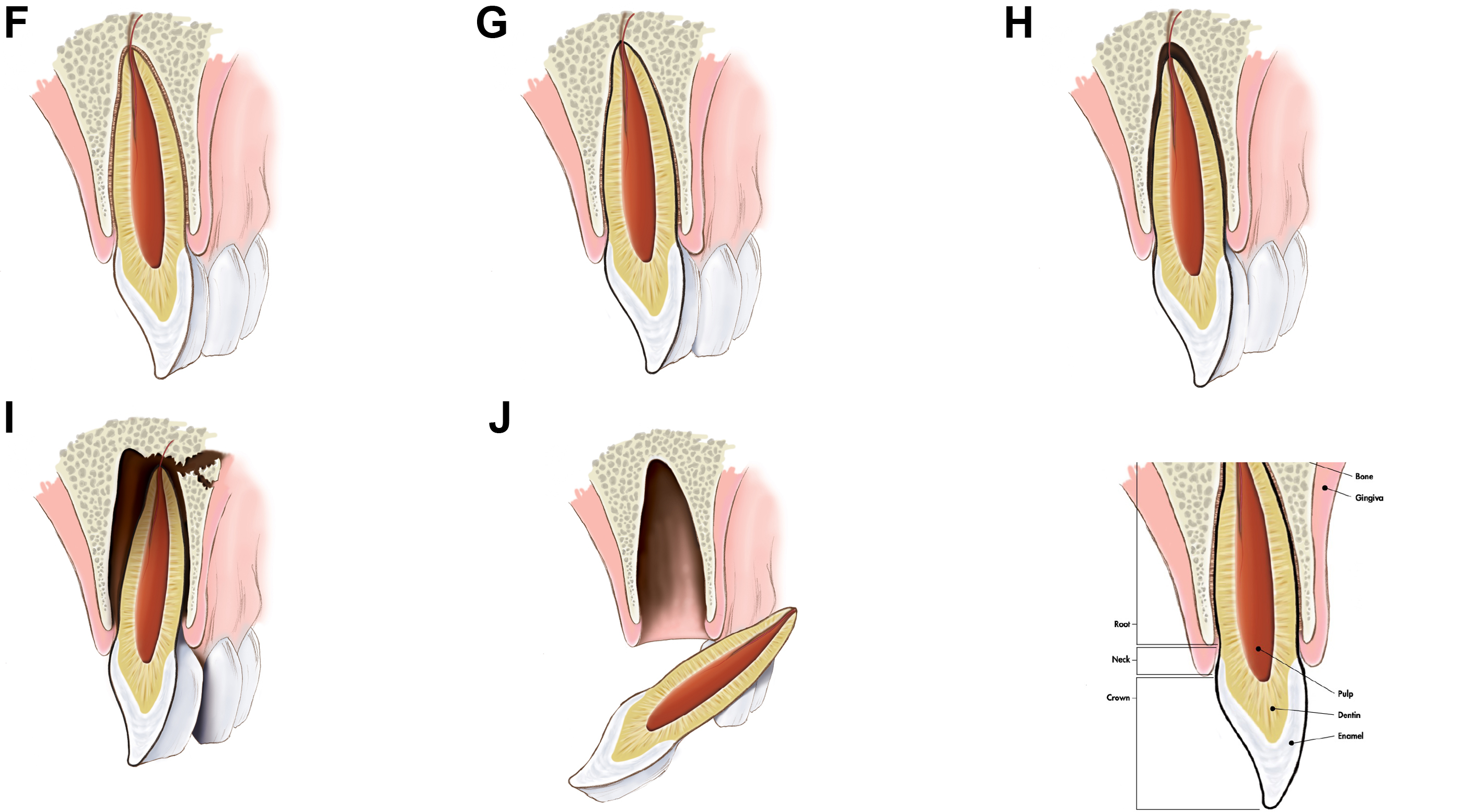
The classification of dentoalveolar trauma can be classified within the following 2 broad categories:
- 1.
dentoalveolar injury ( Fig. 3 )
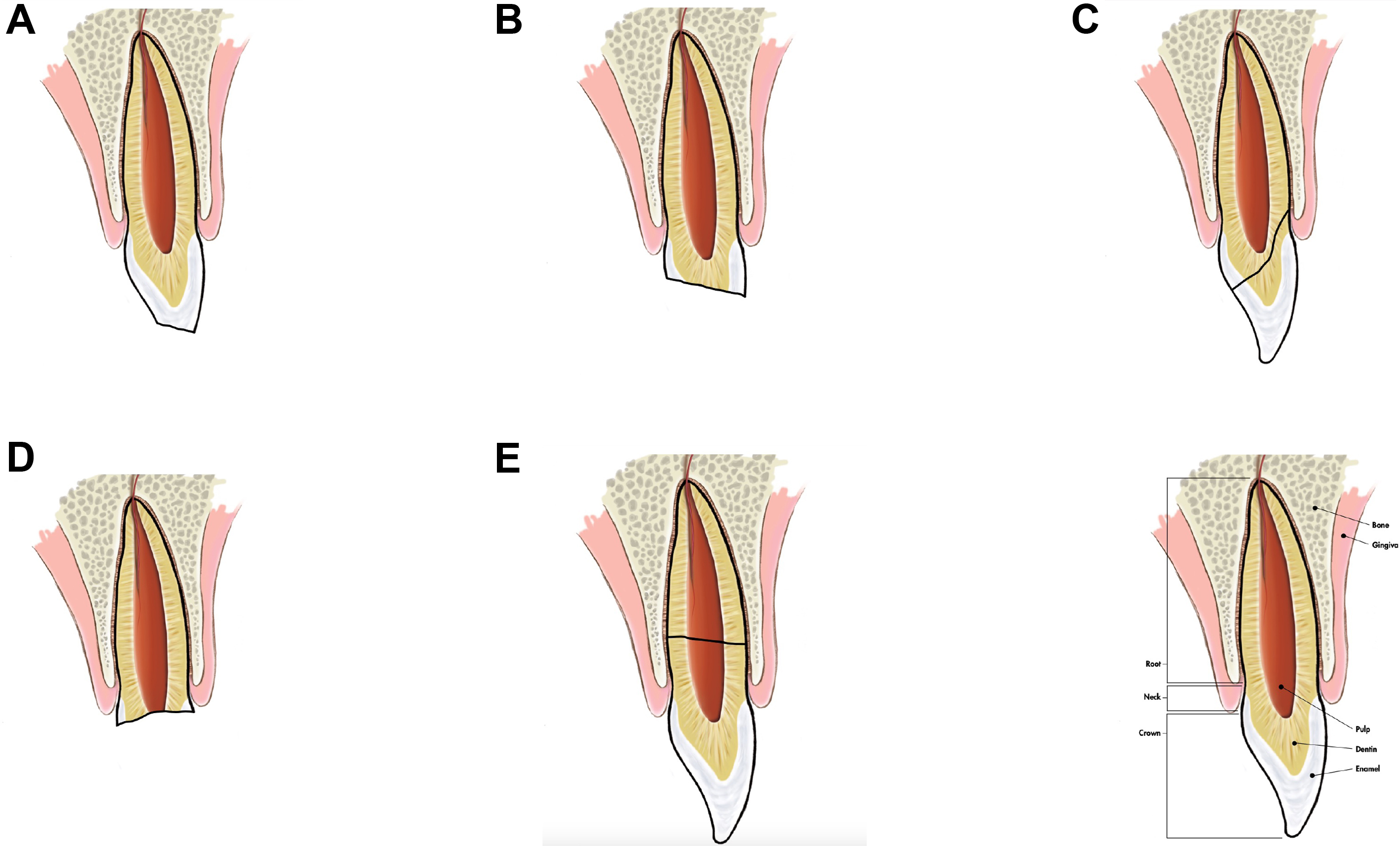
Fig. 3
Classification of dentoalveolar injury correlating to Table 1 .
(From Reynolds JS, Reynolds MT, Powers MP. Diagnosis and Management of Dentoalveolar Injuries. Fourth Edi. Elsevier Inc.; 2013. doi:10.1016/b978-1-4557-0554-2.00013-7)
- 2.
subluxation/alveolar injury ( Fig. 4 ).