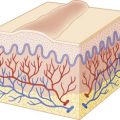
Viruses are ultramicroscopic organisms that grow only within living cells. The antigenic material responsible for viral immunologic reactions is present in the outer protein membrane (capsid) of the virus. The nucleoprotein core is composed of either deoxyribonucleic acid (DNA) or ribonucleic acid (RNA). Lacking ribosomes, viruses depend on the use of the host cells’ enzyme systems, blending with metabolic material of the host cell and often remaining undetected until some stimulus incites the production of new viral particles.
Viral infections of the skin may present with varied morphologies, including papules, vesiculobullous lesions, ulcers, and tumors. This chapter will include a discussion of herpes simplex virus (HSV) infections, herpes zoster (HZ), viral-like disorders of the oral mucosa, and warts. Some poxvirus infections will be discussed, including molluscum contagiosum (MC), cowpox, pseudocowpox (“milker’s nodules”), orf, and smallpox. Although human immunodeficiency virus (HIV) infection does not result in primary skin disease, a brief discussion of acquired immunodeficiency syndrome (AIDS) in children and its skin disease associations is included. Neonatal herpes infection is discussed in Chapter 2 .
Herpes Simplex Virus Infection
The herpesvirus family includes HSV, Epstein–Barr virus (EBV), cytomegalovirus (CMV), varicella-zoster virus (VZV), and human herpesviruses (HHV) 6 through 8. Aside from HSV, the other herpesviruses are implicated primarily in exanthematous illnesses. HSV infections are quite prevalent in both children and adults. HSV-1 and HSV-2 are double-stranded DNA viruses that primarily infect the epidermis or mucosal surfaces. After acute infection, the virus rapidly replicates and establishes latent infection in regional nerve ganglia, from which it occasionally reactivates. These viruses rely on the host-cell nucleus for DNA replication, and hence when microscopic evaluations are performed on samples with infection, the characteristic cytologic inclusions are located within the nucleus.
HSV-1 is primarily associated with oral and labial lesions and HSV-2 with anogenital lesions, although the predilection of a specific viral serotype to a particular anatomic site appears to be changing. Primary HSV-1 infection is largely a childhood disease that affects the oral mucosa, pharynx, lips, and occasionally the eyes. HSV-2 is primarily implicated in genital-tract disease, with spread occurring via sexual contact or most commonly in neonates by passage through an infected birth canal (see Chapter 2 ). Although the mucocutaneous lesions caused by HSV-1 and HSV-2 are clinically indistinguishable, differentiation between the two serotypes can be made by viral culture, Western blot serologic testing, HSV-antigen detection with monoclonal anti-HSV antibodies, or polymerase chain reaction (PCR) studies. The Tzanck smear is a rapid and cost-effective diagnostic test but is dependent on the experience of the examiner and cannot distinguish between HSV and VZV infections. Transmission of HSV is accomplished via exposure to infected mucous membranes or skin with active lesions or to mucosal secretions from an individual with active infection but can also be transmitted via exposure to secretions from an asymptomatic person who is shedding the virus.
Infection with HSV is classified as primary or recurrent. Primary infections occur in individuals without circulating antibodies and result from direct contact with infected secretions or actual mucocutaneous lesions. After an incubation of days to weeks, they may present as subclinical infection, characterized only by the development of antibodies, as a localized or generalized cutaneous eruption, or as a serious systemic infection with central nervous system or disseminated involvement. Most primary HSV infections are asymptomatic. Recurrent HSV infection occurs in individuals who were previously infected either clinically or subclinically. It is characterized by repeated episodes of mucocutaneous lesions at the same site or sites.
Topical and systemic antiviral agents commonly used to treat HSV infections are summarized in Table 15-1 .
| Drug | Formulation | Regimen | Indication/Comment |
|---|---|---|---|
| Topical | |||
| Acyclovir | 5% cream (2 g, 5 g) | Apply 5 times/day | Recurrent HL; A: ≥12 years; 4 days; Rx |
| 5% ointment (15 g, 30 g) | Apply 6 times/day | Initial GH, localized HSV; A: adults; 7 days; Rx | |
| Penciclovir | 1% cream (1.5 g, 5 g) | Apply q. 2 h (awake) | Recurrent HL; A: ≥12 years; 4 days; Rx |
| Docosanol | 10% cream (2 g) | Apply 5 times/day | HL; A: ≥12 years; treat until healed; OTC |
| Oral (all Rx) | |||
| Acyclovir | 200 mg capsule | A: ≥2 years | |
| 400 mg, 800 mg tablet | |||
| 200 mg/5 mL susp | |||
| 200 mg 5 times/day | Initial GH; 10 days | ||
| 200 mg 5 times/day | Recurrent GH; 5 days | ||
| 400 mg 2 times/day | Suppression, recurrent GH; up to 12 months, then reevaluate | ||
| Famciclovir | 125, 250, 500 mg tablet | A: ≥18 years | |
| 1500 mg single dose | Recurrent HL | ||
| 1000 mg 2 times/day | Recurrent GH; 1 day | ||
| 250 mg 2 times/day | Suppression, recurrent GH; up to 12 months | ||
| Valacyclovir | 500 mg, 1 g caplet | A: adults, and ≥12 years for HL | |
| 1 g 2 times/day | Initial GH; 10 days | ||
| 500 mg 2 times/day | Recurrent GH; 3 days | ||
| 500 mg–1 g once daily | Suppressive GH | ||
| 2 g 2 times/day | HL; 1 day; both adults and children ≥12 years | ||
* Approved indications and regimens listed; often used off-label.
Herpetic Gingivostomatitis
Herpetic gingivostomatitis most commonly occurs in children between the ages of 10 months and 5 years, although it may occur at any age. It presents with small vesicles on an erythematous base that evolve into painful, shallow gray erosions and ulcerations ( Fig. 15-1 ). The lesions most often involve the palate, tongue, and gingivae. Gingival swelling and easy bleeding may occur. Perioral lesions involving the lips, cheeks, and chin ( Fig. 15-2 ) occur in up to three-quarters of patients. Other common features include fever, drooling, eating and drinking difficulties, foul breath odor, and irritability. Cervical and submandibular lymphadenopathy is also quite common. Secondary bacteremia with group A β-hemolytic streptococci, Staphylococcus aureus, or other organisms may occasionally be a complication. Associated hepatitis has been observed, most often in neonates and immunosuppressed patients with acute primary HSV-1 infection, but also rarely in immunocompetent children.


The differential diagnosis of herpetic gingivostomatitis in a child includes herpangina, hand-foot-and-mouth disease, aphthous stomatitis, Behçet syndrome, pemphigus vulgaris, and Stevens–Johnson syndrome. The diagnosis can be confirmed by viral culture or direct fluorescent antibody studies when necessary. Although gingivostomatitis is usually caused by HSV-1, HSV-2 may cause a similar syndrome that usually occurs in adolescents and young adults who engage in oral–genital contact. Such primary HSV-2 infection results in similar symptoms of gingivostomatitis and pharyngitis, which in some patients may be difficult to differentiate from bacterial pharyngitis. Adolescents and young adults may also have primary HSV-1 gingivostomatitis.
Although herpetic gingivostomatitis tends to be self-limited over 10 days to 2 weeks, dehydration may result from poor oral intake and excessive fluid losses, especially in younger children. In some patients, hospitalization may be required for intravenous hydration and pain control. Ambulatory treatment measures include supportive therapy with fluids and use of topical analgesics, anesthetics, or coating agents, including lidocaine, diphenhydramine, milk of magnesia, Maalox, or Kaopectate. Specific antiviral therapy with acyclovir is advocated by some, seems most effective when started within 3 days of disease onset, and may reduce the number of oral lesions, prevent the development of new lesions, diminish difficulties with eating and drinking, and reduce the rates of hospitalization in young children.
Ocular Herpes Infection
Primary HSV infection of the eye can result in a severe purulent conjunctivitis with edema, erythema, and vesiculation with superficial erosion or ulceration of the cornea (epithelial keratitis). Ocular HSV infection is a leading cause of recurrent keratoconjunctivitis with associated corneal opacification and one of the chief causes of corneal blindness in the United States. This infection results from recurrent viral shedding from the trigeminal nerve reactivation and is more often caused by HSV-1. Patients with keratoconjunctivitis present with pain, photophobia, lacrimation, and eye discharge. There may also be involvement of the eyelid (blepharitis). Deeper involvement of the cornea (stromal keratitis) or anterior uvea (iritis) may occur, and both are more serious and associated with a greater risk of visual loss. Children with HSV keratitis may have poorer visual outcomes than adults, are more often misdiagnosed, and are susceptible to amblyopia. Ocular HSV infections may be unilateral or bilateral; patients with bilateral involvement tend to have a more protracted clinical course, and recurrences are more common. Bacterial superinfection of herpetic keratoconjunctivitis is common. Acute retinal necrosis has rarely been reported in children.
The diagnosis of herpetic keratoconjunctivitis can be confirmed with viral culture. Nested PCR studies, where available, seem to be superior to culture and can be performed on tear film or corneal scrapings. The immunochromatographic assay (ICGA) kit utilizes a monoclonal antibody against HSV glycoprotein D and has high specificity (but lower sensitivity) when applied to corneal scrapings. Ophthalmology referral is indicated, and treatment includes topical antiviral ophthalmic ointments or solutions and oral antiviral agents. Topical antiviral agents include trifluridine, vidarabine, and idoxuridine. In a series of 53 pediatric patients with HSV eye infections, 79% of those with keratitis had corneal scarring and 26% experienced vision impairment, highlighting the importance of prompt referral and therapy.
Herpes Labialis
Herpes labialis refers to herpetic infections occurring on the lips, most often the vermilion border. This is the most common type of recurrent herpes infection and represents the classic “cold sore.” As with other types of recurrent infection, it occurs after reactivation of latent HSV in the cells of the trigeminal ganglia. Herpes labialis often presents initially with prodromal symptoms such as tingling, burning, or itching. After 1 to 2 days the cutaneous eruption appears as a localized cluster of small vesicles or erosions on an erythematous base ( Fig. 15-3 ). Occasionally other areas of the face may be involved, and in immunocompromised individuals oral mucosal and/or severe involvement ( Fig. 15-4 ) may be noted (see below). Topical and oral antiviral agents are useful in treating herpes labialis, especially when initiated within 1-2 days of the disease onset. Prophylaxis with oral agents is advocated by many for patients with a history of multiple recurrences of herpes labialis.


Genital Herpes
Genital herpes (herpetic vulvovaginitis, herpes progenitalis) is one of the most widespread sexually transmitted diseases (STDs) in the developed world and has an increasing incidence. HSV-2 is primarily responsible for genital-tract herpetic infections, and seroprevalence studies reveal rates as high as 60% to 90% in developing countries and 20% to 22% of the general population in developed countries. The proportion of HSV-1 isolates in genital herpes is also increasing, especially in young adults and college students. Risk factors that directly correlate with HSV-2 infection include race (higher risk in African-Americans and Hispanics), age, years of sexual experience, lower family income, lower education level, number of sexual partners, and other STDs. The diagnosis of genital HSV in a child should raise the suspicion of sexual abuse. Maternal–fetal transmission of HSV may result in neonatal herpes, which is discussed in Chapter 2 .
The majority of HSV-2 infections are subclinical and go unrecognized by the host. Symptomatic primary genital herpes presents with lesions 2 to 8 days after contact with an infected individual. In distinction, first episode, nonprimary genital herpes (i.e., the initial episode of genital herpes in a host with a past history of nongenital herpes) may not present with signs or symptoms for several months. The lesions of primary genital HSV are painful vesicles clustered on an erythematous base ( Fig. 15-5 ) and distributed on the vulva, labia, vagina, perineum, penile shaft, glans penis, urethra, and less often the scrotum. In females, cervical involvement, intense soft-tissue swelling, and severe pain may be present. The vesicles rupture rapidly, leaving behind painful erosions or ulcers that may be associated with pruritus, dysuria, vaginal and urethral discharge, and tender inguinal lymphadenopathy. Pustules may occasionally be present. Systemic signs and symptoms may include fever, malaise, headache, and myalgias. Herpetic sacral radiculomyelitis with urinary or fecal retention and neuralgias may occur, as may aseptic meningitis. Less common features of HSV infection include endometritis and salpingitis in women and prostatitis in men. The symptoms of genital HSV usually improve over 5 to 7 days, and the cutaneous lesions heal over 2 to 4 weeks without therapy.

Genital herpes may show a heterogeneous clinical spectrum. Extragenital involvement may be seen, with lesions most commonly involving the buttocks, anal region, thighs, mouth, and fingers (see below). Atypical morphologies may also be present, including deep and tender ulcers, single erosions, erosive urethritis, vulvar fissure, and penile edema. A high index of suspicion must be maintained, especially in the immunocompromised host or in patients with features of other STDs. The differential diagnosis for genital herpes includes syphilis, chancroid, lymphogranuloma venereum, condylomata acuminate, Behçet syndrome, HZ, erosive candidiasis, and lichen sclerosis. Acute infection with EBV may also present with acute genital ulceration (see Chapter 16 ).
Recurrent genital HSV infection is characterized by less severe cutaneous lesions that are usually preceded by a prodrome of pain, tenderness, itching, tingling, or paresthesia. The vesicles are fewer in number, and recurrent disease may be less common with HSV-1 versus HSV-2 disease. Triggering factors for recurrent disease may include physical or emotional stress, febrile illness, and menstruation. Recurrence rates tend to be highest for the first years after the initial infection. Asymptomatic (subclinical) HSV shedding is another feature of genital herpes and among women with genital HSV-2 infection, occurs on an average of 2% of days. The risk of subclinical shedding increases with the rate of symptomatic recurrences.
The diagnosis of genital herpes can be confirmed by viral culture, Tzanck preparation (cannot distinguish between HSV-1 and HSV-2), direct fluorescent antibody testing, Western blot serologic testing, or PCR. Treatments for genital herpes include supportive care and antiviral therapy (see Table 15-1 ). Supportive measures include warm sitz baths, topical anesthetics, topical antibacterial ointments to prevent secondary infection, and oral analgesics. Education regarding the nature and risks of HSV infection and safe sex practices should be offered, and evaluation for other STDs should be considered when appropriate. An effective vaccine against HSV is highly desirable, and research toward this end is ongoing. Experimental vaccines contain recombinant glycoprotein subunits, attenuated or replication-defective virus vaccines, and those composed of plasmids expressing glycoprotein subunits. Vaccine development has been challenging given the poor understanding of the mechanisms by which host immune responses fail to control HSV.
The choice of antiviral therapy depends on the host immune status and the nature of the infection (primary or recurrent). Oral acyclovir, famciclovir, and valacyclovir may all help to speed healing, decrease symptoms, and decrease viral shedding. Long-term suppressive therapy in patients with frequent recurrences is useful in reducing both the rate and duration of flares. Although topical acyclovir ointment may offer some benefit for initial genital herpes infections, it offers little in recurrent infections.
Cutaneous Herpes and Eczema Herpeticum
Cutaneous HSV infection can occur on any body surface area. Involvement of the finger (herpetic whitlow) is discussed in the next section. Nonorolabial, nongenital involvement presents in a similar fashion, with clustered vesicles or erosions on an erythematous base ( Figs. 15-6 and 15-7 ). The lesions may be misdiagnosed as impetigo or HZ. Occasionally, recurrent cutaneous HSV may present only with prodromal symptoms followed by skin erythema and edema but without the characteristic vesiculation. In some instances, patients with recurrent cutaneous HSV may develop associated secondary bacterial infection or lymphangitis.


Eczema herpeticum (EH, or Kaposi varicelliform eruption; see Chapter 3 ) is a severe, disseminated HSV infection that occurs in individuals with atopic dermatitis or other chronic skin disease, including pemphigus, Darier disease, burns, and others. Although the etiology of EH has not been clearly established, the impaired skin barrier associated with these diseases is believed to create a more permissive environment for viral invasion and binding to cellular receptors, leading to a higher prevalence of EH with greater dermatitis severity. Despite the high prevalence of atopic dermatitis in the general population and frequent exposure to HSV, EH is quite rare, possibly relating to a requirement for multiple additional host and environmental factors. Single nucleotide polymorphisms in the interferon regulatory factor 2 ( IRF2 ) gene have been demonstrated to confer a greater risk of EH, possibly reflecting an abnormal immune response to HSV. Patients with EH usually experience an abrupt onset of fever, malaise, and a widespread eruption of monomorphous vesicles and erosions ( Figs. 15-8 and 15-9 ; see Chapter 3 , Figs. 3-28 and 3-29 ). The lesions are most prominent in areas of active dermatitis but especially tend to involve the head, neck, and trunk.


Complications of EH include keratoconjunctivitis, secondary bacterial superinfection, fluid loss, and viremia. The mainstay of treatment for EH is systemic antiviral therapy, which for the majority of patients is most appropriately administered via intravenous delivery in the hospital. Early initiation of therapy is preferable, and delays in starting acyclovir therapy appear to be associated with increased length of hospital stay. Other treatment considerations include hydration with attention to electrolyte balance, antibiotic therapy for secondary bacterial infection, and pain control. Meticulous skin care should be performed, with bland emollients applied during the early phase of barrier recovery, as well as the application of anti-inflammatory agents for the underlying dermatitis. The timing of the latter remains controversial; although some have suggested that use of topical corticosteroids during active EH may adversely affect prognosis, a review of more than 1300 children admitted for treatment revealed no increase in length of stay when these agents were started at the time of admission. Ophthalmologic evaluation is indicated when facial involvement is present. More extensive EH at presentation may be an indicator of an increased rate of repeated episodes.
Erythema multiforme (see Chapter 20 ), an acute, self-limited reactive skin disease, has been associated with HSV infection in both children and adults. In prepubertal children with erythema multiforme, especially the recurrent type, HSV DNA was detected by PCR studies on skin biopsy specimens taken from the target lesions. This finding was noted both in patients with a known history of HSV and in those without any such history. Prophylactic acyclovir may thus be useful in abrogating recurrences of erythema multiforme in children.
Herpetic Whitlow
Herpetic whitlow is a unique form of HSV infection involving the pulp of the distal phalanx (or multiple phalanges). It is seen most often in physicians, dentists, dental hygienists, and nurses who have contact with the mouth or genital regions of patients with herpetic lesions. It may also occur as a result of autoinoculation in patients with herpes labialis, herpes stomatitis, or genital herpes. The virus is inoculated onto the skin of one or more fingers, resulting in a deep-seated, painful vesicular or bullous eruption with erythema ( Fig. 15-10 ). Spontaneous resolution usually occurs over 3 weeks if the condition is left untreated. The differential diagnosis of herpetic whitlow may include blistering dactylitis, burns, and impetigo. The diagnosis is confirmed by viral culture or direct fluorescent antibody testing, and treatment with oral acyclovir or other antiviral agents may result in alleviation of pain and more rapid healing.

Herpes Gladiatorum
Herpes gladiatorum is a term used to describe a widespread primary inoculation HSV infection occurring in contact sports enthusiasts such as wrestlers or rugby players. It may occur at some time in up to one-third of wrestlers and is characterized by grouped vesicles on an erythematous base. It has also been observed after shared use of boxing gloves believed to be contaminated by HSV-1, with lesions occurring over the knuckles. The most common locations for herpes gladiatorum are the head, neck, and upper extremities. In addition to widespread cutaneous lesions, affected individuals may have fever, malaise, sore throat, anorexia, headache, weight loss, and regional lymphadenopathy. The cutaneous lesions of herpes gladiatorum may occasionally lack classic vesicles, in which case the differential diagnosis may include tinea corporis gladiatorum, impetigo, and atopic dermatitis.
Herpes gladiatorum can be effectively treated with oral acyclovir, famciclovir, or valacyclovir. The duration of therapy necessary before allowing the athlete to return to competition is controversial, and evidence-based recommendations do not exist. Sharing of equipment and towels should be discouraged and appropriate cleaning of wrestling mats encouraged. Seasonal antiviral prophylaxis has been advocated by some in an effort to suppress recurrent outbreaks and reduce the risk of spread to susceptible teammates or opponents.
Herpes in the Immunocompromised Host
Severe, chronic, and recalcitrant HSV infections may be seen in the setting of immunodeficiency. These settings include individuals with hematologic malignancy, those with a history of bone marrow or solid-organ transplantation, and those with HIV infection. Although these patients may develop common forms of HSV infection, their lesions may be more widespread and extensive. Persistent or recurrent ulcers are a common manifestation of HSV infection in patients with AIDS. Large, persistent ulcers in patients infected with HIV should arouse suspicion for HSV, although the differential diagnosis may include syphilis and chancroid. Less common locations such as the buttocks and back are also more likely to be involved in these patients. HSV lesions in immunocompromised hosts may also be verrucous, pustular, markedly crusted ( Fig. 15-11 ), necrotic ( Fig. 15-12 ), or exophytic.


In addition to cutaneous lesions, disseminated HSV may be noted in this patient population. Oropharyngeal involvement, esophagitis, tracheobronchitis, pneumonitis, hepatitis, pancreatitis, adrenal necrosis, and gastrointestinal-tract and bone marrow involvement may occur. These severe and/or disseminated infections may be caused by either HSV-1 or HSV-2.
Herpes Zoster
HZ (also called zoster or shingles ) is an acute vesicular eruption caused by reactivation of a latent infection with VZV in the sensory ganglia. Although it is most often seen in elderly or immunosuppressed individuals, it may also occur in children. Although pediatric zoster is most common in immunocompromised children or those who had a primary intrauterine infection or acute varicella within the first year of life, it may occasionally occur in children without any of these risk factors. Neonatal HZ has rarely been reported, presumably in association with exposure to varicella zoster in utero . Due to licensure of the live attenuated Oka strain varicella vaccine, it has become clear that HZ may be caused by reactivation of the latent vaccine virus, even in children. Studies of HZ incidence since implementation of the vaccination program in 1995 have yielded conflicting results, showing both increased incidence and no increase, and suggesting that there may be other unidentified risk factors for HZ that are changing over time. In a review of 322 children with HZ, the incidence in vaccinated children (either wild-type or vaccine-strain) was 79% lower than in unvaccinated children (wild-type only).
HZ is characterized by vesicles and erythema clustered in a dermatomal distribution of one or more sensory nerves ( Fig. 15-13 ). The most commonly affected dermatomes are the second cervical to second lumbar nerves (C2 to L2) and the fifth ( Fig. 15-14 ) and seventh cranial nerves. Patients often complain of hyperesthesia, pain, and tenderness to light touch in the affected area(s), usually before any cutaneous findings are present. Although the eruption is usually unilateral with a sharp demarcation at the midline, occasional contralateral involvement is seen. It is not unusual to see a few randomly scattered vesicular lesions beyond the primary dermatomal involvement, and such scattered lesions do not necessarily constitute disseminated zoster.


Successive crops of new lesions with extension of the process may occur for up to 1 week, followed by crusting of the vesicles and healing over 1 to 2 weeks. In children the disorder tends to be milder, and healing often occurs rapidly, within a few days to 1 week. In addition, in otherwise healthy children, postherpetic neuralgia (PHN, a delayed phenomenon of chronic pain and paresthesias in an area previously affected by HZ) is rare. PHN is more common in elderly patients and in those with a history of ophthalmic HZ (see below).
Immunocompromised children with HZ may have more extensive involvement with a higher risk of viremia and visceral dissemination. This may include pneumonia, encephalitis, hepatitis, and disseminated intravascular coagulopathy. These patients may also have disseminated cutaneous involvement that presents in a fashion more typical of acute varicella and with no obvious dermatomal component. The intensity of chemotherapy may affect the risk of HZ; in one series, more than half of the children with acute lymphoblastic leukemia receiving chemotherapy on high-risk protocols developed HZ during their course of treatment. Abdominal zoster refers to the presentation of HZ as severe abdominal pain that precedes the development of cutaneous lesions. These patients are often explored surgically, and the condition is associated with a high incidence of abdominal visceral involvement. Children infected with HIV may have chronic or relapsing HZ, or HZ with unusual cutaneous lesions (i.e., hyperkeratotic papules, ulcers, or necrotic plaques).
Infection associated with the ophthalmic branch of the fifth (trigeminal) nerve may involve the cornea with keratitis and uveitis and may lead to permanent damage. This presentation (termed HZ ophthalmicus ) occurs when the nasociliary branch is involved and accordingly presents with cutaneous involvement of the nasal tip (Hutchinson sign). This important sign should not be overlooked and should prompt rapid diagnosis, referral, and institution of therapy.
HZ of the maxillary division of the trigeminal nerve produces vesiculation of the palate, uvula, and tonsillar area. Involvement of the mandibular division produces vesicular involvement of the anterior aspects of the tongue, floor of the mouth, lips, and buccal mucous membranes. Involvement of the geniculate ganglion produces lesions on the tongue, ear, and skin of the auditory canal. When accompanied by Bell palsy and disturbances of hearing and equilibrium, it is part of the Ramsay Hunt syndrome.
The diagnosis of HZ is often a clinical one, and in typical cases further evaluations are generally unnecessary. In patients in whom diagnostic confirmation is indicated, direct detection with fluorescent antibody stains of vesicle-base scrapings is useful. Viral culture can be used, but VZV may take up to 1 week to induce cytopathic changes. PCR studies are not available on a widespread basis for clinical use, and serologic studies are generally not useful in this setting.
Treatment for HZ consists of symptomatic measures and specific antiviral therapy ( Table 15-2 ). Symptomatic care includes wet compresses, drying lotions (i.e., calamine), antihistamines, and analgesics. High-dose acyclovir decreases vesicle formation, time to crusting, and days of pain when instituted within 72 hours of onset of the exanthem. Acyclovir should be administered via the intravenous route in immunocompromised patients, given their greater severity of disease, or in any patient with disseminated or severe infection. Other antiviral options in immunocompetent patients or those with uncomplicated HZ include valacyclovir and famciclovir. An HZ vaccine is approved for adults 50 years of age and older, with widespread vaccination desirable to help in the prevention of HZ and PHN in this population and in reducing the health and financial costs of HZ. This vaccine is nearly identical to the varicella vaccine, except that the HZ vaccine contains 14 times as many virus particles.
| Drug | Formulation | Regimen | Indication/Comment |
|---|---|---|---|
| Acyclovir | 200 mg capsule | A: ≥2 years | |
| 400 mg, 800 mg tablet | |||
| 200 mg/5 mL susp | 800 mg 5 times/day | Adult dose; 7-10 days | |
| Pediatric HZ dosing: NE | |||
| 50 mg/1 mL IV | 60 mg/kg per day | IC <12 years; divide every 8 hours; 7 days | |
| 30 mg/kg per day | IC ≥12 years; divide every 8 hours; 7 days | ||
| Famciclovir | 125, 250, 500 mg tablet | 500 mg 3 times/day | A: ≥18 years; 7 days |
| Valacyclovir | 500 mg, 1 g caplet | 1 g 3 times/day | A: adults; 7 days |
* Approved indications and regimens listed; often used off-label.
Viral-Like Disorders of the Oral Mucosa
Aphthous Stomatitis
Recurrent aphthous stomatitis (RAS; aphthous ulcers, canker sores) is one of the most common painful diseases affecting the oral mucosa of children. It has been reported in 5% to 25% of the general population, and there may be a genetic predisposition. The etiology is not well understood, and treatment has traditionally been symptomatic. Aphthous stomatitis presents with single or multiple shallow erosions or ulcerations ( Fig. 15-15 ) on the labial and buccal mucosae, gingivae, tongue, floor of the mouth, palate, or pharynx. Before the onset of the lesions, a tingling sensation may be present. After 24 to 48 hours, a focal erythema develops, followed soon thereafter by tiny, superficial gray-white erosions. Usually there are 1 to 3 lesions (minor RAS; 80% to 85% of cases), and the area of erosion increases and evolves into one or more sharply defined shallow ulcers covered by gray membranes and surrounded by sharp borders and slightly elevated, bright red areolae. Lesions usually measure 3 to 6 mm in diameter, and if left untreated, persist for 8 to 12 days (sometimes longer) and heal without scarring. Occasionally patients develop larger ulcerations, up to several centimeters in size with prolonged pain, fever, and healing with scarring. This variant has been termed major RAS (10% of cases; formally known as Sutton disease) and may be associated with dysphagia, malaise, and HIV infection. Another form of aphthae, herpetiform RAS, occurs in 5% to 10% of patients with aphthous lesions and presents as clusters of pinpoint ulcers that simulate but are not caused by infection with HSV.

Aphthous stomatitis is believed to be multifactorial in origin and may occur in response to a variety of triggering factors, including stress, trauma, hormonal changes, and infection. Cytokines are felt to play an important role, and polymorphisms in the genes for interleukins (ILs) lb and 6 may increase a patient’s individual risk of RAS. Human leukocyte antigen (HLA) B52 and HLA-B44 antigens were found to be strongly associated with RAS in Israeli Arab youths. Drug-induced RAS has also been suggested, especially in association with nonsteroidal anti-inflammatory drugs and β-blockers. Both EBV and CMV have been hypothesized as potential infectious causes of RAS. In the vast majority of cases, the etiology remains unknown.
The differential diagnosis (and/or potential associations) of RAS includes Behçet syndrome (see Chapter 25 ), inflammatory bowel disease (see Chapter 25 ), cyclic neutropenia, gluten-sensitive enteropathy, herpes simplex infection, candidiasis, vitamin/nutritional deficiencies (iron, folic acid, zinc, and vitamins B 1 , B 2 , B 6 , and B 12 ), and the syndrome of periodic fever, aphthous stomatitis, pharyngitis, and cervical adenitis (PFAPA, Marshall syndrome) (see Chapter 25 ). PFAPA syndrome is characterized by high fevers (up to 41° C), aphthous ulcers, pharyngitis (which is usually culture-negative), and cervical adenitis. Associated symptoms include headache, nausea, vomiting, and abdominal pain. The syndrome usually occurs in patients younger than 5 years of age, and flares recur at 21- to 42-day intervals. The fevers resolve over 24 to 48 hours spontaneously and often drop dramatically after even a single dose of oral corticosteroids. Other reportedly effective therapies have included cimetidine and tonsillectomy. Overall, patients with PFAPA syndrome do well with spontaneous resolution of the episodes within 3 to 5 years and without any long-term sequelae.
Treatments for RAS include primarily topical corticosteroids and topical and/or oral analgesics. Topical clobetasol, a potent corticosteroid, in a denture paste or oral analgesic base and applied two to three times daily often results in remission and symptomatic relief. Mixtures of diphenhydramine elixir and Kaopectate or Maalox have been used successfully, as have a variety of medical mouthwashes (i.e., chlorhexidine [Peridex] antibacterial oral rinse). Patients with severe manifestations of RAS may respond to the oral corticosteroids (usually short course) colchicine, thalidomide, or dapsone. Multivitamin administration has not been demonstrated useful in reducing the frequency or duration of RAS episodes.
Acute Necrotizing Gingivitis
Acute necrotizing gingivitis (acute necrotizing ulcerative gingivitis, trench mouth, Vincent stomatitis, Vincent angina) is a painful ulcerative disorder that chiefly affects adolescents and young adults. A related disorder termed noma (see Chapter 14 ) occurs when the infection spreads beyond the gingiva to involve other oral mucosal surfaces. Although acute necrotizing gingivitis was formerly common in schools and military establishments, it is quite rare in the United States and Western Hemisphere, perhaps owing to improved oral and dental care. The cause of acute necrotizing gingivitis is often a mix of bacterial pathogens, including Fusobacterium , Prevotella , Actinomyces , and Bacteroides species and spirochetes. The condition occurs most commonly in patients with predisposing conditions such as malnutrition, poor oral hygiene, ethanol or tobacco use, or immunosuppression.
Clinical findings consist of painful gingivae that bleed easily and an inflamed, eroded, hemorrhagic oropharynx. Ulcerations are most common at the gingival margins and interdental papillae. The ulcers are covered by a grayish-white slough or pseudomembrane that can be removed, leaving behind a raw bleeding surface. Single or multiple papillae may be involved, and the ulceration can be very extensive. Associated features include lymphadenopathy, pain, bleeding of the gums, fever, and a foul breath odor. Treatment of acute necrotizing gingivitis consists of debridement by a dentist or periodontist and broad-spectrum antibiotic therapy, usually penicillin, clindamycin, or erythromycin. Chlorhexidine or saltwater oral rinses may help alleviate discomfort. Attention to good oral hygiene and nutritional rehabilitation (where indicated) are important steps in prevention.
Warts
Warts (verrucae) are a common viral infection of the skin and mucosae caused by the human papillomavirus (HPV). These benign intraepidermal tumors most commonly occur in children and young adults, and their incidence has been estimated at 10%. However, in a recent cross-sectional study of 1465 primary schoolchildren, 33% had warts, so this figure may be an underestimate. Although harmless and often self-involuting over years, warts are occasionally painful and may carry a negative social stigma. In addition, HPV may be associated with cutaneous and genital oncogenesis, particularly in immunosuppressed individuals.
There are four basic types of warts: verruca vulgaris, verruca plana, verruca plantaris, and condyloma acuminatum. Each of these will be discussed individually in the following sections. Most warts occur on the hands, fingers, elbows, and plantar surfaces of the feet. Patients with warts commonly autoinoculate themselves inadvertently with the subsequent appearance of multiple secondary lesions. A classic feature of cutaneous warts is that of koebnerization, whereby a linear constellation of lesions develops along the path of excoriation ( Fig. 15-16 ).

HPV is transmitted via skin-to-skin contact or from fomites, where recently shed viruses may survive if the environment is warm and moist (i.e., locker room floors, pool decking, showers). The entry site is often an area of recent trauma or a skin region with subclinical abrasion or fissuring. Recently it has been shown that important environmental risk factors include having family members with warts and wart prevalence in classrooms, suggesting that preventive recommendations should perhaps focus on these sources more than public places. The incubation period from inoculation to development of the wart may range from 1 to 6 months or more. Although the duration of warts is variable, one study documented that two-thirds of lesions resolve spontaneously within 2 years. The most important mechanism in wart regression appears to be cell-mediated immunity, with cytokines released by keratinocytes or immune-system cells and inducing an immune response against HPV.
Over 130 HPV types comprise this family of small double-stranded DNA viruses, and the various HPV types have been divided into two groups: cutaneous and mucosal. Mucosal types are recovered mainly in the genital tract, although other mucosae may be infected, including the respiratory tract, nose, conjunctiva, and mouth. Although the same HPV virus can cause various types of warts, there is often a correlation between the virus type and the clinical/morphologic characteristics of the lesions it causes. For instance, HPV types 1, 2, 4, and 7 are often associated with common warts (verrucae vulgaris); type 1 with deep palmar and plantar warts; types 3, 10, 28, and 41 with flat warts; types 5, 8, 17, and 20 (among others) with the autosomal recessive disorder epidermodysplasia verruciformis (EV) (see later); and types 6 and 11 with respiratory, conjunctival, and genital infection. In addition, HPV types associated with a high risk for cervical cancer include 16, 18, 31, 33, 35, 39, and 45, among others. HPV types 16 and 18 are the most common high-risk types found in the female anogenital system and are seen in up to 70% of women with cervical cancer. In a study of HPV types and their relationships to patient characteristics, the most distinct clinical profile was noted with HPV 1, which was associated with infection in children younger than 12 years of age, plantar location, a duration of less than 6 months, and patients with fewer warts. Laboratory diagnosis of HPV skin infection is usually unnecessary, and the diagnosis usually straightforward. In instances where identification of the HPV type is necessary, options include nuclear-acid hybridization assays via Southern blotting, dot blots, RNA and DNA probes, and PCR studies. HPV genotyping on swabs of the overlying skin using a novel PCR assay was shown to be a simple and highly sensitive approach to typing.
Verrucae Vulgaris
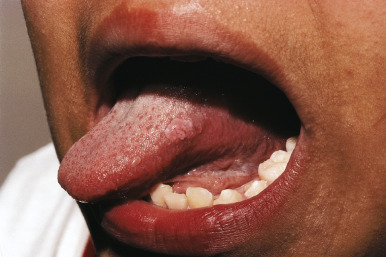
Verrucae vulgaris (common warts) occur predominantly on the dorsal surface of the hands or periungual regions but may be seen anywhere on the cutaneous surface. Occasionally they may also occur on the oral mucosa. Common warts may occur as single or multiple lesions. They clinically present as flesh-colored, verrucous (rough surfaced) papules that may be dome-shaped ( Fig. 15-17 ), exophytic ( Fig. 15-18 ), or filiform (i.e., having a stalk; Fig. 15-19 ). Individual lesions may coalesce into larger plaques ( Fig. 15-20 ). “Ring warts” may occur after overly aggressive therapies and are another example of koebnerization ( Fig. 15-21 ). Oral lesions present as small, pink-white, soft papules and plaques of the labial, lingual ( Fig. 15-22 ), buccal, or gingival mucosa. In Heck disease, multiple verrucous papules occur in a similar mucosal distribution ( Fig. 15-23 ).






Periungual and subungual verrucae ( Figs. 15-24 and 15-25 ) occur around and beneath nailbeds, particularly on the fingers of cuticle pickers and nail biters. These lesions, because of their location and susceptibility to trauma, often become irritated, infected, or tender and are often more resistant to therapy. Satellite lesions may appear, particularly near warts that have been irritated, manipulated, or incompletely treated. When the diagnosis of verruca is in doubt, gentle paring with a number 15 scalpel blade will reveal characteristic punctate black dots that represent thrombosed capillaries ( Fig. 15-26 ).



Verrucae Plana
Verrucae plana (flat warts) occur primarily on the face, neck, arms, and legs. They are usually seen as smooth, flesh-colored to slightly pink or brown, flat-topped papules measuring 2 to 5 mm in diameter (see Fig. 15-16 ; Figs. 15-27 and 15-28 ). They vary from a few lesions to several hundred in any given individual. They may appear in the bearded areas of men and on the legs of women, because irritation from shaving tends to cause their spread. Contiguous warts may coalesce to form larger, plaque-like lesions. Again, linear arrangements of the papules in areas of scratching (koebnerization) are characteristic (see Fig. 15-16 ; Fig. 15-29 ).



Verrucae Plantaris
Verrucae plantaris (plantar warts) occur on the plantar surfaces of the feet and tend to be the most symptomatic type of warts as well as a therapeutic challenge. They usually occur on the weight-bearing areas of the heels, toes, and midmetatarsal areas ( Fig. 15-30 ). Because of the pressure of walking, the lesions often develop an endophytic component and are very painful and tender. Coalescence of multiple lesions may result in mosaic warts ( Fig. 15-31 ). It may occasionally be difficult to differentiate plantar warts from corns or calluses. Corns are localized hyperkeratoses that form over interphalangeal joints as the result of intermittent pressure and friction. Penetrating corns often appear at the base of the second or third metatarsal–phalangeal joint. They can be distinguished from plantar warts by the lack of thrombosed capillaries after paring and by their characteristic hard core. Soft corns are macerated hyperkeratotic lesions that persist at points of friction and pressure in intertriginous areas. They are usually seen on the lateral aspect of the toes or in the web spaces between the fourth and fifth toes.


Black heel (talon noir, calcaneal petechiae) is a common condition that is often confused with plantar warts. In this disorder, superficial dermal capillaries are ruptured by the shearing action associated with sudden stops in athletic individuals, usually tennis, racquetball, or basketball players. Clinically it is characterized by clusters of brown or blue-black pinpoint petechial macules in the horny layer along the backs or sides of the heels or lateral edges of the feet. Gentle paring of the surface with a number 15 scalpel blade can help differentiate this condition from malignant melanoma, calluses, corns, and plantar warts.
Condylomata Acuminata
Condylomata acuminata (anogenital warts, anogenital HPV) are HPV-induced lesions of the anogenital tract and one of the most common STDs. The diagnosis of condylomata acuminata in a child is fraught with anxiety for parents and practitioners alike, and the implications regarding sexual abuse versus benign transmission are controversial and often unclear. Although condylomata often occur after sexual contact, other modes of acquiring the infection include vertical (perinatal) transmission, benign (nonsexual) heteroinoculation, and autoinoculation. In addition, fomite spread is another potential mode of transmission.
Condylomata acuminata present most commonly in the perianal area as flesh-colored, soft, verrucous papules ( Fig. 15-32 ) measuring 1 to 5 mm in diameter. The lesions are usually multiple, and “mirror image” lesions may be noted on each side of the anus. Other areas of involvement include the glans penis, penile shaft, scrotum, and vulva. Vaginal and cervical involvement are appreciable only with internal examination. Occasionally, lesions may enlarge rapidly and present as large, exophytic, cauliflower-like masses ( Fig. 15-33 ). Childhood condylomata are usually incidentally noted during diaper changes, toileting, bathing, or physical examinations. The lesions are usually asymptomatic, but irritation, bleeding, and pain may occur. The differential diagnosis of condylomata acuminata includes MC, epidermal nevus, skin tag, and pseudoverrucous papules and nodules. Infantile perianal pyramidal protrusion is a pyramid-shaped, flesh-colored to pink soft-tissue swelling ( Fig. 15-34 ) that appears in the medial raphe of girls and may represent a peculiar form of lichen sclerosus et atrophicus. The distribution, appearance, and solitary nature of this lesion should distinguish it from condylomata.