Fractures of the mandibular body most commonly occur after interpersonal violence or motorized vehicle accident but can occur in athletes. Mandibular body fractures are often associated with additional mandibular fractures. The treatment goal is to achieve preinjury occlusion and facial appearance, and this can be done via a closed reduction and maxillomandibular fixation or open reduction and fixation with or without maxillomandibular fixation. The authors present 3 cases in this article.
Key points
- •
Mandibular body fractures are often accompanied by secondary mandible fractures.
- •
A plain film radiograph may be sufficient for diagnosis of a mandibular body or symphysis fracture; however, a computed tomography scan allows for appreciation of 3-dimensional relationships and has become the gold standard at most institutions.
- •
Mandibular body fractures often require open reduction and fixation due to the physiologic forces of mastication.
- •
Understanding the location of the inferior alveolar nerve is critical in the surgical management of mandibular body fractures.
Introduction
In the United States, the most common causes of mandible fractures are interpersonal violence or motor violence crashes. Athletic injuries, falls, neoplasms, radiation-related necrosis, and iatrogenic injury are other causes of mandibular body fractures. Most frequently, mandible fractures occur in men in the third decade of life. The incidence of facial fractures from sports has decreased over time due to improved safety measures such as helmets, safety visors, and mouth guards. Sports injuries account for anywhere between 3% and 29% of all facial injuries and between 10% and 42% of all facial fractures. The most contact-heavy sports, such as football, soccer, hockey, and baseball are most frequently involved in sport-related facial injuries. Most of these facial injuries are severe enough to require some form of operative intervention, with open reduction and internal fixation in 50%.
Location of mandible fractures vary depending on the mechanism of injury. In large studies of urban populations, the angle was most affected (36%) followed by the body (21%–24%). , Patterns of mandible fractures depend on the mechanism of trauma and direction of inflicted force. Mandibular body, condyle, and subcondylar fractures more commonly result from falls and motor vehicle accidents causing anterior-posterior force. Angle and ramus fractures tend to occur from lateral force such as during assault. Mandibular body fractures also commonly occur in edentulous patients.
Definitions
- •
Mandible body: region of the mandible from the canine line to a line coinciding to the anterior border of the masseter muscle
- •
Mental foramen: bony foramen that exists halfway between the superior and inferior borders of the mandible, inferior to the second premolar
- •
Mental nerve: terminal branch of the inferior alveolar nerve, a branch of the third division of the trigeminal nerve
Anatomy
The mandible is a U-shaped structure that frequently fractures in multiple locations although single fracture sites may occur. Mandibular trauma often accompanies other facial fractures or closed-head injuries. The mandible consists of the condyle, coronoid process, ramus, angle, body, and symphysis, as shown in Fig. 1 . In this article, the authors focus on fractures of the mandibular body. The body of the mandible encompasses bone from the canine or incisive fossa to the angle of the mandible and contains the molars and premolars.
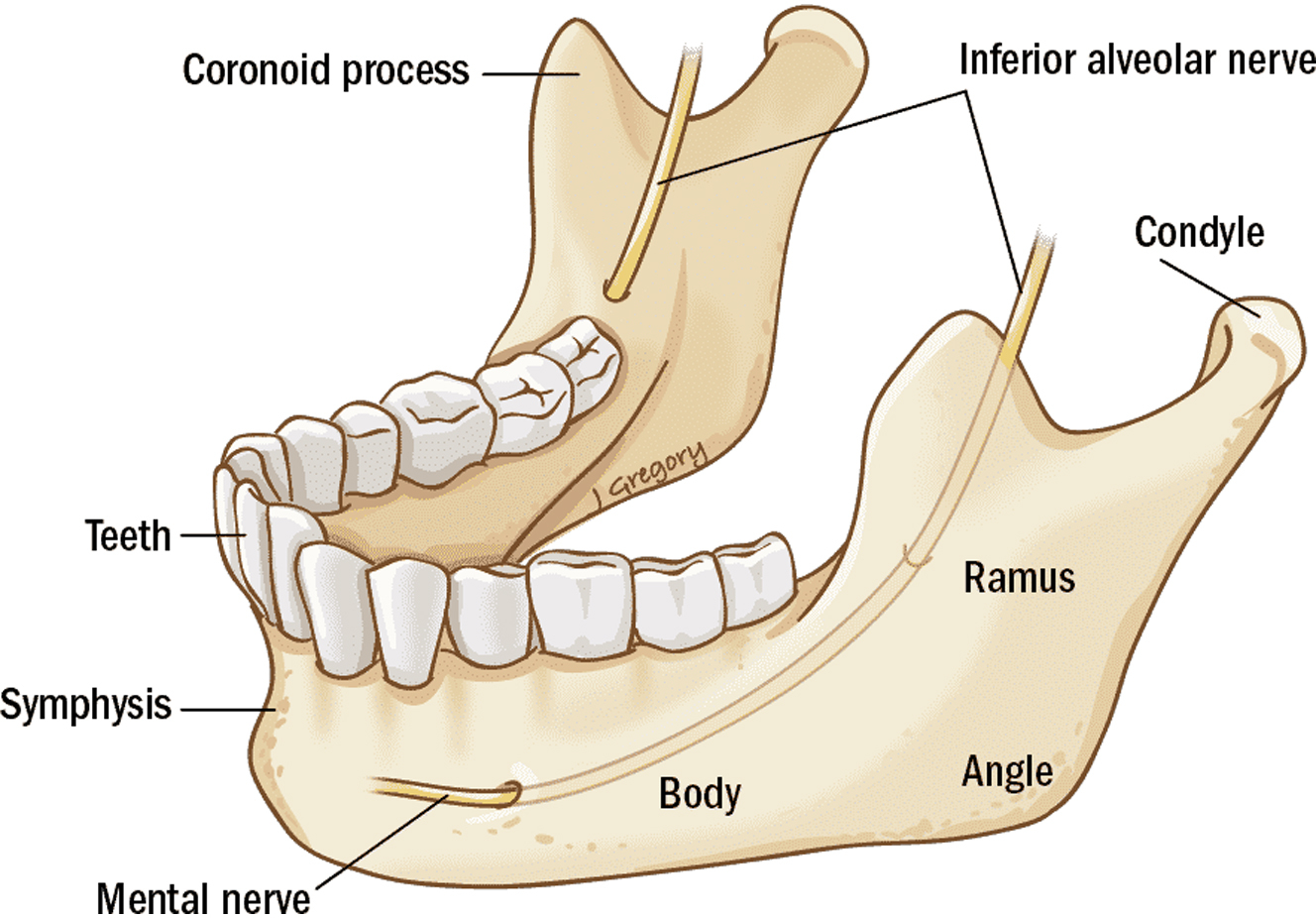
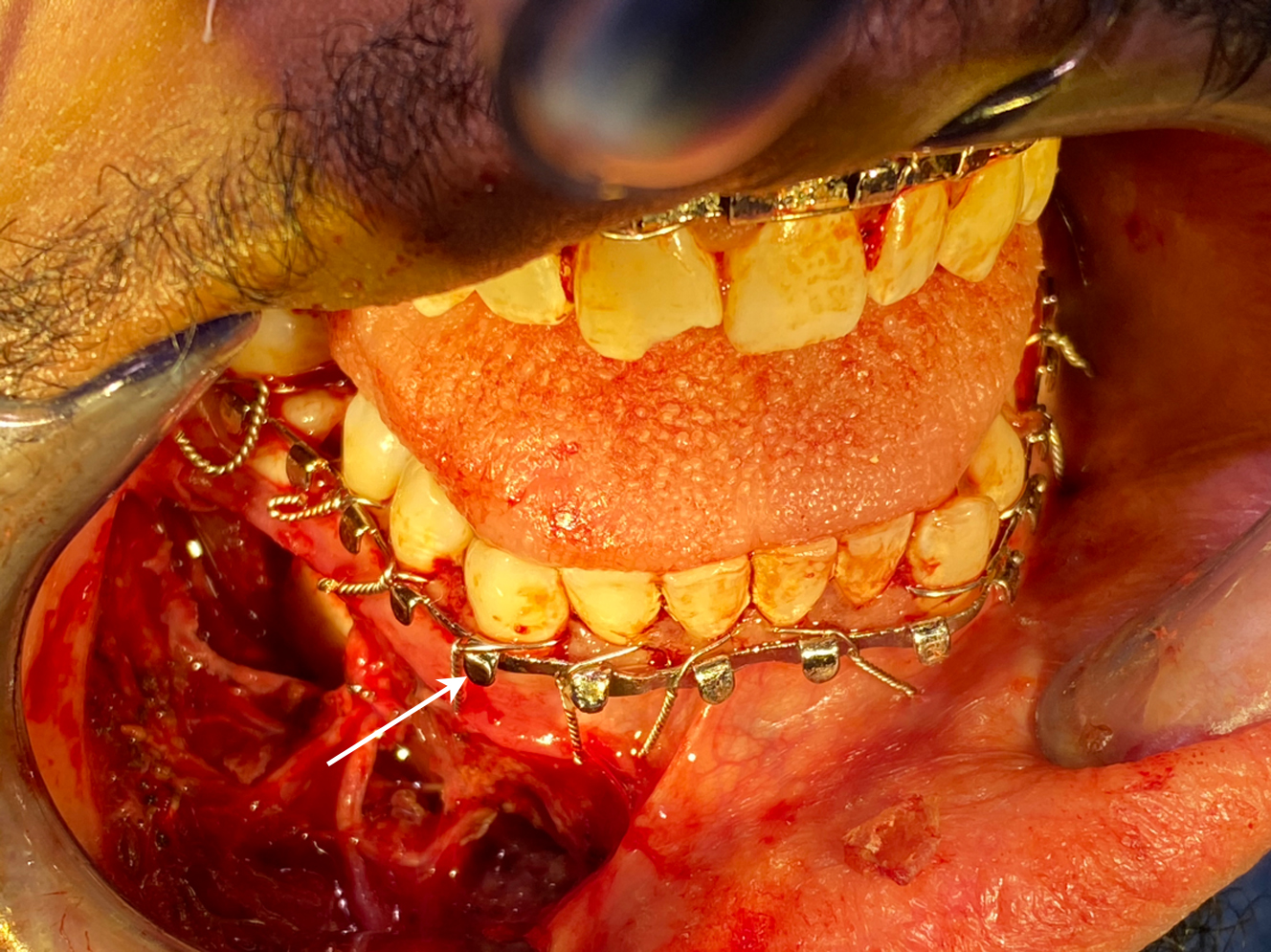
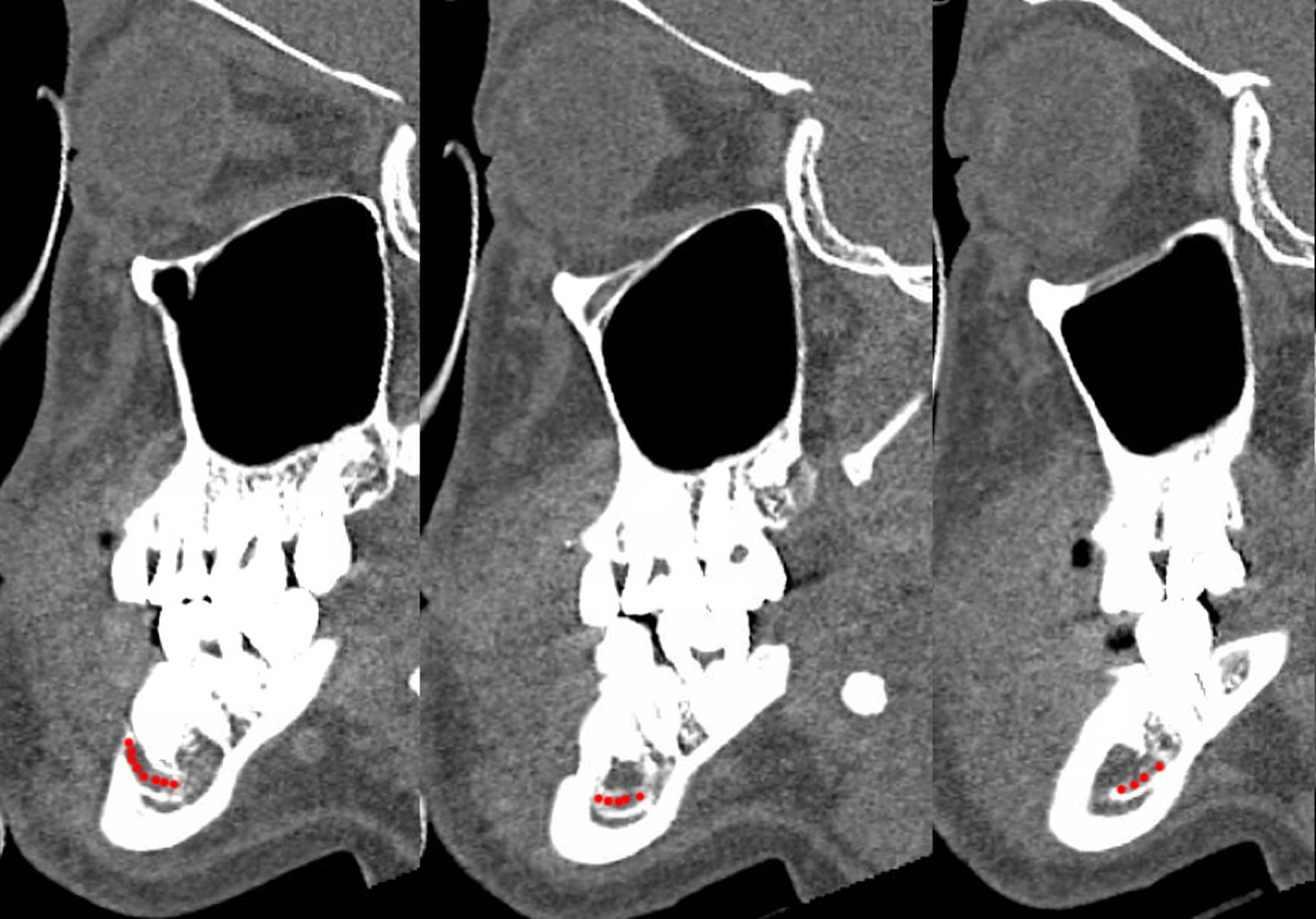
The mandibular body also contains the inferior alveolar nerve (IAN), a branch of the third division of the trigeminal nerve (V3). The IAN enters via the mandibular foramen on the lingual surface of the ramus and travels inferiorly and anteriorly within the bone, exiting via the mental foramen. The mental foramen is located at the level or just anterior to the second premolar ( Fig. 2 ). Just before exiting the mental foramen, the nerve will ascend superiorly. Thus, the level of the IAN as it runs through the mandibular body is inferior to the level of the mental foramen ( Fig. 3 ). The mental nerve divides into several branches innervating the chin, lower lip, and gingiva as it exists the mental foramen. In edentulous patients, the IAN position may shift superiorly as the dentoalveolar bone degenerates.
Evaluation
Initial evaluation of all trauma patients should be according to Advanced Trauma Life Support protocols. Airway management should be determined on a case-by-case basis. Unstable fracture segments, bilateral mandible fractures, complex midfacial fractures, and/or poor neurologic status often necessitate intubation or surgical airway. Identification and management of other associated injuries (particularly neurologic and ophthalmologic) is crucial to determining timing of surgery, as facial fracture repair is rarely urgent.
Mandibular fracture evaluation should include a comprehensive history and head and neck examination. These patients typically present with a history of facial trauma. Mechanism of injury, prior facial injuries or craniofacial surgeries, and past medical history should be assessed. The patient may report pain, swelling, malocclusion, displaced teeth, facial numbness, trismus, and/or bleeding from skin lacerations or intraoral lacerations. Lower lip anesthesia, paresthesia, or hypoesthesia may suggest injury to the inferior alveolar or mental nerve. Malocclusion is a sign of displaced mandibular or maxillary fractures, dental trauma, or temporomandibular joint disruption. As many patients do not possess perfect occlusion before injury, interviewing the patient regarding their premorbid versus postinjury occlusion and history of orthognathic treatment is critical.
Physical examination often begins with an evaluation of external and internal lacerations. Mandible body fractures involving teeth or gingiva are technically open mandible fractures. Completing a comprehensive head and neck examination helps identify additional craniofacial injuries. A complete cranial nerve examination should be performed with particular focus on lower lip and chin sensation. Gentle palpation of the mandible may identify areas of tenderness, step-offs, and bony mobility, indicating fracture instability. Maximal interincisal distance should be evaluated to assess for trismus. Normal interincisal distance varies depending on age, body habitus, and sex and is a minimum of 30 to 40 mm. In the setting of mandible fracture, trismus is typically secondary to muscle spasm and pain and resolves with anesthetic agents. In rare cases, a bony restriction may result in a physical block limiting transoral airway management. Bilateral mandibular body fractures can cause airway obstruction if an unstable central mandible fragment produces posterior tongue prolapse. Emergent intervention may include anterior traction on the tongue to support the airway before definitive airway management.
Preoperative occlusal evaluation should note loose or avulsed dentition. Missing dentition that are not accounted for warrant chest imaging to exclude airway foreign body. The patient is asked to bite down into their best occlusion. Originally developed for orthodontic treatment, Angle’s classification is one method of describing occlusion ( Table 1 ). In the setting of mandibular fractures, Angle’s classification may differ from side to side and does not comprehensively describe posttraumatic occlusion. Areas of early contact or open bite should be noted and correlated with the radiographic fracture pattern. Wear facets on the teeth may offer clues to preinjury occlusion.
| Angle’s Classification | Description |
|---|---|
| Class 1 | Ideal occlusion Mesiobuccal cusp of maxillary first molar rests in buccal groove of mandibular first molar |
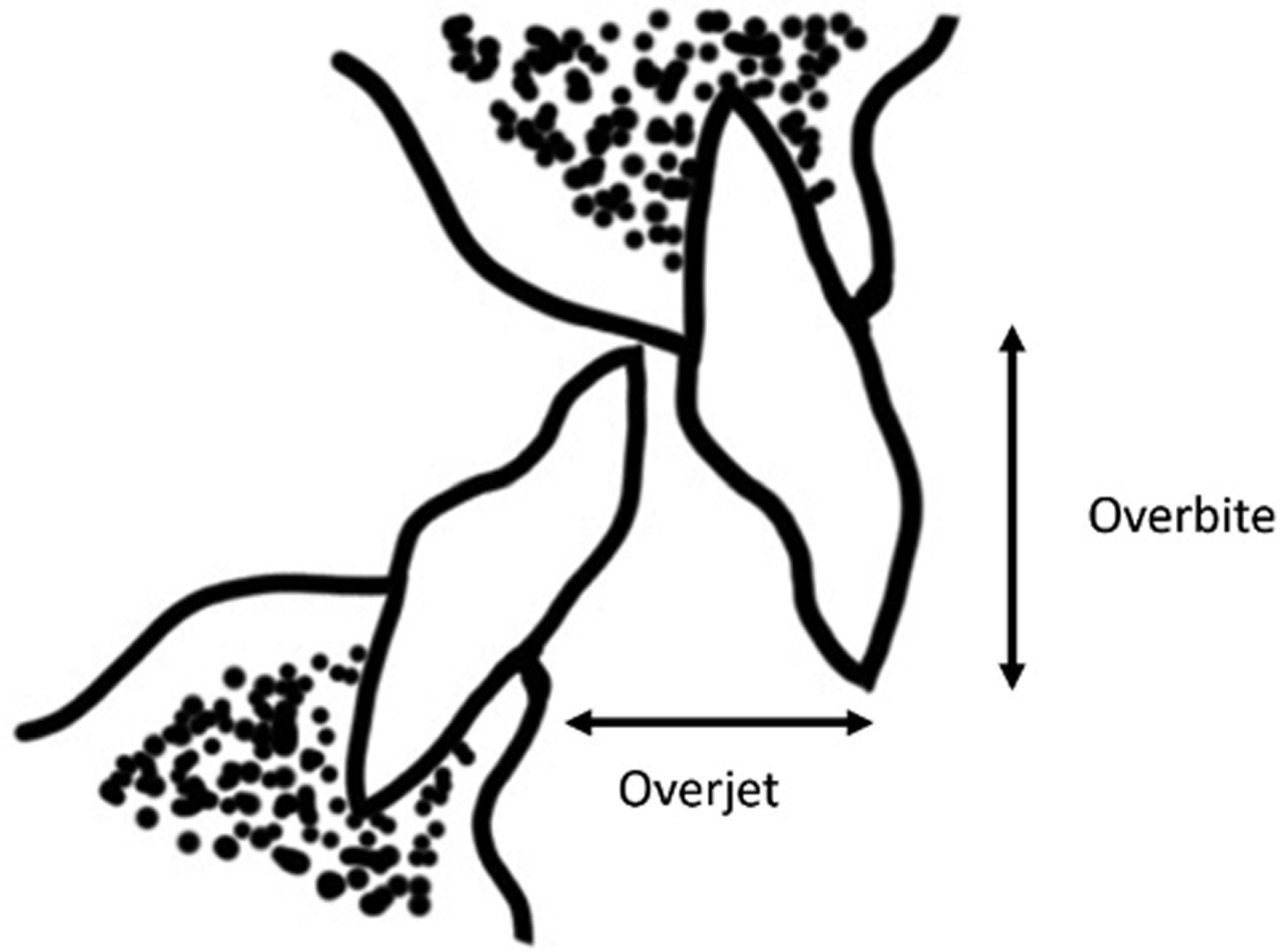
| Class 2 | Mesiobuccal cusp of maxillary first molar rests anterior to buccal groove of mandibular first molar. Division 1: incisor overjet or labial flaring of teeth: horizontal overlap from lateral surface of lower incisor to labial surface of upper incisor, parallel to the occlusal plane when in occlusion ( Fig. 4 ). Division 2: incisors are palatally flared, resulting in less overjet and more normal-appearing dental relationship anteriorly. |
| Class 3 | Mesiobuccal cusp of maxillary first molar rests posterior to buccal groove of mandibular first molar. |
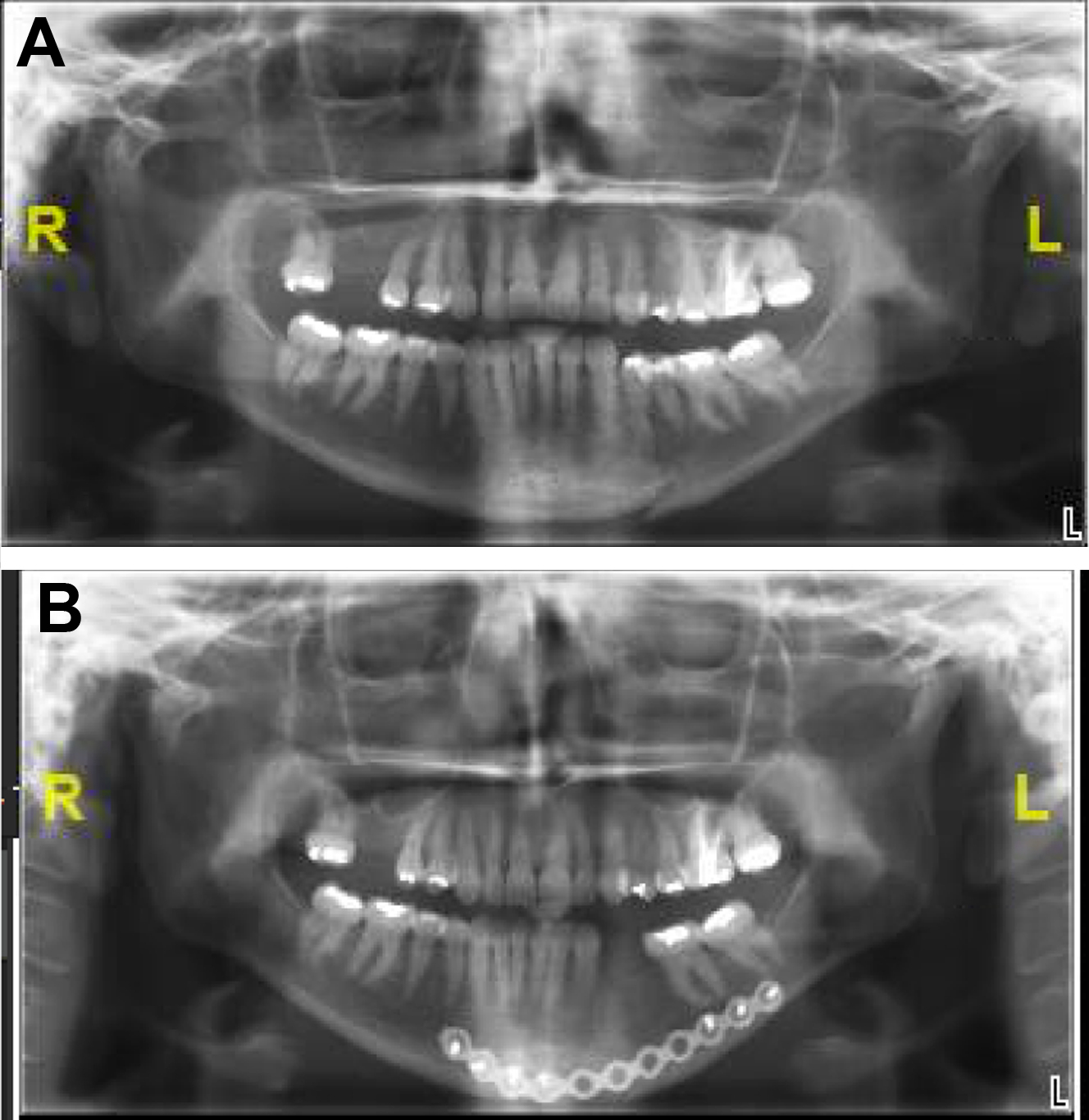
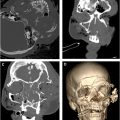
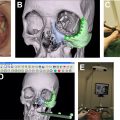
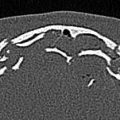
The gold standard for identification and evaluation of mandible fractures is a maxillofacial computed tomography (CT) with cuts at 1 mm or less. Three-dimensional reconstruction of CT scans facilitates understanding of geometric relationships and fracture fragment orientation. However, minimally displaced or hairline fractures may be missed due to volume averaging. The axial, coronal, and sagittal cuts should be carefully evaluated for every patient. Panoramic tomography (eg, panorex) may be used for evaluation of mandible fractures and involves lower cost and radiation exposure. Some surgeons may routinely use this modality of imaging, particularly for postoperative assessment of plating ( Fig. 5 ). However, the lack of 3-dimensional relationships makes appreciation of fracture angulation difficult. CT has higher sensitivity in fracture identification and decreased interpretation error.