Le Fort fractures occur at uniform weak areas in the midface often due to blunt impact to the face. Sporting injuries are a common cause of facial trauma; however, use of protective equipment has reduced the number of sports-related injuries. All patients with traumatic injuries should be evaluated using Advanced Trauma Life Support protocol. Le Fort fractures can contribute to airway obstruction, and urgent intubation may be indicated. Surgery is indicated for most displaced Le Fort fractures to restore function and facial harmony. To facilitate reduction, the original occlusive relationship should be restored by placing the patient in MMF.
Key points
- •
Le Fort fractures occur at uniform weak areas in the midface often due to a blunt impact to the face.
- •
Sporting injuries are a common cause of facial trauma; however, use of protective equipment has reduced the number of sports-related craniofacial injuries.
- •
Le Fort fractures can contribute to airway obstruction and urgent intubation may be indicated.
- •
Surgery is indicated for most displaced Le Fort fractures to restore function and facial harmony. Good exposure is critical. The patient is placed in maxillomandibular fixation (MMF) to facilitate reduction and establish the original occlusive relationship. The sequence of fracture repair is variable.
Introduction
Le Fort level fractures are complex facial fractures that are differentiated as I, II, and III based on fracture patterns. The location of the injury, velocity and energy transfer at impact, and patient-related factors determine the fracture severity and pattern. Le Fort fractures typically occur due to blunt impact to the midface. Motor vehicle accidents (MVAs), interpersonal violence, industrial accidents, falls, and sports-related injuries are common mechanisms of injury. Sporting injuries account for 10% to 42% of all facial fractures, with midface fractures accounting for a large percentage of these injuries. , In recent years, there has been a rise in craniofacial injuries related to motor scooters with the introduction of electronic scooters to many cities. Studies noted significant bony injury to the midface with these fractures.
Facial fractures due to sporting injuries are generally less severe than those caused by MVAs and are associated with shorter hospitalization time. Le Fort level fractures are more common in high-velocity sports such as mountain biking or skiing. Sporting fracture mechanisms typically include player–player collisions and impact from equipment such as a ball–face impact with improper protective equipment. , This chapter reviews pertinent anatomy, initial patient workup, and principles of surgical repair with an emphasis on Le Fort pattern fractures related to sports.
Preventing Injuries with Protective Equipment
The use of protective equipment in sports such as helmets, facemasks, and intraoral mouthguards has significantly reduced the number of craniofacial injuries. , Although traditional helmets have been shown to reduce cranial injuries, they leave the mid and lower face unprotected. Studies are needed to determine if helmets with an extension to cover the lower jaw reduce the prevalence of mid and lower facial injuries. One study found that baseball players using faceguards were 35% less likely to suffer facial injuries than nonusers. Mouthguards may act as impact absorption devices which distribute energy from a traumatic blow in order to prevent direct force on oral structures and reduce trauma from mandible and maxilla contact. Recent increases in craniofacial trauma due to motor scooter use have been associated with noncompliance with the safety requirements and to lack of head and facial safety equipment. ,
Anatomic Considerations
The maxilla, a critical part of the human viscerocranium, is formed by the fusion of two pyramid-shaped maxillary bones at the palatine process. This fusion creates the main horizontal buttress of the face. The development of the maxilla provides support to the orbit, houses the maxillary sinus and maxillary dentition, and creates a “crumple zone” as kinetic energy in blunt force trauma is passed through the skeleton protecting the brain and neurocranium posteriorly.
The maxilla consists of the maxillary body and the frontal, zygomatic, palatine and alveolar processes. Energy delivered upon impact to the maxilla will transfer through the bone to the pyriform rim, zygoma, and pterygoid plates. These vertical buttresses absorb and distribute masticatory forces from the teeth to the skull base. There are three paired vertical buttresses: nasomaxillary (medial), zygomaticomaxillary (lateral), and pterygomaxillary (posterior). A fourth, single buttress, the nasal septum, exists at the midline ( Fig. 1 B). Although the vertical buttresses provide support and structure, they are susceptible to damage from transverse forces. The vertical buttresses are reinforced by three horizontal buttresses: the superior and inferior orbital rims and the alveolar ridge. The pterygoid plates provide posterior support to the maxilla.
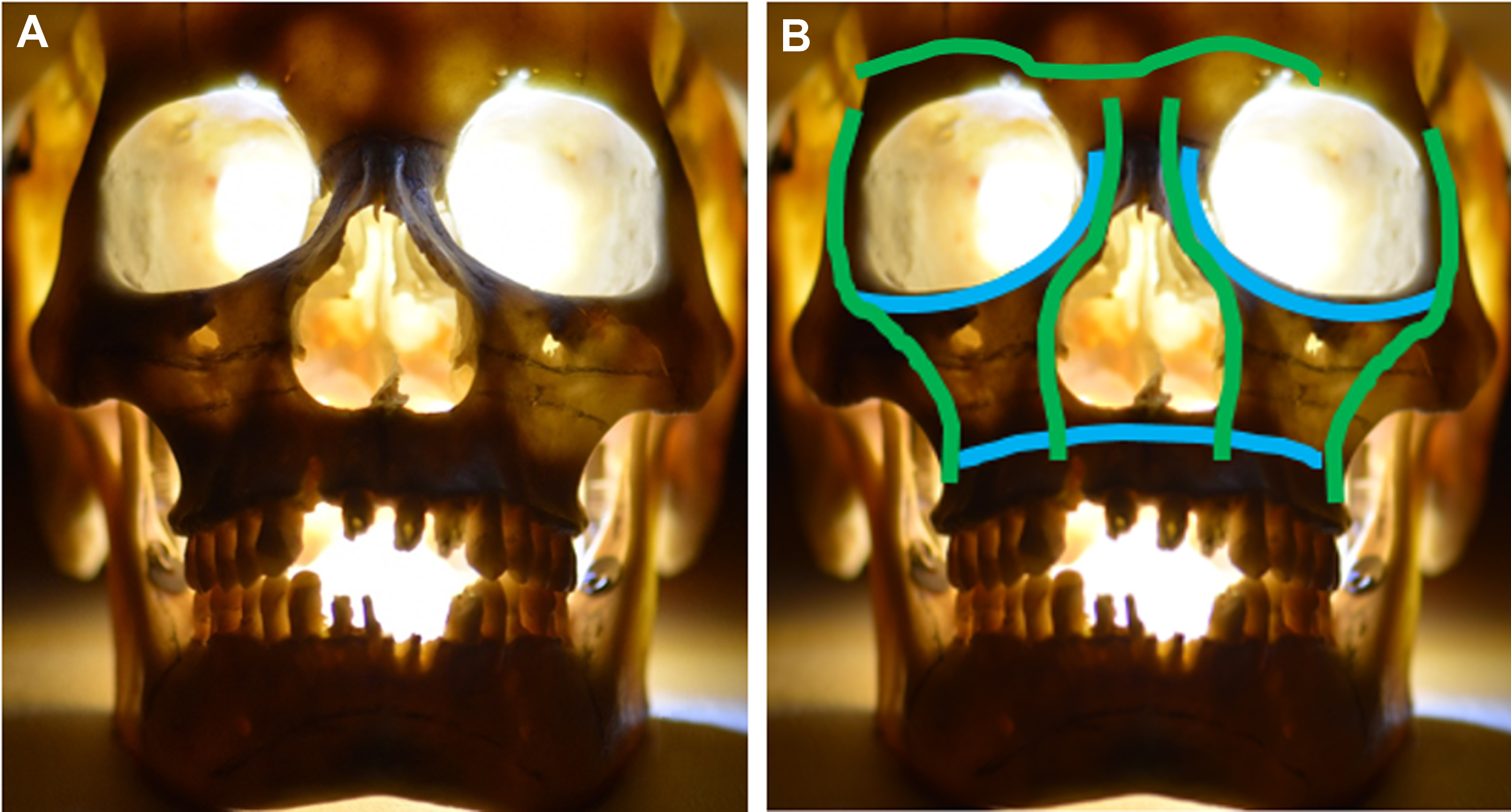
This complicated developmental conjugation of the midface creates uniform weak areas prone to fractures in specific patterns (see Fig. 1 A). These patterns were initially classified by René Le Fort in 1901 with a classification system that is still used today. Le Fort fractures are described as either unilateral or bilateral.
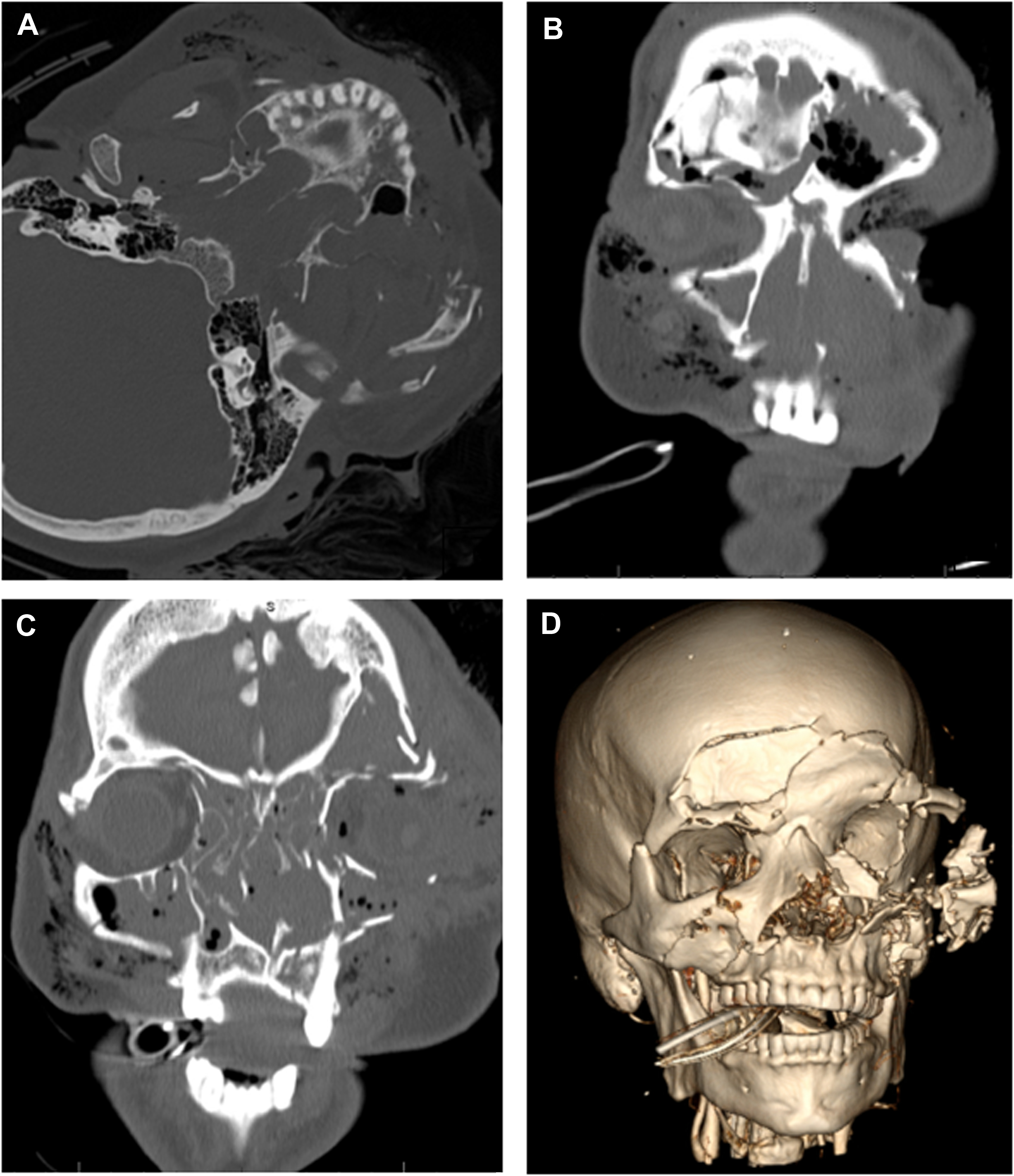
Le Fort I fracture lines are superficial to the alveolar ridge and create a separation through the maxillary sinus wall horizontally with disjunction of the maxilla from the pterygoid plate ( Fig. 2 B). Le Fort II fractures are pyramid-shaped central midface fractures that include extension superiomedially through the nasal bones, nasal process of the frontal bone or nasion, medial orbital walls, and inferior orbital rim (see Fig. 2 C). Le Fort III fractures result in complete disjunction of the maxilla from the skull base due to a transverse fracture extending from the pterygoid plate superiorly to the zygomaticofrontal suture, horizontally through the orbit to the nasofrontal suture (see Figs. 2 A, B). These are the most severe type of Le Fort fractures and carry additional risk of blindness secondary to the fracture extension near the optic nerve.
Initial Evaluation
All patients who present to the hospital with traumatic injuries should be evaluated using Advanced Trauma Life Support (ATLS) protocol. The primary goals of the ATLS protocol include securing a stable airway, supporting ventilation, evaluating circulation, identifying and controlling life-threatening hemorrhage, obtaining a baseline neurologic evaluation, and exposing the patient to evaluate for injuries. Life-threatening injuries, including intracranial, spinal, and visceral injuries, require urgent attention. Le Fort fractures can contribute to airway obstruction secondary to hemorrhage, posterior inferior displacement of the maxilla, oropharyngeal edema, and hematoma. , As many as 31% of patients with Le Fort fractures require intubation or tracheotomy due to airway obstruction or acute respiratory failure. Cervical spine instability/injury must also be taken into consideration. Standardized clinical and radiographic protocols should be implemented for workup and management of cervical spine injury. Intubation with a fiberoptic scope may be indicated. In rare instances, blunt cerebrovascular injury (BCVI) can occur with high impact craniomaxillofacial injuries. Computed tomography angiography is the recommended imaging modality to evaluate for these injuries. Plain X-ray films are mostly historical and inadequate to evaluate midfacial fractures.
Once the patient has been stabilized and initial survey is complete a complete history and physical examination should be obtained. History of present illness can be challenging to obtain. It is critical to use all available resources including previous hospital records, first responder accounts of the trauma scene, and family/witnesses. Understanding the mechanism of injury, including the vector and severity of the force, can help predict the involved structures. Mechanism of injury can also provide extremely valuable information about the cleanliness of the wound and potential for foreign bodies. The patient’s history can further direct additional workup which can be lifesaving.
Midface edema and ecchymosis are common with midface trauma and can make evaluation for facial symmetry and bony step-offs challenging. Evaluation for midface mobility can be accomplished by stabilizing the cranium while grasping the maxillary alveolar ridge. Intubation can make evaluation of the stability of the maxilla challenging as tube holding devices can stabilize the teeth and fracture. Anterior open bite malocclusion may indicate displacement of the maxillary segment due to caudal pull by the medial pterygoid muscles. The palate should be examined via direct visualization and palpation to identify palatal fractures and lacerations. Palatal fractures can create maxillary width discrepancies that present as a crossbite when the patient is brought into occlusion. Additionally, large palatal lacerations should be identified as typical repair of the Le Fort fractures includes access to the midface via the maxillary vestibule. This access, along with separation of the septum, and possible laceration of the descending palatine arteries creates a situation where the ascending pharyngeal artery is the sole blood supply of the maxilla. Failure to recognize lacerations in this area before surgical access could predispose patients to avascular necrosis. The clinician should inspect for missing or loose teeth and tooth sockets. Any missing teeth with evidence of avulsion should be accounted for. If unable to account for missing teeth, then it is recommended to review computerized tomography (CT) imaging of the face to evaluate for teeth dislodged to other areas. Additionally, an AP chest X-ray is recommended to confirm that there was no aspiration during the injury. A comprehensive ophthalmologic examination should be performed especially in Le Fort II-III type fracture patterns. In addition, evaluation for cerebrospinal fluid leak should also be included when midface fractures occur jointly with skull base injuries.
Diagnostic Imaging
The excellent resolution of CT and the availability of three-dimensional (3D) reconstruction have made CT scanning the method of choice for evaluating complex facial fractures. With current technology, fine-cut CT is a largely preferred modality as this will provide detail necessary to fully visualize the complexity of the trauma and provide enough data to use 3D imaging and 3D printing technology if desired. The ideal resolution is <0.1 mm which can be achieved by modern cone beam computed tomography imaging; hospital CTs should routinely be able to provide <1 mm slices which is acceptable. Vertical and horizontal structures are viewed best on axial and coronal views, respectively. A methodical and thorough evaluation is important in order to accurately diagnose midface fractures. MRI may be used to evaluate soft tissue, intracranial, and vascular injuries, but it has limited usefulness in evaluating skeletal injuries. Imaging of the brain and cervical spine and neck vessels should be performed to evaluate for BCVI with CTA. This is critical for severe injuries or when involvement of vessels is suspected.
Surgical Indications
Surgery is indicated for a majority of displaced Le Fort fractures, especially those that impact form and/or function. Nondisplaced and minimally displaced fractures that do not affect function and/or cause facial disharmony can be managed conservatively with or without protective devices. Goals of fracture repair include restoration of occlusion secondary to maligned maxilla or restricted mandibular movement because of coronoid process impingement. Surgical repair can also facilitate a clean, stable, well-approximated midface skeleton which is critical for bony union. , , The restoration of preinjury facial harmony is an indication for surgery. In the athlete, an important goal is typically safe and timely return to play; the need for open or closed surgical intervention can impact when an athlete can return to competition.
Indications for closed surgical treatment, such as maxillary mandibular fixation, include nondisplaced, nonmobile fractures in reliable patients who can follow-up for monitoring. Closed surgical treatment often minimizes pain and facilitates return to preinjury occlusion during the healing period. Open surgical treatment, also known as open reduction and internal fixation, is indicated for complex fractures that result in malocclusion, disruption of facial harmony, and are associated with neurologic complication such as visual disturbances and cerebrospinal fluid leakage. In general, open reduction requires longer downtime compared with closed approaches.
Surgical Approach: Airway
When possible, nasotracheal intubation is ideal, as it optimizes exposure and allows for establishment of premorbid occlusion following maxillomandibular fixation (MMF). Retromolar and submental intubations are alternatives to nasotracheal intubation that allow occlusion to be evaluated intraoperatively. In the event of significant skull base injuries, severe facial deformities, anticipated prolonged intubation, or expected multiple returns to the operating room, tracheotomy may be preferred.
Surgical Approach: Exposure
Good exposure is critical for a successful repair. All fractures should be visible before stabilization. Access can sometimes be accomplished through existing facial lacerations. The entire anterior maxilla including the zygomaticomaxillary buttress, the infraorbital foramen and nerve, orbital rim, and piriform aperture can be accessed through a maxillary vestibular incision. This incision alone is often adequate for Le Fort level I injuries. A coronal incision may be required in more extensive fracture cases and readily provides exposure of the nasal root and supraorbital rims. The incision can be extended to access the zygomatic arch and bilateral zygomas if necessary. Limited access to the zygomaticofrontal suture can be obtained with a lateral brow or upper blepharoplasty incision. The orbital floor and infraorbital rim can also be accessed via a transconjunctival, subciliary, or infraorbital skin incision.
Surgical Approach: Sequence of Approach and Repair
Once exposure is optimized, the fracture site should be cleaned extensively. Removal of blood products, tissue, and foreign material not only will allow for better adaptation of the bony segments but also will improve the environment for bone healing. Following exposure and cleaning, the bone is ready for reduction under direct visualization. To facilitate reduction in Le Fort fractures, the original occlusive relationship should be restored by placing the patient in MMF. MMF can be established with interdental wiring, intermaxillary fixation screws, conventional arch bars, hybrid arch bars, ivy loops, or using bonded orthodontic hardware.
In these cases, it is imperative that the operative surgeon mobilizes the maxilla to allow for passive seating of the patient into a stable and repeatable occlusal relationship. Using existing wear facets or comparing current occlusion to preoperative photographs can help. It is important to work with the anesthesiologist during this stage of the surgery. The midface is highly vascular, and control of bleeding is often not possible until osteotomies are performed and segments are replaced. Movement of the maxilla, including down fracture, is associated with the highest incidence of bleeding in these cases. In a study of Le Fort I patients, the mean estimated intraoperative blood loss was 945 mL, with 50% of cases reporting greater than 1000 mL. Permissive hypotension can reduce some of the blood loss but should be used with caution in older and medically complex patients. Additionally, muscle paralysis is critical when establishing occlusion as muscle pull can inadvertently create occlusal discrepancies. In cases with unusual premorbid occlusal patterns, segmental fractures of the maxilla, or difficulty establishing intraoperative occlusion, fabrication of an occlusal splint is recommended.
In edentulous patients, if establishment of MMF is desired, it is necessary to use a gunning splint. This can be specifically made for the patient. Alternatively, existing dentures can be modified to accept screws or wire fixation to the jaw and can help establish an appropriate vertical dimension to guide operative efforts if open repair is essential. In addition, osteotomies may be necessary to mobilize the midface when fractures are incomplete or unusual. Palatal fractures generally reduce well once establishing proper occlusion. Palatal fractures can easily be plated on the anterior surface of the maxilla superior/between the tooth roots. The operative surgeon should strongly consider alternative options to creating additional cuts on the palatal mucosa or implanting hardware on the palatal bone. Once the fracture is reduced and the occlusion reestablished, the surgeon can select a fixation technique that allows for stabilization of the bones and realignment of the segments. For uncomplicated fractures, L-shaped plates at the zygomaticomaxillary buttress and piriform rim should allow for adequate fixation and will be positioned in the best bone stock available to hold the hardware.
The sequence of the approach is surgeon specific, and multiple approaches have been described. The senior author prefers working from the periphery to the center to transform a Le Fort III fracture into a Le Fort II and subsequently into a Le Fort I fracture. This approach of reducing Le Fort fractures from complex to simple allows for an orderly repair of the midface and reestablishes both midface height and width. First, frontal fractures are repaired creating a solid frontal bar. Next, the bizygomatic width must be reconstructed. When the frontal bone is intact and the zygomatic arches are continuous, the midfacial height and bitemporal width are reestablished by repairing the zygomaticofrontal suture. By stabilizing the zygoma to the frontal and temporal bones, a Le Fort III fracture has been reduced to a Le Fort II fracture. Next, the nasofrontal area is repaired, thereby reducing the Le Fort II component and converting it to a Le Fort I fracture.
Virtual Planning and Intraoperative Imaging
There are many challenges when it comes to repairing Le Fort level facial trauma. First, there is the complexity of facial anatomy and importance of restoring function and structure to the facial skeleton with the primary goals being to restore occlusion and obtain bony union which will facilitate proper mastication and speech and minimize pain. Visualizing 3D relationships from a two-dimensional image is a challenge, especially in regions with complex 3D anatomy. It can be difficult to directly view the deep facial skeleton from esthetic incision lines, and it can therefore be difficult to visually assess the intraoperative result for ideal projection and position. Additionally, edema limits evaluation of symmetry. Use of preoperative and intraoperative imaging can help address some of these challenges. With the availability of intraoral scanners, 3D images of the teeth can be obtained and fused with CT imaging. This surface-generated image is not distorted by dental materials like images obtained using ionizing radiation. This allows for more accurate representation of the dentition and occlusion and permits accurate fabrication of planned surgical splints that can recreate a planned occlusion intraoperatively. Image-guided simulation with use of 3D CT allows for preoperative analysis and manipulation of images as part of a comprehensive surgical planning session. Surgeons can then manipulate the fractured segments while observing the effect on reference anatomic structures, compare the fractures to “standard anatomy” or unaffected sides, and create micromovements which are easily reproducible in vivo. Although 3D reconstruction of scans can provide an important tool for the operative surgeon, it is critical that the images be evaluated carefully in the nonreformatted views. Volume averaging in the 3D reconstruction can underestimate fractures and may mislead a surgical team. Nevertheless, surgeons report a subjective preference for viewing images in 3D, and one study shows improved diagnostic accuracy with 3D CT scans.
Another useful tool is intraoperative imaging which allows the surgeon to evaluate the repair in the operating room and make adjustments in real time. This is most useful when positioning fracture segments, grafts, or hardware near vital structures like the optic nerve. Postoperative CT is considered the gold standard for the evaluation of surgical outcomes, but errors identified with this approach would require return to the operating room. New technology allows for more mobile CT scans with rapid processing time and low radiation exposure making intraoperative imaging more realistic. Although the majority of Le Fort fractures are easily visualized with standard surgical approaches and using the as low as reasonably achievable standard for diagnostic imaging and radiation, intraoperative CT can be an extremely useful intraoperative tool when used correctly in limited situations. This technology is increasingly available in operating rooms. The mean total operating time is minimal, and the use of intraoperative CT often results in intraoperative revisions. It is not clear how this relates to patient outcomes, but ultimately, addressing malposition or insufficient reductions intraoperatively results in decreased complication and reoperation rates.
Return to Play
Evidence-based research to establish return-to-play guidelines is limited. Recovery periods of up to 6 weeks have been reported in literature with some advocating return to activity at 3 weeks with graduated participation until 6 weeks. , Professional athletes are under significant pressure to return to play in a timely manner, but this must be weighted carefully in terms of possibility of reinjury and need for healing from the initial event. Loss of play time can negatively impact position in team and loss of salary. Early return with insufficient time for recover is associated with high risk of another impact to the injured site. The use of sports-orthosis or protective equipment can provide psychological reassurance and may prevent reinjury, but research on the efficacy of these devices is lacking. These advantages must be weighed against their shortcomings, such as obstructing sight, being hot, and uncomfortable, and, in some sports, the appearance of these devices has been not accepted by athletes. The appropriate time to return to play is likely athlete, injury, and sport specific. Sports more prone to repeat injury such as boxing would likely require longer convalescence than sporting with lower contact risk.
Clinics care points
- •
Le Fort fractures typically occur due to blunt impact to the midface
- •
Sporting injuries accounts for 10% to 42% of all facial fractures
- •
Le Fort level fractures are more common in high-velocity sports
- •
Use of protective equipment reduces the number of craniofacial injuries ,
- •
The midface has uniform weak areas which are prone to fracturing in specific patterns
- •
Le Fort I fracture lines result in disjunction of the maxilla from the pterygoid plate
- •
Le Fort II fractures are pyramid-shaped central midface fractures
- •
Le Fort III fractures result in complete disjunction of the maxilla from the skull base
- •
All patients with traumatic injuries should be evaluated using the Advanced Trauma Life Support protocol
- •
Le Fort fractures can contribute to airway obstruction, and urgent intubation may be indicated
- •
Computerized tomography (CT) scanning, with resolution less than 1 mm, is the method of choice for evaluating complex facial fractures
- •
For surgical repair, nasotracheal intubation is ideal, as it optimizes exposure and allows for establishment of premorbid occlusion
- •
Surgery is indicated for most displaced Le Fort fractures
- •
Goals of fracture repair include restoration of occlusion, facial harmony, and to facilitate a clean, stable, well-approximated midface skeleton to allow for healing
- •
Good exposure is critical for a successful repair
- •
To facilitate reduction in Le Fort fractures, the original occlusive relationship should be restored by placing the patient in maxillomandibular fixation
- •
Close collaboration with the anesthesiology team is critical for establishing a safe airway, limiting blood loss and ensuring complete muscle relaxation
- •
The sequence of repair of facial fractures is surgeon specific, and multiple successful approaches have been described
- •
Intraoral scanners, three-dimensional CT, and image-guided simulation are useful as part of a comprehensive surgical planning session
- •
For complex fractures, intraoperative CT can be useful in evaluating and addressing malposition or insufficient reductions intraoperatively
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


