Although frontal sinus fractures are relatively uncommon, the potential for long-term morbidity is significant. Management strategies remain controversial due to a lack of strong clinical evidence. Despite a paucity of strong literature, a logical treatment algorithm is presented based on the structural integrity of three anatomic parameters: anterior table, frontal sinus outflow tract, and the posterior table/dura. The literature supports a paradigm shift from open surgical management to a more conservative treatment algorithm emphasizing observation and minimally invasive endoscopic techniques. Long-term follow-up for complex frontal sinus injuries is critical
Key points
- •
A lack of clinic evidence results in continued controversy over optimal treatment strategies for frontal sinus fractures.
- •
Despite a paucity of evidence, logical and effective treatment decisions can be made based on the structural integrity of three anatomic parameters: anterior table, frontal sinus outflow tract, and the posterior table/dura.
- •
The literature supports a paradigm shift from aggressive, open surgical management to a more conservative treatment algorithm emphasizing observation and minimally invasive endoscopic techniques.
- •
Long-term follow-up for complex frontal sinus injuries is critical.
Introduction
The frontal sinus is protected by the thick cortical bone, making frontal sinus fractures relatively uncommon. However, the potential for long-term sequelae is significant, and a comprehensive treatment strategy is critical. Management of these injuries remains controversial, but most authors agree that management should include treatment of intracranial injuries, avoidance of long-term complications, reestablishment of the frontal bone contour, and return of sinus function whenever possible. This chapter provides a comprehensive, evidence-based algorithm for management of these injuries in the endoscopic era.
Anatomy and epidemiology
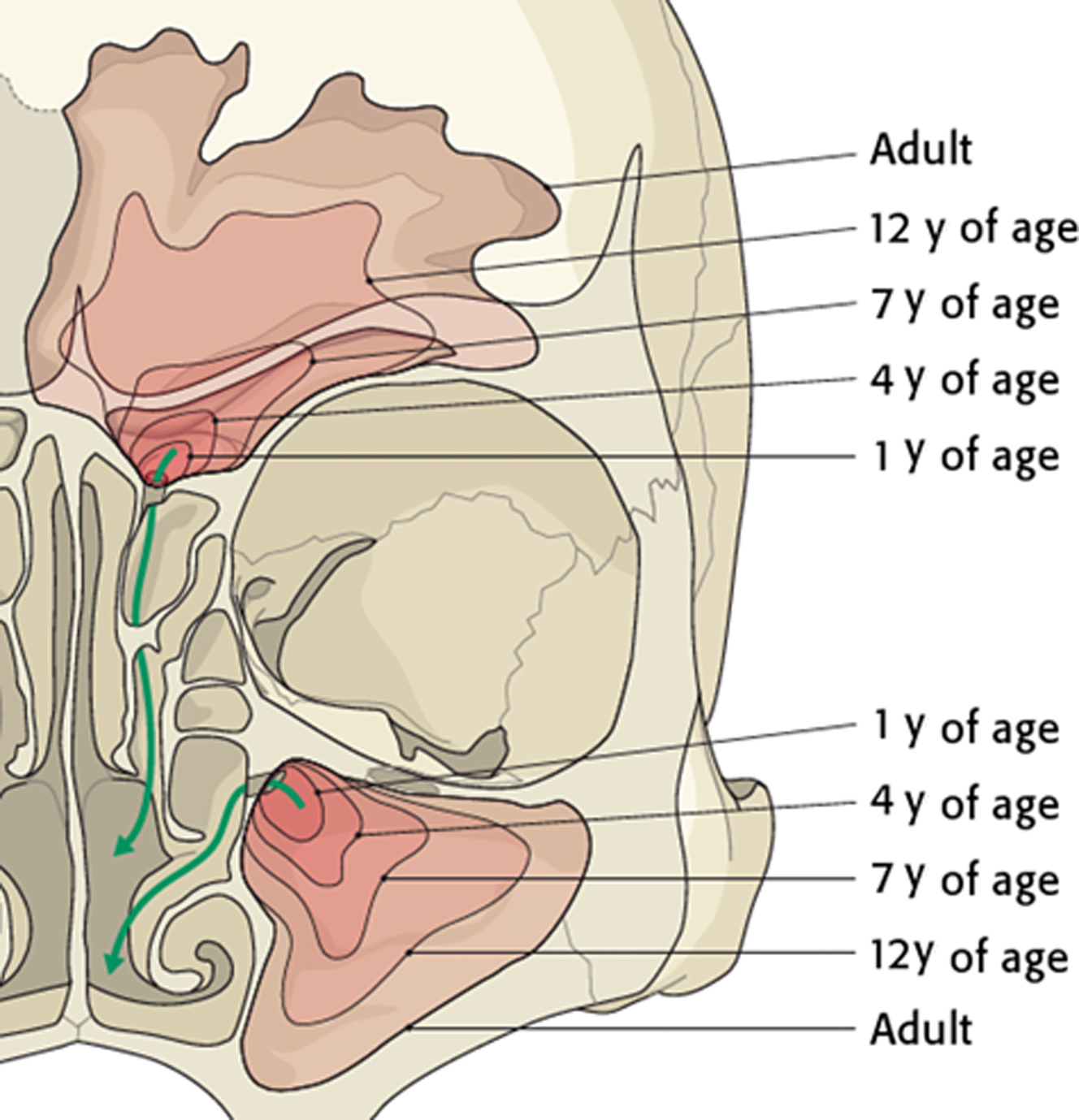
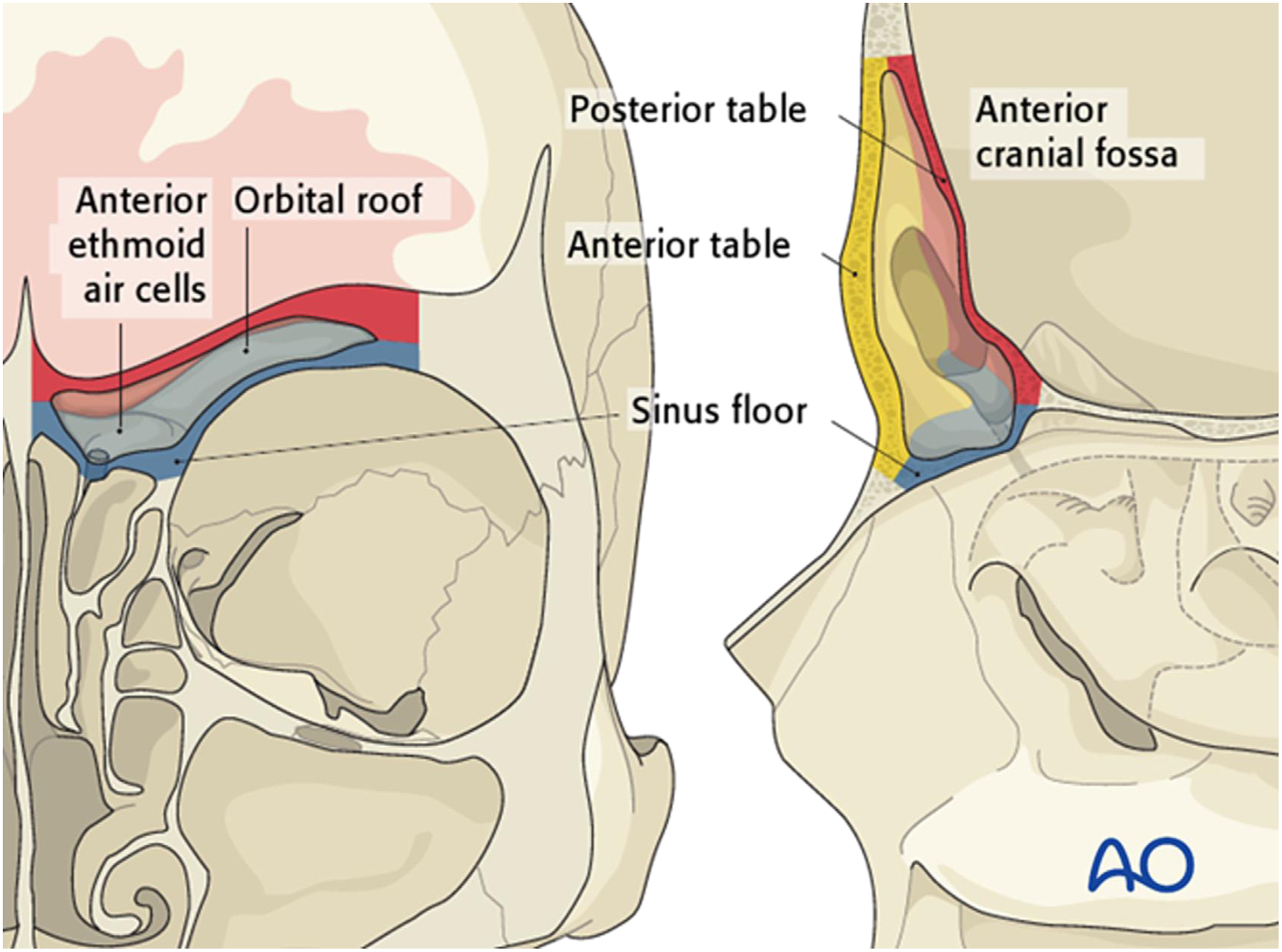
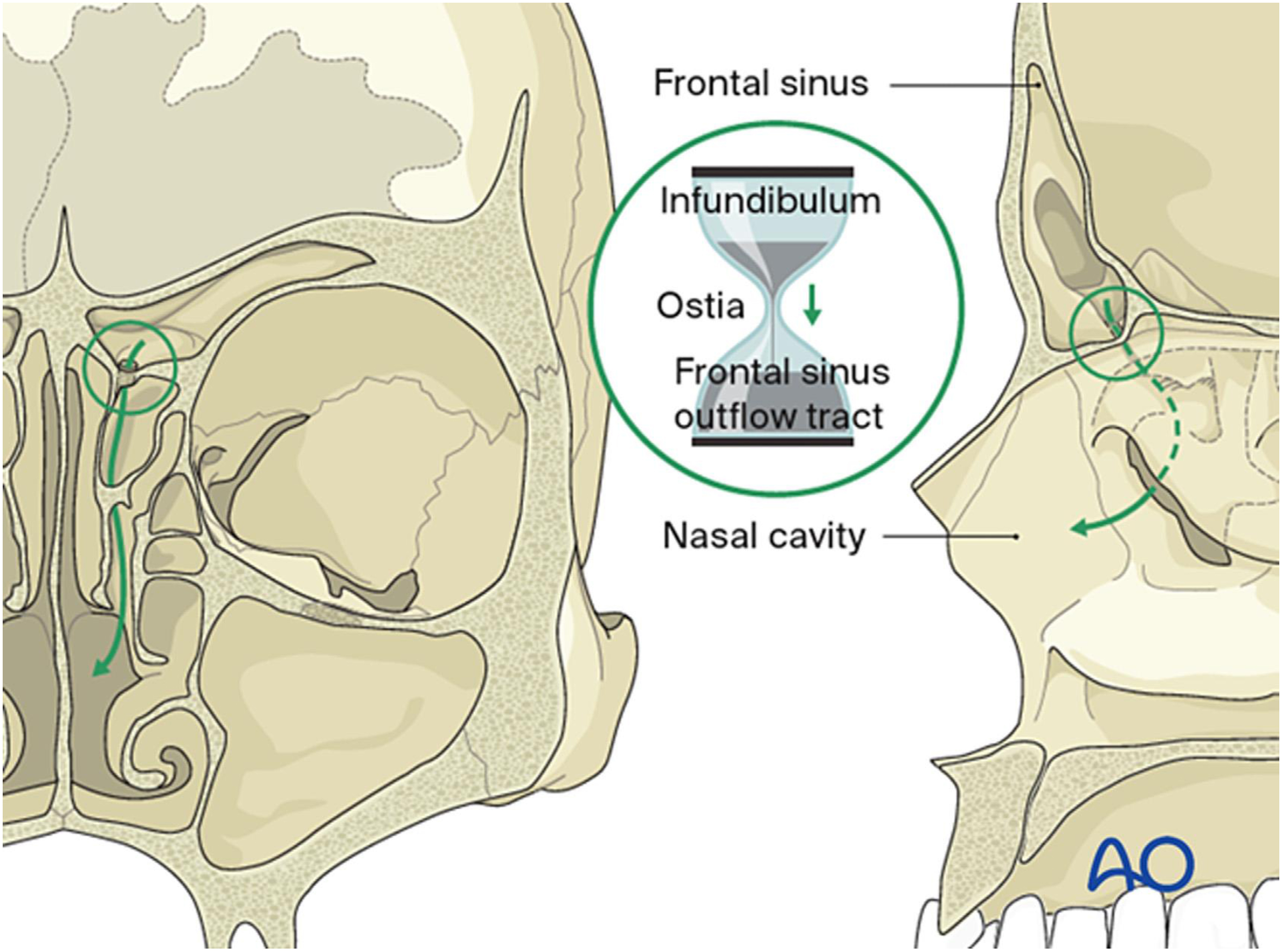
The frontal sinus is absent at birth. A rudimentary cavity develops by 1 to 2 years of age, and it achieves adult size during adolescence ( Fig. 1 ). The anterior table is very thick (up to 12 mm), and the posterior table is thin (often < 1 mm). The frontal sinus outflow tract (FSOT) has an “hourglass” shape, with the narrowest portion being 1 to 3 mm in diameter ( Fig. 2 ). Familiarity with the three-dimensional anatomy of the sinus and surrounding structures (orbital roof, anterior cranial fossa, FSOT, forehead/glabella) is critical to appropriate diagnosis and treatment of these injuries ( Fig. 3 ).
Frontal sinus fractures account for 5% to 15% of traumatic maxillofacial injuries and are usually the result of high energy trauma. Motor vehicle accidents and assaults account for the majority of these injuries. Severe “through-and-through” injuries with violation of the anterior cranial fossa have trended downward with the introduction of seat belts and air bags. , Isolated anterior table fractures account for 33% of injuries, while combined anterior/posterior table and/or FSOT fractures account for 67% of fractures. Isolated posterior table injuries are uncommon.
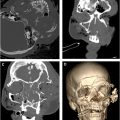
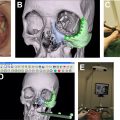
A thorough head and neck examination is essential with particular attention to the orbits, naso–orbito–ethmoid region, zygomaticomaxillary complex, and potential cerebrospinal fluid (CSF) leaks. Physical examination findings may include abrasions/lacerations, forehead contour irregularities, hematoma, tenderness, epistaxis, and clear rhinorrhea. Initial imaging should include fine-cut (∼1 mm) computed tomography (CT). 3D reconstructions are helpful for surgical planning when there is significant comminution or displacement of fracture fragments. If a CSF leak is suspected, a beta-2-transferrin assay should be obtained. It has excellent sensitivity (99%) and specificity (97%) but does take several days to process.
Treatment algorithm
Historically, frontal sinus fractures have been managed with large, open surgical approaches. The introduction of high-resolution CT and advanced transnasal endoscopic surgical techniques has ushered in a significant paradigm shift toward observation and minimally invasive treatment. An appropriate treatment strategy for frontal sinus fractures can be determined by evaluating the structural integrity of three anatomic parameters: (1) anterior table, (2) frontal sinus outflow tract, and (3) posterior table/dura. These findings can then be applied to the treatment algorithm presented in Fig. 4 .
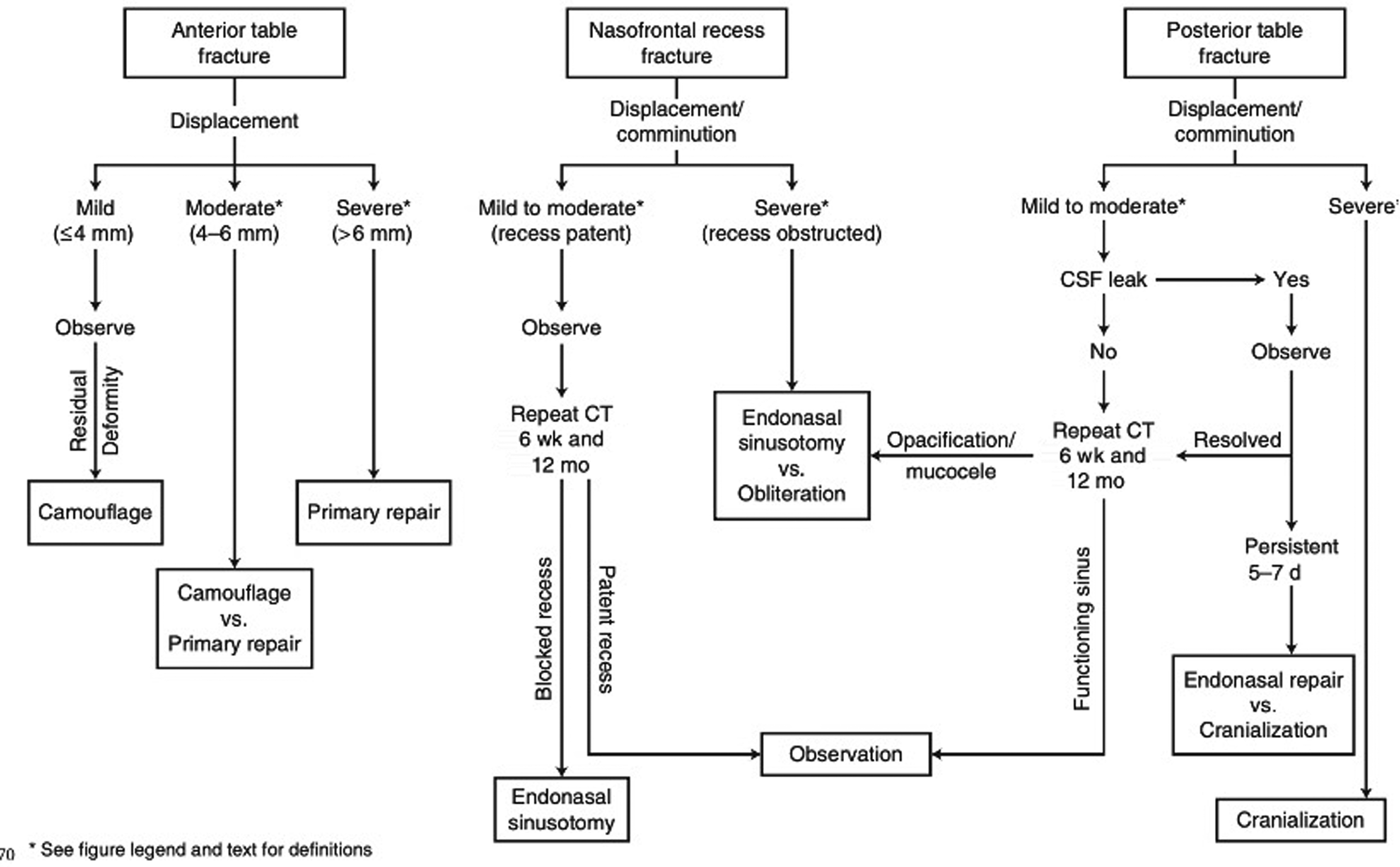
Anterior table fractures
The authors divide these injuries into three groups ( Fig. 4 ):
Mild: ≤4 mm displacement
Moderate: 4 to 6 mm displacement, moderate fracture area, with mild comminution
Severe: greater than 6 mm displacement, large fracture area with severe comminution
These anatomic parameters are used to select between 3 treatment strategies: observation, primary repair, and secondary camouflage . Surgical management is indicated when the risk of a contour deformity outweighs the risk of iatrogenic injury (ie, scaring, alopecia, paresthesia, etc).
Observation
Mucocele formation with isolated anterior table fractures is uncommon, and observation is appropriate for many of these injuries. The authors observe “mild ” and less severe “moderate ” fractures with close follow-up (see Fig. 4 ). A very small percentage may develop a contour deformity which can be corrected with a secondary camouflage procedure (see below). The goal of this approach is to avoid unnecessary surgery, while offering those few patients who need treatment a procedure that is equally efficacious to primary repair. The literature supports this conservative approach. In a series of 51 patients who underwent nonoperative management, Kim and colleagues demonstrated that no patients with fracture displacement < 4 mm developed late forehead contour deformity at a mean follow-up of 18 months. Similarly, Dalla Torre and colleagues reported on 91 patients with fracture displacement ranging from 0 to 5 mm. Only 4 patients developed a frontal contour deformity, and none of the patients elected for secondary correction.
Secondary Camouflage
The authors use secondary camouflage for patients found to have an esthetic deformity after observation or who present with an anterior table esthetic deformity. Secondary camouflage is very effective for patients with anterior table contour deformities that are completely healed. The authors most often use an endoscopic brow lift approach; however, mid-forehead (through a rhytid or laceration) and upper blepharoplasty approaches can be equally effective.
Endoscopic repair
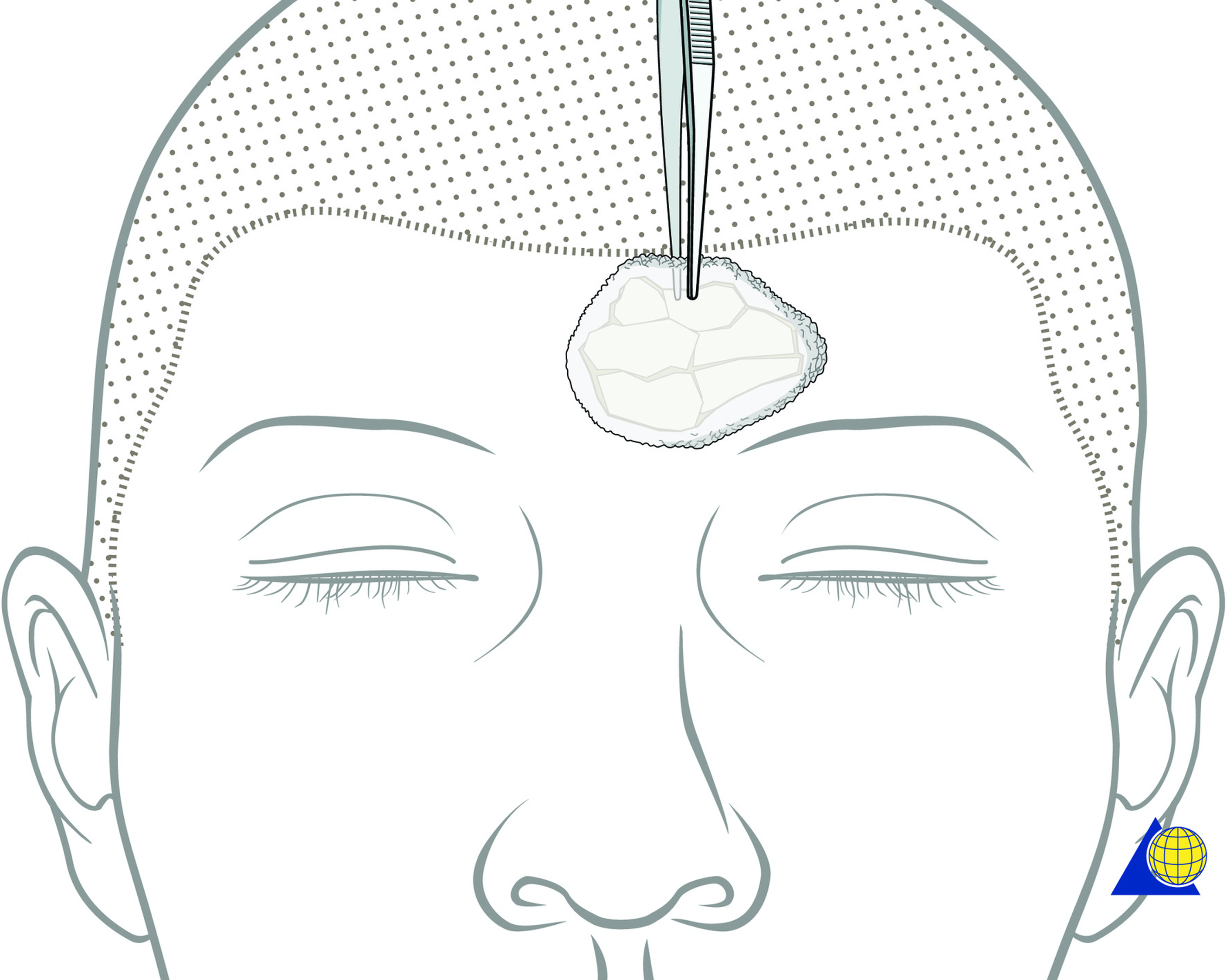
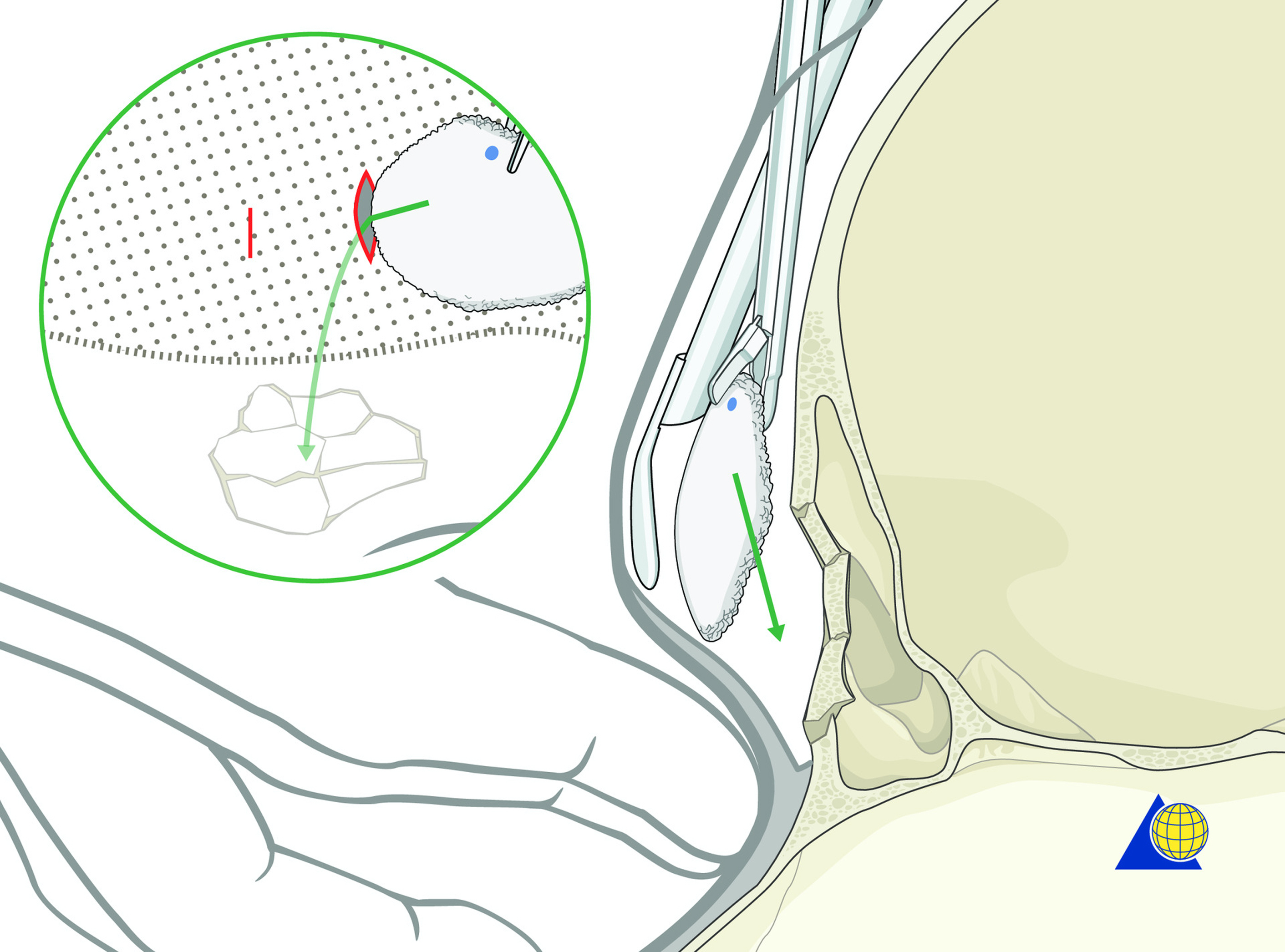
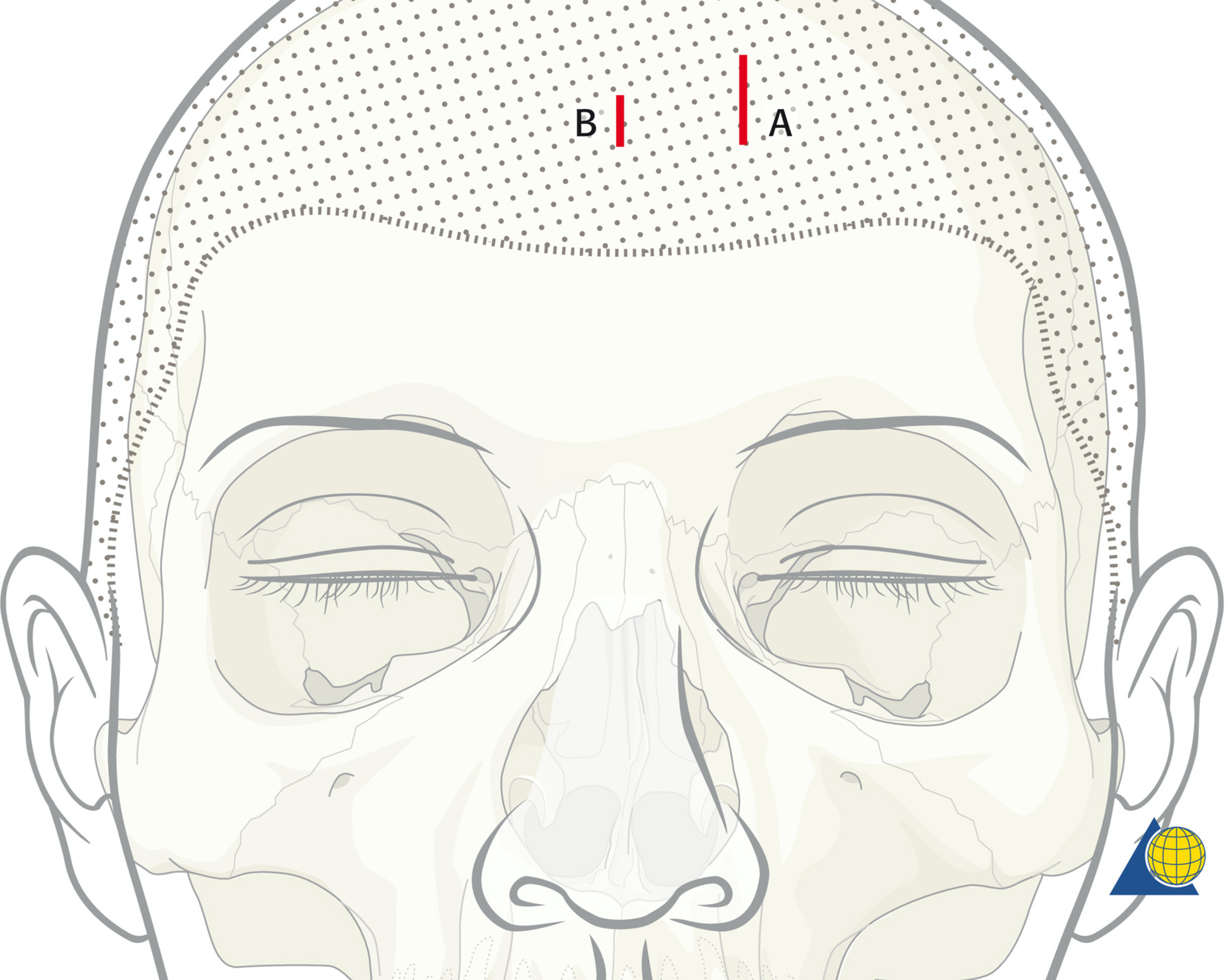
A 3 to 5 cm parasagittal “working” incision is placed 3 cm posterior to the hairline and in line with the fracture ( Fig. 5 ). A 1-2 cm “endoscope” incision is then placed at the same height, 6 cm medial to the working incision. Incisions may be moved toward the hairline for patients with receding hairlines. A subperiosteal dissection is performed with an endoscopic brow lift elevator. Dissection is performed without the endoscope and guided by palpation. Avoid tearing the periosteum, as it will help to maintain the optical cavity. After the deformity is exposed, a 4.0 mm 30-degree endoscope with rigid endosheath is inserted through the endoscope incision. A suture can be applied transcutaneously to tent the forehead skin/periosteum upward, optimizing the optical cavity ( Fig. 6 ).

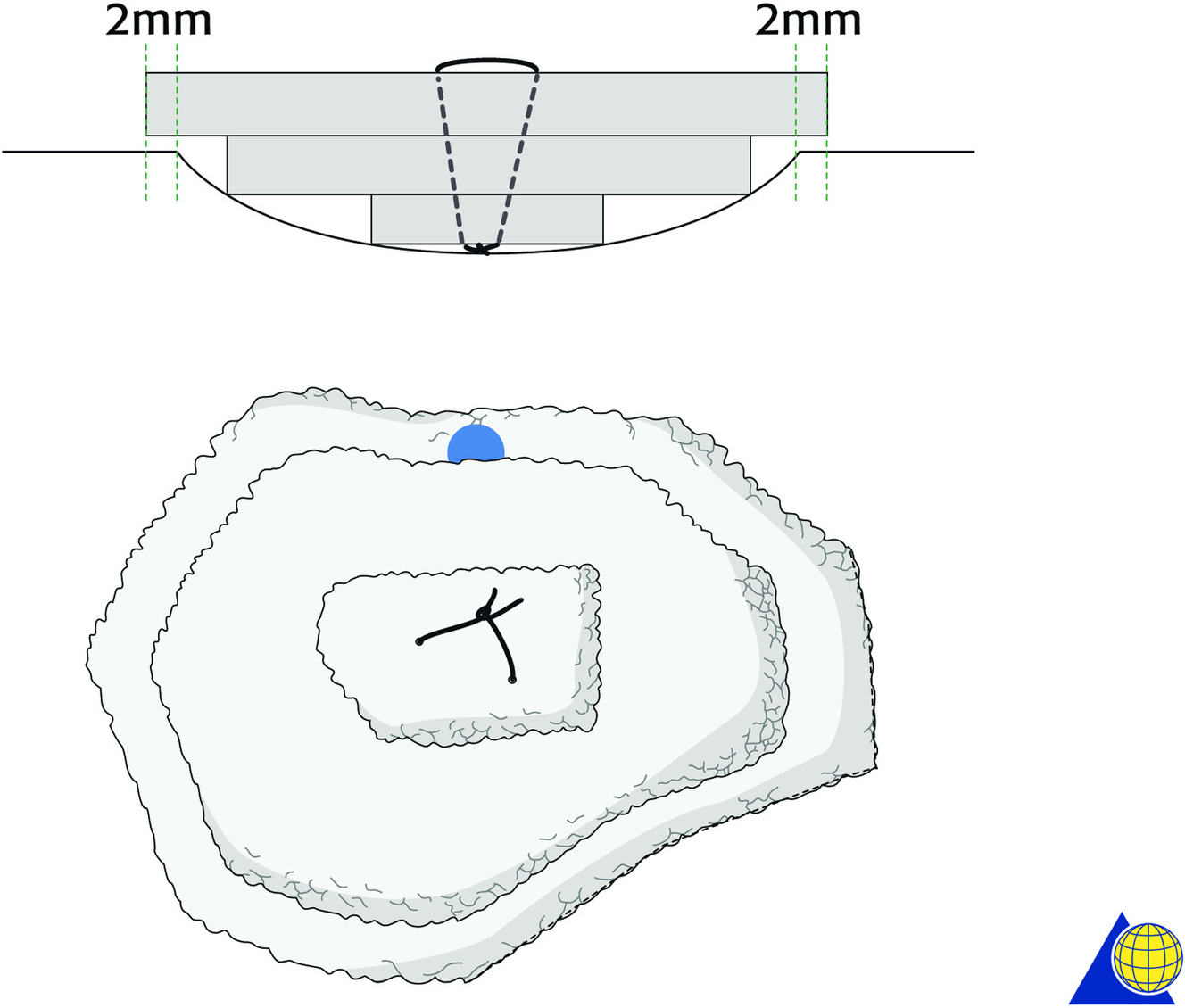
Porous polyethylene sheeting (0.85 mm) is used for reconstruction. Titanium mesh should be avoided because the sharp edges make it very challenging to insert and manipulate. The implant is trimmed to cover the defect ( Fig. 7 ). The implant is inserted through the working incision and manipulated over the defect using both internal instrumentation and external palpation ( Fig. 8 ). The superior aspect of the implant is marked with a pen to maintain endoscopic orientation. The implant often needs to be modified after initial placement to optimize shape and contour. For deeper defects, it can be sutured in 2 to 3 layers forming an inverted pyramid ( Fig. 9 ). Once the final implant is in place, a 25-gauge needle is passed through the skin and visualized endoscopically to determine optimal screw placement (ie, where multiple screws can be placed through a single incision). An 11 blade is used to make a 2 mm stab incision, and a 4-7 mm self-drilling screw is used to secure the screw through the implant at the periphery of the fracture ( Fig. 10 ). Caution should be used to avoid losing screws as they pass through the soft tissue. Patient-specific implants also work very well ( Fig. 11 ), avoiding the need for intraoperative contouring and reducing operative time. They are, however, significantly more expensive.